When comparing vaccines, the question of whether one is better than another depends on various factors, including efficacy, safety, availability, and the specific needs of the population. Different vaccines may offer varying levels of protection against a disease, with some demonstrating higher efficacy rates in clinical trials or real-world settings. Additionally, factors like side effects, dosing schedules, and storage requirements play a crucial role in determining which vaccine might be more suitable for certain individuals or regions. For instance, while one vaccine may provide stronger immunity, another might be more accessible or easier to distribute in low-resource areas. Ultimately, the better vaccine is context-dependent, and decisions should be guided by scientific evidence, public health priorities, and individual circumstances.
Explore related products






What You'll Learn
- Efficacy comparison: Which vaccine provides stronger, longer-lasting immunity against the target disease
- Side effects: Are adverse reactions more frequent or severe in one vaccine
- Dosage requirements: Does one vaccine need fewer doses for full protection
- Storage needs: Is one vaccine easier to store and distribute globally
- Cost difference: Which vaccine is more affordable for mass production and distribution
![]()
Efficacy comparison: Which vaccine provides stronger, longer-lasting immunity against the target disease?
Vaccine efficacy is a critical factor in determining which vaccine offers superior protection against a target disease. For instance, the Pfizer-BioNTech and Moderna mRNA vaccines have demonstrated efficacy rates of approximately 95% in preventing symptomatic COVID-19 in clinical trials, while the Oxford-AstraZeneca vaccine showed around 70-80% efficacy depending on dosing intervals. These numbers, however, only tell part of the story. Efficacy can vary based on factors such as age, immune status, and the circulating virus variants. For example, in older adults, the immune response to vaccines may wane more quickly, making booster doses essential for maintaining protection. Understanding these nuances is key to evaluating which vaccine might provide stronger, longer-lasting immunity for specific populations.
To compare vaccine efficacy, it’s essential to examine real-world data alongside clinical trial results. For instance, studies have shown that while the Johnson & Johnson single-dose vaccine has a lower initial efficacy (around 66-72%), it provides robust protection against severe disease and hospitalization, particularly in regions with high viral transmission. In contrast, mRNA vaccines like Pfizer and Moderna have shown higher efficacy against mild and moderate cases but may require boosters after 6-8 months to maintain optimal protection. Practical considerations, such as storage requirements and dosing schedules, also play a role. For example, the Pfizer vaccine requires ultra-cold storage (-70°C), making it less accessible in certain regions compared to the AstraZeneca vaccine, which can be stored at standard refrigerator temperatures (2-8°C).
When evaluating long-term immunity, the durability of the immune response becomes a focal point. Research indicates that mRNA vaccines tend to elicit higher levels of neutralizing antibodies initially, but these levels decline over time, necessitating boosters. For example, a third dose of the Pfizer vaccine administered 6 months after the initial series has been shown to restore antibody levels and enhance protection against variants like Delta and Omicron. On the other hand, viral vector vaccines like AstraZeneca may induce a more robust T-cell response, which could contribute to sustained protection against severe disease even as antibody levels wane. Age-specific recommendations further complicate the comparison; for individuals over 65, mRNA vaccines are often prioritized due to their higher initial efficacy, while younger populations may have more flexibility in vaccine choice.
A persuasive argument for vaccine selection must also consider the target disease’s characteristics and the population’s needs. For diseases with high mutation rates, such as COVID-19, vaccines that can be quickly adapted to new variants are invaluable. mRNA technology, as seen in Pfizer and Moderna vaccines, allows for rapid modification, making them more future-proof compared to traditional platforms. However, in regions with limited healthcare infrastructure, a single-dose vaccine like Johnson & Johnson may be more practical, despite its lower efficacy, as it simplifies the vaccination process and reduces logistical challenges. Ultimately, the "better" vaccine depends on the specific context—whether prioritizing maximum efficacy, ease of distribution, or long-term immune durability.
In conclusion, comparing vaccine efficacy requires a multifaceted approach that considers clinical data, real-world performance, and practical factors. While mRNA vaccines like Pfizer and Moderna offer higher initial efficacy and adaptability, viral vector vaccines like AstraZeneca and Johnson & Johnson provide viable alternatives, particularly in resource-constrained settings. For individuals, consulting healthcare providers to determine the most suitable vaccine based on age, health status, and local disease prevalence is crucial. Boosters and updated formulations will continue to play a pivotal role in maintaining immunity, ensuring that the chosen vaccine remains effective over time. By weighing these factors, one can make an informed decision about which vaccine provides stronger, longer-lasting protection against the target disease.
