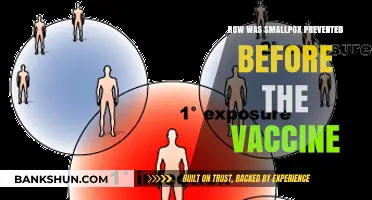
The development of the hepatitis B vaccine is a landmark achievement in medical history, rooted in decades of research and innovation. The journey began in the 1960s when Baruch Blumberg discovered the hepatitis B virus (HBV) and its surface antigen (HBsAg), for which he later won the Nobel Prize. This breakthrough led to the creation of the first vaccine in the 1970s, using HBsAg extracted from the blood of infected individuals. However, this method was risky due to the potential for contamination. A safer approach emerged in the 1980s with the advent of recombinant DNA technology, allowing scientists to produce synthetic HBsAg in yeast cells. This revolutionized the vaccine, making it safer, more scalable, and widely accessible. Today, the hepatitis B vaccine is a cornerstone of global public health, preventing millions of infections and saving countless lives.
| Characteristics | Values |
|---|---|
| Discovery of Hepatitis B Virus | Identified in the 1960s by Baruch Blumberg, who discovered the HBsAg (Hepatitis B surface antigen). |
| Vaccine Development Approach | Utilized recombinant DNA technology to produce the vaccine. |
| Key Component | Hepatitis B surface antigen (HBsAg) derived from yeast or mammalian cells. |
| First Recombinant Vaccine | Approved in 1986, making it the first vaccine produced using genetic engineering. |
| Manufacturing Process | HBsAg protein is synthesized in yeast (Saccharomyces cerevisiae) or Chinese hamster ovary (CHO) cells. |
| Vaccine Types | Plasma-derived (early versions) and recombinant (current standard). |
| Efficacy | Over 95% effective in preventing HBV infection and its chronic consequences. |
| Dosage Schedule | Typically 3 doses over 6 months (0, 1, 6 months). |
| Global Impact | Included in routine infant immunization programs in over 190 countries. |
| Safety Profile | Considered very safe, with mild side effects like soreness at the injection site. |
| Long-Term Protection | Provides immunity for at least 20–30 years, often lifelong. |
| Baruch Blumberg's Contribution | Awarded the Nobel Prize in Physiology or Medicine in 1976 for his work on HBV. |
| Current Status | A cornerstone of global hepatitis B prevention strategies. |
Explore related products






What You'll Learn
- Early research on hepatitis B virus and its transmission
- Identification of surface antigen (HBsAg) as key vaccine target
- Development of plasma-derived vaccine using blood donations in the 1970s
- Transition to recombinant DNA technology for safer, synthetic vaccine production
- Clinical trials, approval, and global distribution of the modern vaccine
![]()
Early research on hepatitis B virus and its transmission
The hepatitis B virus (HBV) was first identified in the 1960s, but its origins and transmission routes remained shrouded in mystery. Early researchers, armed with limited technology, embarked on a detective-like quest to unravel the virus's secrets. One pivotal discovery came in 1965 when Baruch Blumberg, an American scientist, identified the Australia antigen (later renamed hepatitis B surface antigen, or HBsAg) in the blood of an Aboriginal Australian man. This finding marked the first direct link between a specific blood component and hepatitis B, laying the groundwork for understanding its transmission through blood and bodily fluids.
To trace the virus's spread, researchers conducted epidemiological studies in high-risk populations, such as healthcare workers and intravenous drug users. These investigations revealed that HBV was not only transmitted through blood transfusions but also via sexual contact, shared needles, and from mother to child during childbirth. A critical observation was that the virus could persist in the body for decades, often without symptoms, making it a silent but potent threat. By the 1970s, scientists had established that HBV was a global health concern, with over 350 million chronic carriers worldwide, many of whom were unaware of their infection.
One of the most instructive early experiments involved the deliberate (and ethically questionable) injection of HBsAg into chimpanzees, which confirmed the antigen's role in causing hepatitis B. This animal model became essential for studying the virus's lifecycle and testing potential vaccines. Meanwhile, public health campaigns began to emphasize the importance of safe injection practices and blood screening, reducing transmission rates in developed countries. However, the lack of a vaccine left millions vulnerable, particularly in regions with limited access to healthcare.
