The question of whether COVID-19 vaccines affect antibody test results has sparked considerable interest and debate. Antibody tests, designed to detect the presence of antibodies produced in response to a SARS-CoV-2 infection, are often used to assess prior exposure to the virus. However, with the widespread rollout of COVID-19 vaccines, concerns have arisen about whether vaccination could interfere with these test results. Vaccines, particularly mRNA and viral vector types, stimulate the immune system to produce antibodies against the virus’s spike protein, which may be detected by certain antibody tests. This overlap raises questions about the accuracy of interpreting test results, especially in distinguishing between vaccine-induced immunity and natural infection. Understanding this interaction is crucial for both individuals seeking clarity on their immune status and public health officials monitoring population immunity.
| Characteristics | Values |
|---|---|
| Effect on Antibody Test Results | COVID-19 vaccines can cause positive antibody test results. |
| Type of Antibodies Detected | Vaccines primarily induce IgG antibodies, which most tests detect. |
| Timing of Test After Vaccination | Antibodies typically appear 1-2 weeks after the first dose. |
| Duration of Detectable Antibodies | Antibodies may remain detectable for several months post-vaccination. |
| Distinction Between Natural Infection and Vaccination | Some tests can differentiate between vaccine-induced and natural infection antibodies (e.g., spike protein vs. nucleocapsid antibodies). |
| Impact on Test Accuracy | Vaccination does not typically interfere with test accuracy but may complicate interpretation. |
| False Positive Risk | Low risk of false positives, but possible in certain cases. |
| False Negative Risk | Unlikely post-vaccination, as vaccines reliably induce antibodies. |
| Test Type Specificity | Rapid tests and lab-based assays may vary in detecting vaccine-induced antibodies. |
| Public Health Implications | Antibody tests post-vaccination are not recommended for immunity assessment. |
Explore related products






What You'll Learn
![]()
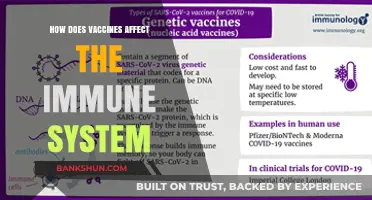
Vaccine type impact on antibody test results
The type of vaccine administered can significantly influence antibody test results, particularly when distinguishing between natural infection and vaccination-induced immunity. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna encode the SARS-CoV-2 spike protein, prompting the body to produce antibodies specific to this antigen. Antibody tests targeting the spike protein will likely yield positive results post-vaccination, reflecting vaccine-induced immunity rather than past infection. Conversely, tests designed to detect nucleocapsid antibodies, which are produced in response to natural infection, may remain negative in vaccinated individuals without prior exposure to the virus.
Consider the practical implications for healthcare providers interpreting antibody test results. A patient vaccinated with a viral vector vaccine, such as Johnson & Johnson or AstraZeneca, may also show spike protein antibodies, as these vaccines deliver genetic material encoding the spike protein. However, the antibody levels and persistence may differ from mRNA vaccines due to variations in dosage and delivery mechanism. For example, a single 0.5 mL dose of Johnson & Johnson may elicit a distinct antibody profile compared to the two-dose regimen of 0.3 mL each for Pfizer-BioNTech. Clinicians must account for these nuances to avoid misinterpreting results, especially when assessing immunity in older adults (65+), who may mount a weaker immune response.
From a comparative standpoint, protein subunit vaccines like Novavax introduce another layer of complexity. These vaccines contain stabilized spike proteins, potentially leading to antibody test results that resemble natural infection more closely than mRNA or viral vector vaccines. This similarity arises because protein subunit vaccines directly expose the immune system to the target antigen, mimicking the viral components present during an actual infection. However, the specificity of the antibody test becomes critical here—tests must differentiate between antibodies generated by the vaccine’s stabilized spike protein and those produced in response to the wild virus.
For individuals seeking clarity on their immune status, understanding vaccine type is essential. If you received an mRNA vaccine and undergo a spike protein antibody test, a positive result confirms vaccination but not necessarily prior infection. To investigate past exposure, request a nucleocapsid antibody test. Additionally, timing matters: antibody levels peak 2–4 weeks post-vaccination but may wane over months, affecting test sensitivity. Repeating the test 6–12 months after vaccination can provide a more accurate assessment of long-term immunity, particularly for those with compromised immune systems or chronic conditions.