Unveiling the Height of Hickstead Derby Bank: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Side effects: Are adverse reactions more frequent or severe in one vaccine?
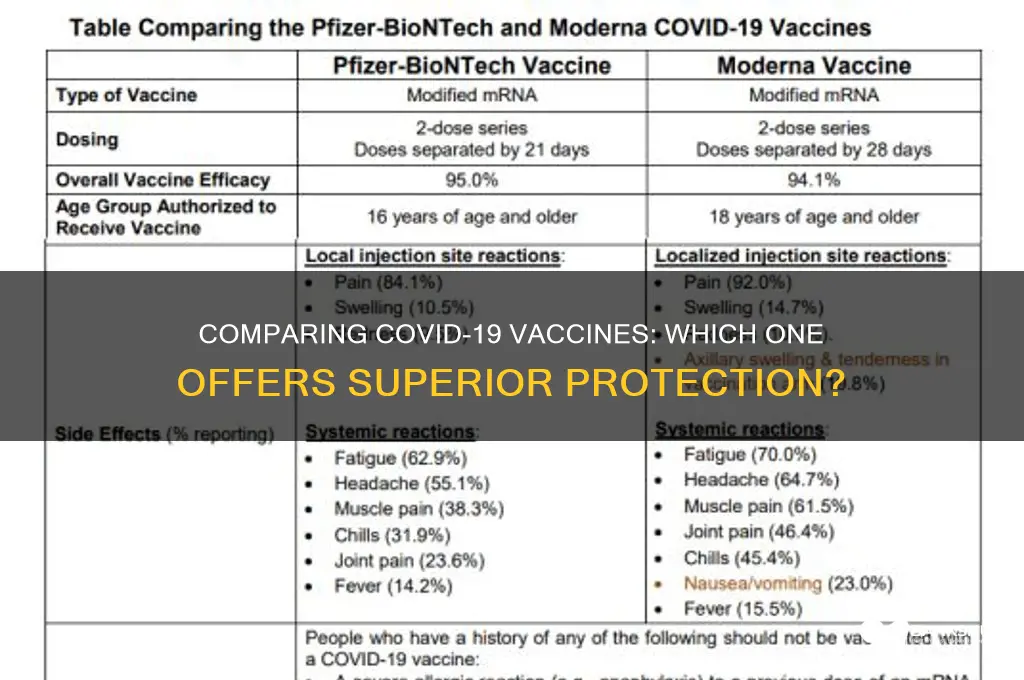
Adverse reactions to vaccines are a critical factor in assessing their comparative safety profiles. While all vaccines undergo rigorous testing, real-world data often reveals nuanced differences in side effect frequency and severity. For instance, the mRNA vaccines (Pfizer-BioNTech and Moderna) have been associated with more frequent systemic reactions, such as fatigue, headache, and muscle pain, particularly after the second dose. These reactions, though uncomfortable, are generally mild to moderate and resolve within a few days. In contrast, the adenovirus vector-based vaccine (Johnson & Johnson) has a lower incidence of systemic reactions but a rare but serious risk of thrombosis with thrombocytopenia syndrome (TTS), particularly in women under 50. Understanding these differences is essential for informed decision-making, especially for individuals with specific health concerns or risk factors.
Analyzing the data, it’s clear that the severity and type of side effects depend on the vaccine’s mechanism of action and the individual’s immune response. For example, the Pfizer-BioNTech vaccine, administered in a two-dose regimen of 30 µg each, often causes more pronounced side effects after the second dose due to a primed immune response. Moderna’s vaccine, with a higher dosage of 100 µg per shot, tends to elicit slightly more intense reactions but follows a similar pattern. On the other hand, the Johnson & Johnson single-dose vaccine, while convenient, carries a unique risk profile that has led to specific usage recommendations, such as prioritizing it for individuals who cannot receive mRNA vaccines or in regions with limited access to multi-dose regimens.