A key breakthrough came in the 1970s when researchers developed a method to produce HBsAg in large quantities using yeast cells. This innovation paved the way for the first hepatitis B vaccine, approved in 1981. The vaccine, initially derived from the blood of chronic carriers, was later replaced by a safer, recombinant DNA version in 1986. Today, the vaccine is administered in a three-dose series, typically at 0, 1, and 6 months, with a minimum interval of 4 weeks between doses. For infants born to HBV-positive mothers, the first dose is given within 12 hours of birth, followed by additional doses to ensure immunity.
In retrospect, early research on HBV and its transmission was a blend of scientific ingenuity and public health pragmatism. By identifying the virus's unique antigen, tracing its transmission routes, and developing animal models, researchers laid the foundation for a vaccine that has since prevented millions of infections. Practical steps, such as blood screening and safe injection practices, complemented these discoveries, underscoring the importance of both laboratory science and community action in combating infectious diseases.
Is Fifth Third Bank a Visa Member? Unraveling the Partnership
You may want to see also
Explore related products






![]()
Identification of surface antigen (HBsAg) as key vaccine target
The discovery of the hepatitis B surface antigen (HBsAg) marked a pivotal moment in the development of the hepatitis B vaccine. In the 1960s, Baruch Blumberg and his team identified this antigen in the blood of Australian Aboriginal people, initially calling it the "Australia antigen." This finding was serendipitous, as the team was originally studying genetic variations in populations, not viral infections. HBsAg was later recognized as a key component of the hepatitis B virus (HBV), present in the viral envelope and capable of eliciting a strong immune response. This antigen became the foundation for the vaccine, as its identification allowed researchers to focus on a specific target for immune protection.
Analyzing the role of HBsAg, it became clear that this protein was not only a marker of HBV infection but also a critical player in viral replication and persistence. The antigen’s ability to self-assemble into particles resembling the virus, even in the absence of other viral components, was a breakthrough. These particles, known as virus-like particles (VLPs), could stimulate the immune system to produce protective antibodies without the risk of causing infection. This property made HBsAg an ideal candidate for vaccine development, as it offered a safe and effective way to mimic the virus and trigger immunity.
From a practical standpoint, the production of the hepatitis B vaccine involved purifying HBsAg from the blood of chronically infected individuals in the early stages. However, this method posed risks of contamination with other blood-borne pathogens. The advent of recombinant DNA technology in the 1980s revolutionized vaccine production. Scientists inserted the gene encoding HBsAg into yeast or mammalian cells, enabling these organisms to produce the antigen in large quantities. This approach not only eliminated the risk of contamination but also ensured a consistent and scalable supply of the vaccine. Today, the standard dosage for adults is 1–2 micrograms of HBsAg per injection, administered in a series of three shots over 6 months to achieve full immunity.
Comparing the hepatitis B vaccine to others, its reliance on a single antigen highlights the precision of modern vaccinology. Unlike vaccines that require live attenuated or inactivated viruses, the hepatitis B vaccine’s focus on HBsAg allows for a highly targeted immune response. This specificity reduces the likelihood of side effects while maintaining efficacy. For instance, the vaccine is recommended for all infants at birth, with a lower dosage of 5–10 micrograms for children under 20 years old, ensuring safety across age groups. Its success underscores the importance of identifying and isolating key viral components in vaccine design.
In conclusion, the identification of HBsAg as the key vaccine target was a cornerstone in the fight against hepatitis B. Its discovery not only provided a safe and effective means of inducing immunity but also paved the way for advancements in recombinant vaccine technology. Practical considerations, such as dosage adjustments for different age groups and the shift to recombinant production, have made the vaccine accessible and reliable worldwide. This targeted approach serves as a model for future vaccine development, emphasizing the power of isolating and utilizing specific viral antigens.
Secure Your HDFC Account: Step-by-Step Guide to Setting Your IPIN
You may want to see also
Explore related products






![]()
Development of plasma-derived vaccine using blood donations in the 1970s
The development of the hepatitis B vaccine in the 1970s marked a pivotal moment in medical history, leveraging plasma-derived technology from blood donations to combat a pervasive global health threat. At the heart of this innovation was the identification of the hepatitis B surface antigen (HBsAg) in the blood of infected individuals. Scientists discovered that this antigen, when purified and concentrated from donor plasma, could stimulate the immune system to produce protective antibodies without causing the disease itself. This breakthrough laid the foundation for the first hepatitis B vaccine, known as the plasma-derived vaccine.