In summary, vaccine type dictates the antibody profile detectable in serological tests, requiring careful interpretation to distinguish between vaccine-induced and natural immunity. Healthcare providers and individuals must consider the vaccine’s mechanism, dosage, and timing relative to testing. By doing so, they can ensure accurate results that inform decisions about booster shots, exposure risk, and public health strategies. Always consult a healthcare professional to contextualize antibody test results within your vaccination history and health profile.
Banks Provide Coin Wrappers: Efficient and Time-Saving Service
You may want to see also
Explore related products




![Prime Screen [25 Pack] EtG Alcohol Urine Test - at Home Rapid Testing Dip Card Kit - 80 Hour Low Cut-Off 300 ng/mL - WETG-114](https://m.media-amazon.com/images/I/51MNffSFwAL._AC_UL320_.jpg)

![]()
Timing of vaccination and test accuracy
The timing of vaccination relative to antibody testing can significantly influence test accuracy, particularly for serological assays designed to detect natural infection. Administering an antibody test immediately after vaccination—typically within the first 14 days—often yields negative or inconclusive results, even in fully vaccinated individuals. This occurs because the immune system requires time to mount a detectable antibody response. For mRNA vaccines like Pfizer-BioNTech or Moderna, peak antibody levels are generally observed 2–3 weeks post-second dose, making this window ideal for accurate testing if distinguishing between vaccine-induced and natural immunity is necessary.
Consider a scenario where a healthcare provider needs to determine whether a patient’s antibodies stem from a prior COVID-19 infection or recent vaccination. If the patient was tested within 10 days of receiving the second vaccine dose, the assay might fail to detect sufficient antibodies, leading to a false assumption of no prior infection. Conversely, testing 4–6 weeks post-vaccination increases the likelihood of detecting vaccine-induced antibodies, which could be misinterpreted as evidence of natural infection if the test does not differentiate between antibody types (e.g., anti-spike vs. anti-nucleocapsid antibodies).
To optimize test accuracy, follow these practical steps: First, delay antibody testing for at least 14 days after completing the vaccine series to ensure detectable antibody levels. Second, use assays that differentiate between anti-spike (vaccine-induced) and anti-nucleocapsid (natural infection) antibodies, such as the Roche Elecsys Anti-SARS-CoV-2 S or N assays. Third, for individuals with suspected prior infection, test before vaccination or at least 3 months post-vaccination to minimize cross-reactivity. Adhering to these guidelines reduces the risk of misinterpretation, particularly in populations like healthcare workers or researchers where distinguishing immunity sources is critical.
A comparative analysis of testing timelines reveals that early post-vaccination testing (0–14 days) often underestimates antibody presence, while testing during the peak response phase (21–28 days post-second dose) maximizes detection of vaccine-induced antibodies. However, this window may complicate efforts to identify natural infection in vaccinated individuals. Testing beyond 6 months post-vaccination can be less reliable due to waning antibody levels, though this varies by vaccine type and individual immune response. For instance, older adults or immunocompromised individuals may exhibit lower antibody titers even at peak times, necessitating additional clinical context for interpretation.
In conclusion, the interplay between vaccination timing and antibody test accuracy underscores the need for strategic scheduling and assay selection. Healthcare providers and individuals must consider the purpose of testing—whether to confirm natural infection, assess vaccine response, or both—and align testing timelines accordingly. By understanding these dynamics, stakeholders can avoid common pitfalls, such as false negatives in early post-vaccination testing or misattributing vaccine-induced antibodies to natural infection. This precision ensures that antibody tests remain a valuable tool in both clinical and public health contexts.
PNC Bank: Pending Transactions and Overdrafts
You may want to see also
Explore related products






![]()
False positives or negatives post-vaccination
The COVID-19 vaccine rollout has raised questions about its impact on antibody test results, particularly concerning false positives or negatives. Understanding this interplay is crucial for accurate diagnosis and public health strategies. Antibody tests, designed to detect past infections, may yield unexpected results post-vaccination due to the immune response triggered by the vaccine. This phenomenon warrants a closer examination of the factors contributing to these discrepancies and their implications.