From a practical standpoint, managing side effects effectively can improve the vaccination experience. For mRNA vaccines, over-the-counter pain relievers like acetaminophen or ibuprofen can alleviate symptoms, but it’s advisable to avoid these medications preemptively unless recommended by a healthcare provider, as they may theoretically dampen the immune response. Staying hydrated and resting after vaccination can also help mitigate discomfort. For the Johnson & Johnson vaccine, awareness of TTS symptoms (severe headache, abdominal pain, leg swelling) is crucial, particularly in the first two weeks post-vaccination. Immediate medical attention is necessary if these symptoms arise, as early treatment significantly improves outcomes.
Comparatively, the frequency and severity of side effects should not overshadow the vaccines’ efficacy and safety in preventing severe COVID-19 outcomes. However, for certain populations, such as pregnant individuals or those with a history of blood disorders, the risk-benefit analysis may tilt toward one vaccine over another. Pregnant individuals, for instance, are often advised to receive an mRNA vaccine due to more extensive safety data in this group. Conversely, individuals with a history of severe allergic reactions to polyethylene glycol (PEG), a component of mRNA vaccines, may be better suited for the Johnson & Johnson vaccine. Tailoring vaccine choice to individual health profiles ensures both safety and confidence in the immunization process.
In conclusion, while no vaccine is universally “better” in terms of side effects, understanding the specific risks and reactions associated with each can guide more personalized decisions. Healthcare providers play a pivotal role in this process, offering evidence-based recommendations that balance efficacy, safety, and patient preferences. As vaccination campaigns continue globally, transparency about side effects fosters trust and ensures that individuals can make choices aligned with their health needs. Whether it’s managing mild fever after an mRNA vaccine or monitoring for rare complications with the Johnson & Johnson shot, proactive communication and education remain key to a successful vaccination strategy.
Does Robinhood Offer Instant Bank Transfers? A Quick Guide
You may want to see also
Explore related products


$20.46 $21.95




![]()
Dosage requirements: Does one vaccine need fewer doses for full protection?
The number of doses required for full protection varies significantly across vaccines, and this difference can impact both individual compliance and public health strategies. For instance, the Pfizer-BioNTech COVID-19 vaccine typically requires two doses, administered 3–4 weeks apart for individuals aged 12 and older, while the Johnson & Johnson vaccine offers full protection with a single dose for those aged 18 and above. This disparity in dosage requirements raises questions about convenience, efficacy, and the logistical challenges of vaccine distribution.
From an analytical perspective, the fewer doses a vaccine requires, the simpler it becomes to achieve widespread immunity. Single-dose vaccines like Johnson & Johnson’s eliminate the need for follow-up appointments, reducing barriers such as transportation, time off work, or hesitancy due to multiple injections. However, efficacy must be considered alongside dosage. For example, while the Johnson & Johnson vaccine provides robust protection with one dose, its efficacy rate (around 66–72% against moderate to severe COVID-19) is lower than the two-dose Pfizer vaccine (around 95% after the second dose). This trade-off between convenience and efficacy highlights the importance of tailoring vaccine choice to specific populations and contexts.
Instructively, understanding dosage requirements is crucial for individuals navigating their vaccination options. For parents, the Pfizer vaccine for children aged 5–11 involves a lower dose (10 micrograms per shot) compared to the adult dose (30 micrograms), with two doses administered 3 weeks apart. This age-specific dosing ensures safety and efficacy while maintaining a two-dose regimen. For travelers or those in remote areas, a single-dose vaccine like Johnson & Johnson’s may be more practical, as it eliminates the risk of missing a second appointment. Always consult healthcare providers to determine the most appropriate vaccine based on age, health status, and lifestyle.
Persuasively, the debate over dosage requirements extends beyond individual convenience to public health impact. In low-resource settings or during outbreaks, single-dose vaccines can accelerate immunity and reduce strain on healthcare systems. For example, during the Ebola outbreak in 2019, the single-dose Ervebo vaccine was deployed effectively in the Democratic Republic of Congo, demonstrating the power of simplified dosing in crisis situations. Conversely, two-dose vaccines may require more robust infrastructure and public education campaigns to ensure completion of the series, which can be challenging in underserved communities.