The process of creating this vaccine was both intricate and labor-intensive. Blood donations from individuals with chronic hepatitis B infection were collected and screened to ensure safety and high HBsAg content. The plasma was then separated, and the antigen was extracted through a series of purification steps, including precipitation, filtration, and chemical treatment. This meticulous process aimed to remove potential contaminants, such as viruses and other blood components, while retaining the immunogenic properties of HBsAg. The purified antigen was then formulated into a vaccine, typically administered in a three-dose series over several months to ensure robust immunity.
One of the critical challenges in developing the plasma-derived vaccine was ensuring its safety. Despite rigorous screening, the risk of transmitting blood-borne pathogens, such as HIV or hepatitis C, remained a concern during the early years of production. To mitigate this, additional safety measures, including heat treatment and detergent inactivation, were introduced to destroy any residual viruses. These steps were essential to build public trust in the vaccine, particularly among high-risk groups like healthcare workers and infants born to infected mothers.
The plasma-derived hepatitis B vaccine represented a significant advancement, but it was not without limitations. The reliance on blood donations made production costly and dependent on a steady supply of infected donors. Additionally, the vaccine’s efficacy varied, with some individuals failing to mount a sufficient immune response. These challenges spurred the development of recombinant DNA technology in the 1980s, which eventually replaced plasma-derived vaccines with safer, more scalable alternatives. Nonetheless, the 1970s plasma-derived vaccine remains a testament to the ingenuity of early vaccine science and its role in paving the way for modern immunization strategies.
For those interested in historical vaccine development, understanding the plasma-derived hepatitis B vaccine offers valuable insights into the evolution of medical technology. Practical takeaways include the importance of antigen purification, safety protocols, and the transition from donor-dependent methods to more sustainable approaches. While no longer in widespread use, this vaccine’s legacy underscores the critical role of blood donations in early medical breakthroughs and the ongoing quest to protect global health.
Why Do Banks Send Letters in All Caps?
You may want to see also
Explore related products






![]()
Transition to recombinant DNA technology for safer, synthetic vaccine production
The development of the hepatitis B vaccine marked a pivotal shift from reliance on human blood products to the adoption of recombinant DNA technology, a transition that revolutionized vaccine safety and production. Early hepatitis B vaccines, derived from the blood of infected individuals, carried inherent risks of contamination with pathogens like HIV and hepatitis C. This method, though effective, was fraught with ethical and safety concerns, prompting the search for a safer alternative.
Recombinant DNA technology emerged as the solution, enabling the production of synthetic vaccines free from human blood components. This process involves inserting the gene for the hepatitis B surface antigen (HBsAg) into yeast or mammalian cells, which then produce the antigen in large quantities. The purified antigen is formulated into the vaccine, eliminating the need for blood-derived materials. This breakthrough not only addressed safety concerns but also scaled up production, making the vaccine more accessible globally.
One of the key advantages of recombinant DNA technology is its ability to produce highly purified and standardized vaccines. For instance, the modern hepatitis B vaccine contains 10–20 micrograms of HBsAg per dose, ensuring consistent immunogenicity across batches. This precision is critical for efficacy, as studies show that a three-dose series of the recombinant vaccine provides over 95% protection in healthy adults and children. The vaccine is administered intramuscularly, with doses spaced at 0, 1, and 6 months, a schedule optimized for robust immune response.
Despite its benefits, the transition to recombinant technology required rigorous testing and regulatory approval. Clinical trials demonstrated the vaccine’s safety profile, with mild side effects like soreness at the injection site reported in less than 10% of recipients. This contrasts sharply with the risks associated with earlier blood-derived vaccines. Additionally, the synthetic vaccine is suitable for all age groups, including infants, who receive their first dose within 24 hours of birth to prevent vertical transmission from infected mothers.
In conclusion, the adoption of recombinant DNA technology for hepatitis B vaccine production exemplifies the power of innovation in addressing public health challenges. By eliminating blood-derived components, this method has not only enhanced safety but also expanded global access to a life-saving vaccine. Practical considerations, such as adhering to the recommended dosing schedule and storing the vaccine at 2–8°C, ensure its effectiveness in preventing hepatitis B infection worldwide. This transition underscores the importance of technological advancements in shaping the future of vaccine development.
