Tumor vaccines represent a promising immunotherapeutic approach aimed at harnessing the body's immune system to combat cancer. Unlike traditional vaccines that prevent infectious diseases, tumor vaccines are designed to stimulate an immune response specifically against cancer cells. They exert their antitumor activity by several mechanisms: first, they enhance the recognition of tumor-associated antigens (TAAs) or neoantigens by immune cells, such as T lymphocytes, enabling targeted destruction of cancer cells. Second, they promote the activation and proliferation of effector cells, including cytotoxic T cells and natural killer (NK) cells, which directly eliminate tumor cells. Third, tumor vaccines can modulate the tumor microenvironment by reducing immunosuppressive factors and increasing pro-inflammatory cytokines, thereby creating a more hostile environment for cancer growth. Additionally, they can induce immunological memory, providing long-term protection against tumor recurrence. Through these multifaceted mechanisms, tumor vaccines aim to achieve durable antitumor responses and improve patient outcomes in cancer treatment.
| Characteristics | Values |
|---|---|
| Mechanism of Action | Tumor vaccines primarily exert antitumor activity by activating the immune system to recognize and target cancer cells. They achieve this through antigen presentation, immune cell activation, and modulation of the tumor microenvironment. |
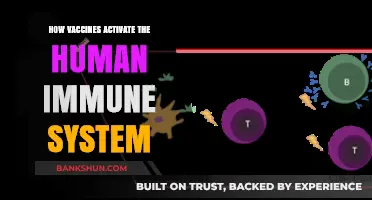
| Antigen Presentation | Vaccines deliver tumor-associated antigens (TAAs) or neoantigens to antigen-presenting cells (APCs), such as dendritic cells (DCs), which process and present these antigens to T cells via MHC molecules. |
| T Cell Activation | Activation of CD4+ and CD8+ T cells, leading to the proliferation of cytotoxic T lymphocytes (CTLs) that directly kill tumor cells and helper T cells that support immune responses. |
| Immune Checkpoint Modulation | Enhancement of immune responses by blocking inhibitory checkpoints (e.g., PD-1, CTLA-4) or promoting stimulatory pathways, thereby overcoming tumor-induced immune suppression. |
| Cytokine Production | Induction of pro-inflammatory cytokines (e.g., IFN-γ, TNF-α, IL-2) that enhance immune cell activity and create a hostile environment for tumor growth. |
| Antibody-Mediated Immunity | Stimulation of B cells to produce antibodies against tumor antigens, leading to antibody-dependent cellular cytotoxicity (ADCC) and complement-mediated lysis of tumor cells. |
| Natural Killer (NK) Cell Activation | Activation of NK cells, which can directly lyse tumor cells and contribute to the overall antitumor immune response. |
| Memory Immune Response | Generation of long-term immune memory, allowing for rapid and effective responses to recurrent or residual tumor cells. |
| Tumor Microenvironment Modulation | Alteration of the tumor microenvironment by reducing immunosuppressive cells (e.g., regulatory T cells, myeloid-derived suppressor cells) and promoting infiltration of effector immune cells. |
| Epitope Spreading | Induction of immune responses against additional tumor antigens not initially targeted by the vaccine, broadening the antitumor immune response. |
| Combination Therapies | Enhanced efficacy when combined with other immunotherapies (e.g., checkpoint inhibitors, CAR-T cell therapy) or conventional treatments (e.g., chemotherapy, radiation). |
| Personalization | Development of personalized vaccines tailored to individual patient tumor mutational profiles (neoantigen vaccines) for improved specificity and efficacy. |
| Safety Profile | Generally well-tolerated with fewer systemic side effects compared to traditional therapies, though local reactions (e.g., injection site pain) and rare immune-related adverse events may occur. |
Explore related products






What You'll Learn
- Antigen Presentation: Enhances immune recognition of tumor-specific antigens by dendritic cells and other APCs
- T Cell Activation: Stimulates cytotoxic CD8+ T cells to target and destroy cancer cells directly
- Immune Checkpoint Modulation: Overcomes tumor immune evasion by blocking inhibitory pathways like PD-1/PD-L1
- Antibody Production: Induces tumor-specific antibodies to mark cancer cells for immune destruction
- Cytokine Release: Promotes pro-inflammatory cytokines (e.g., IFN-γ, TNF-α) to enhance antitumor immunity
![]()
Antigen Presentation: Enhances immune recognition of tumor-specific antigens by dendritic cells and other APCs
Effective tumor vaccines hinge on the ability of antigen-presenting cells (APCs), particularly dendritic cells (DCs), to process and display tumor-specific antigens (TSAs) to T cells. This process, known as antigen presentation, is the linchpin of immune recognition and activation against cancer. Tumor vaccines often deliver TSAs directly or indirectly to APCs, priming them to initiate a robust antitumor immune response. For instance, mRNA-based vaccines encode TSAs, enabling DCs to synthesize and present these antigens on MHC molecules, thereby activating CD4+ and CD8+ T cells. Similarly, peptide-based vaccines deliver TSA fragments directly to APCs, streamlining the presentation process. This targeted approach ensures that the immune system focuses on cancer cells while minimizing off-target effects.