Consider the mechanism of antibody tests, which typically target specific proteins, such as the nucleocapsid (N) or spike (S) proteins. Most COVID-19 vaccines, including Pfizer-BioNTech and Moderna, introduce the S protein to elicit an immune response. Consequently, vaccinated individuals may test positive for S protein antibodies, even without prior infection. However, this does not necessarily indicate a false positive, as the presence of S protein antibodies is an expected outcome of vaccination. The challenge arises when distinguishing between vaccine-induced immunity and natural infection, particularly in seroprevalence studies.
False negatives, on the other hand, may occur in individuals who received vaccines targeting only the S protein, such as the mRNA vaccines. If the antibody test is designed to detect the N protein, a vaccinated individual without prior infection may test negative, despite having vaccine-induced immunity. This scenario highlights the importance of test specificity and the need for clear communication regarding the antigens targeted by both the vaccine and the test. For instance, the Abbott Architect SARS-CoV-2 IgG assay detects the N protein, whereas the Roche Elecsys Anti-SARS-CoV-2 S assay targets the S protein, leading to different results post-vaccination.
To mitigate these issues, healthcare providers should consider the timing of antibody testing relative to vaccination. Testing immediately after vaccination may yield higher antibody levels, potentially confounding results. The CDC recommends waiting at least 90 days post-vaccination before administering an antibody test to minimize false positives. Additionally, using multiplex assays that detect multiple antigens can improve accuracy by differentiating between vaccine-induced and natural immunity. For example, a test that measures both N and S protein antibodies can provide a more comprehensive assessment of an individual’s immune status.
In practical terms, individuals should be informed about the limitations of antibody testing post-vaccination. For those aged 65 and older or immunocompromised, understanding their immune response is particularly vital, as vaccine efficacy may vary. If an antibody test is necessary, consult a healthcare provider to interpret results in the context of vaccination history. Moreover, relying on antibody tests for immunity assessment is not recommended, as the correlation between antibody levels and protection remains unclear. Instead, vaccination status and booster recommendations should guide decisions regarding immunity.
In conclusion, false positives or negatives post-vaccination stem from the interplay between vaccine design, test specificity, and immune response timing. By understanding these factors and adopting strategic testing practices, healthcare providers can ensure more accurate results. Clear communication and informed decision-making are essential to navigate this complex landscape effectively.
Effective Strategies to Monitor and Optimize Your ClickBank Promotions
You may want to see also
Explore related products




![]()
Natural vs. vaccine-induced antibody detection
Antibody tests, designed to detect immune responses, face a unique challenge in distinguishing between antibodies generated by natural infection and those induced by vaccination. This distinction is crucial for epidemiological studies, vaccine efficacy assessments, and individual health evaluations. While both natural infection and vaccines trigger the production of antibodies, the type, quantity, and longevity of these antibodies can differ significantly. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna elicit high levels of IgG antibodies targeting the SARS-CoV-2 spike protein, whereas natural infection produces a broader spectrum of antibodies, including those against the nucleocapsid protein.
To differentiate between these sources, antibody tests must target specific antigens. Tests detecting anti-spike antibodies may indicate vaccination, while those detecting anti-nucleocapsid antibodies suggest natural infection. However, this approach is not foolproof. Some vaccinated individuals may still develop anti-nucleocapsid antibodies if they contract the virus post-vaccination, complicating interpretation. Additionally, the timing of testing matters; antibody levels peak differently after vaccination (typically 2–4 weeks post-second dose) compared to natural infection (2–3 weeks post-symptom onset). Clinicians and researchers must consider these temporal patterns to accurately interpret results.
Practical tips for distinguishing between natural and vaccine-induced antibodies include using multiplex assays that detect both anti-spike and anti-nucleocapsid antibodies simultaneously. For example, the Roche Elecsys Anti-SARS-CoV-2 S assay measures anti-spike antibodies, while the Abbott Architect SARS-CoV-2 IgG assay targets the nucleocapsid protein. Combining these tests provides a clearer picture of an individual’s immune history. However, cost and availability may limit their use in resource-constrained settings. In such cases, a detailed patient history, including vaccination dates and potential exposure to the virus, becomes essential for accurate interpretation.