Is the Federal Reserve Bank Tax Exempt? Unveiling the Truth
You may want to see also
Explore related products






![]()
Clinical trials, approval, and global distribution of the modern vaccine
The journey of the hepatitis B vaccine from laboratory to global distribution is a testament to rigorous scientific inquiry and international collaboration. Clinical trials, a cornerstone of this process, began in the 1970s, focusing initially on high-risk populations such as healthcare workers and individuals with hemophilia. These trials aimed to assess the vaccine’s safety, immunogenicity, and efficacy in preventing hepatitis B virus (HBV) infection. Early formulations, derived from plasma of chronic carriers, were replaced by recombinant DNA technology in the 1980s, producing a safer, more reliable vaccine. Phase III trials demonstrated that the vaccine was 95% effective in preventing HBV infection, setting the stage for regulatory approval.
Approval of the hepatitis B vaccine followed a meticulous review by regulatory bodies such as the U.S. Food and Drug Administration (FDA) and the World Health Organization (WHO). In 1986, the first recombinant hepatitis B vaccine, Recombivax HB, was licensed in the United States. This milestone was followed by the approval of Engerix-B in 1989. Both vaccines required a three-dose schedule, typically administered at 0, 1, and 6 months, to ensure optimal immune response. The WHO’s prequalification program further validated these vaccines for global use, ensuring they met international standards for safety, efficacy, and quality. This regulatory endorsement paved the way for widespread adoption, but challenges in distribution and accessibility remained.
Global distribution of the hepatitis B vaccine has been a complex endeavor, requiring coordination between governments, NGOs, and pharmaceutical companies. The WHO’s Expanded Programme on Immunization (EPI) played a pivotal role in integrating the vaccine into national immunization schedules, particularly in low-income countries. By 2009, over 170 countries had included the hepatitis B vaccine in their routine childhood immunization programs. However, disparities persist, with coverage rates varying widely across regions. For instance, while high-income countries achieve near-universal coverage, some low-income countries struggle to reach 50%. Practical strategies, such as birth-dose administration (within 24 hours of birth) and combination vaccines, have been implemented to improve uptake and reduce transmission, especially in high-prevalence areas.
A critical aspect of the vaccine’s success lies in its adaptability to diverse populations and settings. For infants, the birth dose is crucial in preventing perinatal transmission, particularly in regions with high HBV prevalence. Adolescents and adults, especially those in high-risk groups, benefit from catch-up vaccination programs. Dosage adjustments, such as higher antigen content for immunocompromised individuals, ensure broader protection. Despite these advancements, ongoing challenges include vaccine hesitancy, supply chain logistics, and the need for sustained funding. The hepatitis B vaccine’s global impact, however, is undeniable: it has reduced chronic infections by over 82% in children under 5, averting millions of cases of cirrhosis, liver cancer, and deaths annually. This underscores the importance of continued efforts to expand access and maintain high vaccination rates worldwide.
Does Mascoma Bank Offer Quest ATM Services? Find Out Here
You may want to see also
Frequently asked questions
The first hepatitis B vaccine was developed by Dr. Maurice Hilleman and his team at Merck & Co. in the late 1960s and early 1970s. It was approved for use in 1981 and became the first vaccine capable of preventing a major human cancer (hepatocellular carcinoma) caused by chronic hepatitis B infection.
The hepatitis B vaccine was created using a groundbreaking method that involved purifying a protein from the surface of the hepatitis B virus (HBsAg) from the blood of infected individuals. Later, a safer and more efficient method was developed using recombinant DNA technology, where yeast or mammalian cells are genetically engineered to produce the viral surface protein without the risk of contamination.
The development of the hepatitis B vaccine was significant because it marked the first vaccine created through genetic engineering and the first to prevent a major human cancer. It also drastically reduced the global burden of hepatitis B, a virus that causes chronic liver disease, cirrhosis, and liver cancer, saving millions of lives worldwide.





![A History of Violence (The Criterion Collection) [4K UHD]](https://m.media-amazon.com/images/I/71lqpbUFtWL._AC_UY218_.jpg)