To optimize antigen presentation, tumor vaccines employ strategies that enhance DC maturation and function. Adjuvants, such as TLR agonists (e.g., CpG oligodeoxynucleotides or poly-ICLC), are frequently co-administered to activate DCs, upregulating co-stimulatory molecules like CD80 and CD86. This activation transforms DCs into potent APCs capable of effectively priming naïve T cells. For example, the FDA-approved therapeutic cancer vaccine Provenge (sipuleucel-T) uses autologous DCs loaded with a prostate cancer antigen, fused to a DC-activating factor, to stimulate a patient-specific immune response. Practical considerations include dosing regimens, with adjuvants typically administered at 1–10 mg/kg body weight, depending on the formulation and route of administration.
A critical challenge in antigen presentation is overcoming the immunosuppressive tumor microenvironment (TME), which often impairs DC function. Tumor vaccines address this by incorporating strategies to reverse DC inhibition. For instance, combining vaccines with checkpoint inhibitors (e.g., anti-PD-1 or anti-CTLA-4 antibodies) can restore DC activity by blocking inhibitory pathways. Additionally, vaccines may include cytokines like GM-CSF, which promote DC recruitment and activation within the TME. A notable example is the GVAX vaccine, which genetically modifies tumor cells to secrete GM-CSF, enhancing DC infiltration and antigen uptake at the tumor site. This dual approach—vaccine plus immunomodulation—amplifies antigen presentation and sustains antitumor immunity.
Comparatively, different vaccine platforms vary in their efficiency of antigen delivery to APCs. Viral vector-based vaccines, such as those using adenovirus or lentivirus, excel at targeting DCs due to their inherent immunogenicity. In contrast, cell-based vaccines, like DC vaccines, offer precise control over antigen loading but require complex manufacturing processes. Peptide and protein vaccines are simpler to produce but often necessitate potent adjuvants to ensure adequate DC activation. Each platform has unique advantages, and the choice depends on factors like antigen complexity, patient-specific immune status, and manufacturing scalability. For example, personalized neoantigen vaccines, which target patient-specific mutations, rely on advanced bioinformatics and synthesis techniques to identify and deliver optimal TSAs for presentation.
In practice, enhancing antigen presentation requires a multifaceted approach tailored to the patient and tumor type. Clinicians and researchers must consider the vaccine’s ability to deliver TSAs to APCs, activate DCs, and overcome TME-mediated suppression. For instance, in melanoma patients, combining a peptide vaccine with a TLR3 agonist has shown promise in clinical trials, with dosages of 100–300 μg of peptide and 1 mg of adjuvant administered intradermally every 2–4 weeks. Monitoring DC activation markers (e.g., CD83 or CD86 expression) and T cell responses (e.g., IFN-γ production) can guide treatment adjustments. Ultimately, mastering antigen presentation is key to unlocking the full potential of tumor vaccines, transforming them from experimental therapies into standard-of-care treatments for cancer.