A comparative analysis reveals that vaccine-induced antibodies often exhibit higher neutralizing activity against specific variants, particularly those targeted by the vaccine (e.g., the original Wuhan strain). In contrast, natural infection may confer broader cross-reactivity due to exposure to multiple viral proteins. This difference has implications for immunity duration and protection against emerging variants. For instance, studies show that hybrid immunity (natural infection plus vaccination) results in higher antibody titers and broader neutralization compared to either alone. Understanding these nuances is critical for public health strategies, such as booster recommendations for different populations.
In conclusion, while antibody tests are valuable tools, their interpretation requires careful consideration of antigen specificity, timing, and clinical context. Distinguishing between natural and vaccine-induced antibodies is not just a technical challenge but a necessity for informed decision-making in healthcare and research. By leveraging targeted assays and integrating patient histories, professionals can navigate this complexity, ensuring accurate assessments of immune status and vaccine efficacy.
Effective Strategies for Complaining About Your Bank Branch Experience
You may want to see also
Explore related products






![]()
Test sensitivity to vaccine-generated antibodies
Vaccine-induced antibodies can indeed influence the results of serological tests, but the extent of this impact varies depending on the test's sensitivity and the vaccine type. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna typically elicit a robust IgG response, which most antibody tests are designed to detect. However, some rapid antigen tests may not differentiate between vaccine-generated and infection-induced antibodies, leading to potential false positives in vaccinated individuals. Understanding this interplay is crucial for accurate interpretation of test results, especially in populations with high vaccination rates.
Analyzing test sensitivity requires examining the assay's ability to detect specific antibody types and their concentrations. For example, the Roche Elecsys Anti-SARS-CoV-2 S assay targets antibodies against the spike protein, a primary component of COVID-19 vaccines. Studies show that this test detects antibodies in 98.9% of vaccinated individuals two weeks post-second dose, with titers peaking at approximately 2,500 U/mL. In contrast, tests targeting the nucleocapsid protein, such as the Abbott Architect SARS-CoV-2 IgG assay, are less likely to cross-react with vaccine-induced antibodies, making them useful for distinguishing between vaccination and prior infection.
From a practical standpoint, healthcare providers should consider the timing of antibody testing relative to vaccination. Antibody levels are lowest immediately after the first dose and peak 2–4 weeks following the second dose. Testing too soon after vaccination may yield false-negative results due to insufficient antibody production. Conversely, waiting at least 14 days post-vaccination ensures a more accurate assessment of the immune response. For individuals aged 65 and older, who may mount a weaker response, repeat testing at 6–8 weeks could provide a clearer picture of antibody persistence.
A comparative analysis of vaccine platforms reveals differences in antibody test sensitivity. Viral vector vaccines like AstraZeneca and Johnson & Johnson produce lower spike protein antibody titers compared to mRNA vaccines, which may result in lower detectability in certain assays. For instance, the DiaSorin Liaison SARS-CoV-2 S1/S2 IgG test shows a 95% sensitivity in mRNA vaccine recipients but only 85% in those who received the AstraZeneca vaccine. This highlights the need for test validation across diverse vaccine types to ensure reliable results.
In conclusion, test sensitivity to vaccine-generated antibodies is a nuanced issue requiring careful consideration of assay design, vaccine type, and testing timing. Healthcare professionals should select tests validated for post-vaccination use and interpret results within the context of vaccination history. For individuals seeking to confirm prior infection, nucleocapsid-specific tests remain the gold standard. As vaccination campaigns continue globally, ongoing research into antibody test performance will be essential to inform public health strategies and individual care decisions.
Contact Access Bank Customer Service: Quick and Easy Methods
You may want to see also
Frequently asked questions
Yes, COVID-19 vaccines can cause a positive result on an antibody test, as they stimulate the production of antibodies against the virus.
An antibody test may show positive results as early as 1-2 weeks after the first vaccine dose, but it typically becomes more consistent after the second dose or a few weeks post-vaccination.
Some antibody tests can differentiate between antibodies produced by vaccination and those from natural infection by detecting specific types of antibodies (e.g., spike protein vs. nucleocapsid protein antibodies).
No, a negative antibody test after vaccination does not necessarily mean the vaccine didn’t work. Antibody levels can vary, and the vaccine primarily provides protection through immune memory, not just detectable antibodies.