Securely Link MaxRewards Without Sharing Your Bank Password: A Guide
You may want to see also
Explore related products






![]()
T Cell Activation: Stimulates cytotoxic CD8+ T cells to target and destroy cancer cells directly
Cytotoxic CD8+ T cells, often referred to as killer T cells, are the immune system's precision-guided missiles in the fight against cancer. Tumor vaccines harness their destructive potential by presenting cancer-specific antigens, essentially flagging tumor cells for elimination. This process begins with antigen-presenting cells (APCs) engulfing vaccine-delivered tumor antigens and displaying them on their surface MHC class I molecules. Circulating naive CD8+ T cells, each equipped with unique T cell receptors (TCRs), scan these APCs. When a TCR recognizes a tumor antigen-MHC complex, it triggers a cascade of intracellular signals, activating the CD8+ T cell.
This activation transforms the naive T cell into a cytotoxic effector cell, proliferating rapidly and differentiating into a tumor-seeking army. Armed with potent cytotoxic molecules like perforin and granzymes, these effector cells migrate to the tumor site, guided by chemokine signals. Upon encountering cancer cells expressing the target antigen, they form an immunological synapse, a specialized contact zone, and release their cytotoxic payload. Perforin creates pores in the cancer cell membrane, allowing granzymes to enter and initiate apoptosis, a programmed cell death pathway.
The success of this strategy relies on several critical factors. Firstly, the vaccine must deliver antigens that are highly specific to the tumor, minimizing off-target effects on healthy tissues. Secondly, the vaccine formulation should incorporate adjuvants, substances that enhance the immune response by stimulating APCs and promoting T cell activation. Thirdly, the patient's overall immune status plays a crucial role. Pre-existing immunosuppression, often seen in cancer patients, can hinder T cell activation and response.
Combining tumor vaccines with immunomodulatory therapies, such as checkpoint inhibitors, can overcome this hurdle by unleashing the full potential of activated CD8+ T cells.
While the concept of T cell activation by tumor vaccines is promising, challenges remain. Tumors often develop mechanisms to evade immune detection, such as downregulating antigen presentation or creating an immunosuppressive microenvironment. Additionally, achieving sustained T cell responses can be difficult, as effector T cells may become exhausted over time. Ongoing research focuses on developing strategies to overcome these obstacles, including the use of personalized neoantigen vaccines, which target unique mutations specific to an individual's tumor, and combination therapies that enhance T cell persistence and functionality. By refining our understanding of T cell activation and overcoming these challenges, tumor vaccines hold immense potential to revolutionize cancer treatment, offering a targeted and durable approach to combating this complex disease.
Citi Bank High Yield Savings: Rates, Benefits, and Alternatives Explained
You may want to see also
Explore related products






![]()
Immune Checkpoint Modulation: Overcomes tumor immune evasion by blocking inhibitory pathways like PD-1/PD-L1
Tumors employ cunning strategies to evade immune detection, and one of their most effective tactics is hijacking immune checkpoint pathways. These pathways, designed to prevent autoimmune reactions, act as brakes on the immune system. Cancer cells exploit this by expressing proteins like PD-L1, which binds to PD-1 receptors on T cells, effectively shutting them down. This "molecular handshake" allows tumors to fly under the radar, unchecked by the body's natural defenses.
Immune checkpoint modulation disrupts this insidious handshake. By administering antibodies that block PD-1 or PD-L1, we essentially remove the tumor's invisibility cloak. This unleashes the full force of the immune system, allowing T cells to recognize and attack cancer cells with renewed vigor. Think of it as removing the "do not disturb" sign from a hotel room door, allowing the cleaning crew (the immune system) to do its job.
The success of this approach is evident in the remarkable clinical responses seen with checkpoint inhibitors like pembrolizumab and nivolumab. These drugs, administered intravenously every 2-3 weeks, have revolutionized the treatment of various cancers, including melanoma, lung cancer, and kidney cancer. While not a cure-all, they offer significant benefits, with response rates ranging from 20-40% in some cancers, and durable remissions in a subset of patients.
However, checkpoint inhibition isn't without its challenges. By revving up the immune system, these drugs can also trigger autoimmune side effects, ranging from mild skin rashes to more serious conditions like colitis and pneumonitis. Careful patient monitoring and prompt management of these side effects are crucial for maximizing the benefits of this powerful therapy.
Looking ahead, the future of immune checkpoint modulation is bright. Researchers are exploring combination therapies, pairing checkpoint inhibitors with other immunotherapies or traditional treatments like chemotherapy, to further enhance their efficacy. Additionally, efforts are underway to identify biomarkers that can predict which patients are most likely to respond, allowing for more personalized treatment strategies. As our understanding of the intricate dance between tumors and the immune system deepens, immune checkpoint modulation will undoubtedly continue to play a pivotal role in the fight against cancer.
Is Bank of Baroda a Government Bank? Unraveling the Ownership
You may want to see also
Explore related products






![]()
Antibody Production: Induces tumor-specific antibodies to mark cancer cells for immune destruction
Tumor vaccines harness the immune system's precision to target cancer cells, and one of their key mechanisms is the induction of tumor-specific antibodies. These antibodies act as molecular beacons, flagging cancer cells for destruction by immune cells. Unlike broad-spectrum treatments like chemotherapy, this approach is highly selective, minimizing collateral damage to healthy tissues. For instance, the FDA-approved vaccine Sipuleucel-T (Provenge) for prostate cancer stimulates the production of antibodies against prostatic acid phosphatase (PAP), a protein overexpressed in prostate cancer cells, effectively marking them for immune elimination.
The process begins with the vaccine introducing tumor-associated antigens (TAAs) to the immune system. These antigens, often proteins or peptides unique to cancer cells, trigger B cells to differentiate into plasma cells. Plasma cells then secrete antibodies tailored to bind specifically to these TAAs. Once bound, antibodies activate the complement system, a cascade of proteins that can directly lyse cancer cells. Alternatively, they tag cancer cells for phagocytosis by macrophages or engage natural killer (NK) cells via antibody-dependent cellular cytotoxicity (ADCC). Clinical trials have shown that higher titers of such antibodies correlate with improved survival rates, particularly in cancers like melanoma and ovarian cancer.
However, inducing robust antibody production is not without challenges. Tumors often create immunosuppressive microenvironments that hinder B cell activation and antibody secretion. To overcome this, adjuvants like aluminum salts or toll-like receptor agonists are frequently incorporated into vaccines to enhance immune responses. Additionally, combining vaccines with checkpoint inhibitors, such as anti-PD-1 antibodies, has shown promise in boosting antibody production by reversing immune suppression. For optimal results, dosing regimens typically involve priming with 1–3 initial vaccinations followed by booster shots every 3–6 months, tailored to individual immune responses.
A notable example is the HER2-targeted vaccine for breast cancer, which induces antibodies against the HER2 protein, overexpressed in 20–25% of breast cancers. Studies have demonstrated that patients with high anti-HER2 antibody levels post-vaccination exhibit significantly longer progression-free survival. Practical tips for patients include maintaining a balanced diet rich in antioxidants and staying hydrated to support immune function during vaccination. While antibody-based antitumor activity is a powerful tool, it is most effective when integrated into a multimodal treatment plan, combining vaccines with surgery, chemotherapy, or immunotherapy for synergistic effects.
Adding Bank Details to Flipkart: A Step-by-Step Guide for Sellers
You may want to see also
Explore related products






![]()
Cytokine Release: Promotes pro-inflammatory cytokines (e.g., IFN-γ, TNF-α) to enhance antitumor immunity
Cytokine release is a critical mechanism through which tumor vaccines exert their antitumor activity, particularly by promoting pro-inflammatory cytokines like interferon-gamma (IFN-γ) and tumor necrosis factor-alpha (TNF-α). These cytokines act as molecular messengers, orchestrating a robust immune response that targets and eliminates cancer cells. For instance, IFN-γ enhances the cytotoxic activity of T cells and natural killer (NK) cells, while TNF-α induces apoptosis in tumor cells and promotes vascular disruption within the tumor microenvironment. This dual action not only directly attacks cancer cells but also reshapes the immune landscape to favor antitumor immunity.
To harness the power of cytokine release effectively, tumor vaccines often incorporate adjuvants or immunomodulatory agents that stimulate cytokine production. For example, toll-like receptor (TLR) agonists, such as CpG oligodeoxynucleotides or MPL (Monophosphoryl Lipid A), are commonly used to induce IFN-γ and TNF-α secretion. Clinical trials have shown that combining these adjuvants with tumor-specific antigens can significantly enhance vaccine efficacy. A notable example is the Sipuleucel-T vaccine for prostate cancer, which leverages cytokine release to activate antigen-presenting cells and stimulate T-cell responses. Practical considerations include optimizing adjuvant dosage—typically ranging from 100 to 500 μg per administration—to balance immunogenicity and safety, as excessive cytokine release can lead to systemic inflammation.
While cytokine release is a potent driver of antitumor immunity, its effectiveness depends on the tumor microenvironment. Immunosuppressive factors, such as regulatory T cells (Tregs) and myeloid-derived suppressor cells (MDSCs), can dampen cytokine-mediated responses. To counteract this, combination therapies that pair tumor vaccines with checkpoint inhibitors (e.g., anti-PD-1 or anti-CTLA-4 antibodies) are increasingly explored. These inhibitors block immunosuppressive pathways, allowing pro-inflammatory cytokines to exert their full potential. For patients, this approach may require careful monitoring for immune-related adverse events, such as colitis or hepatitis, which can arise from heightened cytokine activity.
A comparative analysis of cytokine-driven tumor vaccines reveals that their success hinges on personalized strategies. Factors like tumor type, mutation burden, and patient immune status influence cytokine responsiveness. For instance, patients with high mutational loads, often seen in melanoma or lung cancer, tend to respond better to cytokine-based vaccines due to increased neoantigen presentation. Conversely, "cold" tumors with low immune infiltration may require additional interventions, such as intratumoral injections of cytokine-inducing agents, to overcome local immunosuppression. Tailoring vaccine design to these variables can maximize cytokine release and improve clinical outcomes.
In conclusion, cytokine release is a cornerstone of tumor vaccine efficacy, with IFN-γ and TNF-α playing pivotal roles in enhancing antitumor immunity. By strategically incorporating adjuvants, combining therapies, and personalizing treatment, clinicians and researchers can leverage this mechanism to combat cancer more effectively. Practical tips include optimizing adjuvant dosages, monitoring for adverse events, and considering the tumor microenvironment to ensure cytokine-driven responses are both potent and safe. As our understanding of cytokine biology deepens, so too will the potential of tumor vaccines to transform cancer treatment.
Discovering the Number of Centennial Bank Locations Across the USA
You may want to see also
Frequently asked questions
Tumor vaccines work by introducing tumor-specific antigens (TSAs) or tumor-associated antigens (TAAs) to the immune system, often combined with adjuvants. These antigens are recognized as foreign by immune cells, such as dendritic cells, which then present them to T cells. Activated T cells, particularly cytotoxic CD8+ T cells, target and destroy cancer cells expressing these antigens, exerting antitumor activity.
Dendritic cells (DCs) are critical in tumor vaccines as they act as antigen-presenting cells (APCs). They capture and process tumor antigens, then migrate to lymph nodes where they present these antigens to T cells. This process primes and activates T cells, enabling them to recognize and attack cancer cells, thus driving the antitumor immune response.
Tumor vaccines enhance immune recognition by presenting tumor antigens in a way that overcomes immune tolerance and evasion. They often include adjuvants or immunomodulatory agents that stimulate a robust immune response, such as activating innate immune pathways or blocking inhibitory signals (e.g., PD-1/PD-L1). Additionally, vaccines can induce immunological memory, allowing for sustained surveillance and elimination of cancer cells.