Comparatively, the dosage requirements of vaccines also reflect their design and mechanism of action. mRNA vaccines like Pfizer and Moderna rely on a prime-boost strategy, where the first dose primes the immune system and the second amplifies the response, necessitating multiple doses. In contrast, viral vector vaccines like Johnson & Johnson’s and AstraZeneca’s deliver genetic material in a single, efficient dose, often requiring fewer administrations. This difference underscores the importance of scientific innovation in vaccine development and its direct impact on practical considerations like dosing schedules.
In conclusion, dosage requirements are a critical factor in evaluating whether one vaccine is “better” than another, but the answer depends on context. Fewer doses offer convenience and logistical advantages, particularly in urgent or resource-constrained scenarios, while multiple doses may provide higher efficacy or tailored protection for specific populations. By weighing these factors, individuals and policymakers can make informed decisions that maximize both personal and public health outcomes.
Inside a Blood Bank: Facilities, Equipment, and Lifesaving Operations
You may want to see also
Explore related products






![]()
Storage needs: Is one vaccine easier to store and distribute globally?
One of the most critical factors in global vaccine distribution is storage requirements, which can significantly impact accessibility, especially in low-resource settings. The Pfizer-BioNTech COVID-19 vaccine, for instance, initially required ultra-cold storage at temperatures between -80°C and -60°C, necessitating specialized freezers and a robust cold chain infrastructure. In contrast, the Oxford-AstraZeneca vaccine can be stored at standard refrigerator temperatures (2°C to 8°C), making it far easier to distribute in regions with limited access to advanced cooling equipment. This disparity highlights how storage needs can determine a vaccine’s reach and effectiveness on a global scale.
Consider the logistical challenges of transporting vaccines to remote areas. A vaccine like Moderna’s, which requires storage at -20°C, still demands more sophisticated cold chain management than the Johnson & Johnson vaccine, which can be stored at 2°C to 8°C for up to three months. For humanitarian organizations operating in conflict zones or rural areas, the ability to use existing refrigeration systems—often the same as those used for food—can be a game-changer. This simplicity reduces the risk of spoilage and ensures more doses reach those in need.
From a cost perspective, the storage requirements of a vaccine directly influence its affordability and scalability. Ultra-cold storage not only requires expensive equipment but also increases operational costs, including electricity and maintenance. For example, a single ultra-low temperature freezer can cost upwards of $10,000, a prohibitive expense for many healthcare systems. Vaccines with less stringent storage needs, like the Novavax vaccine (stable at 2°C to 8°C), offer a more cost-effective solution, particularly for low- and middle-income countries.
Practical tips for healthcare providers and distributors include mapping out the cold chain infrastructure in advance and investing in temperature monitoring devices to ensure vaccine integrity. For vaccines requiring ultra-cold storage, dry ice can be used as a temporary solution, but it must be handled carefully to avoid frostbite. Additionally, training staff on proper storage protocols and contingency planning for power outages can mitigate risks. Ultimately, vaccines with simpler storage needs not only reduce logistical burdens but also increase the likelihood of successful immunization campaigns worldwide.
In conclusion, while all vaccines aim to protect public health, their storage requirements play a pivotal role in determining their global impact. Vaccines that can be stored at standard refrigeration temperatures offer a clear advantage in terms of accessibility, cost, and ease of distribution. As the world continues to grapple with vaccine inequity, prioritizing vaccines with less demanding storage needs could be a strategic step toward achieving broader immunization coverage.
Does Canera Bank Accept DigiLock ID for Verification?
You may want to see also
Explore related products






![]()
Cost difference: Which vaccine is more affordable for mass production and distribution?
The cost of producing and distributing vaccines can significantly impact their accessibility, especially in low- and middle-income countries. For instance, the Oxford-AstraZeneca COVID-19 vaccine is priced at approximately $2 to $3 per dose, making it a more affordable option compared to the Pfizer-BioNTech mRNA vaccine, which costs around $15 to $20 per dose. This price difference is largely due to the manufacturing processes involved; AstraZeneca's vaccine uses a modified adenovirus vector, which is less expensive to produce at scale than the lipid nanoparticle technology required for mRNA vaccines.
From a production standpoint, the AstraZeneca vaccine also has logistical advantages. It can be stored and transported at standard refrigerator temperatures (2-8°C), whereas the Pfizer vaccine requires ultra-cold storage (-70°C) until distribution, necessitating specialized equipment and infrastructure. This makes the AstraZeneca vaccine more feasible for mass distribution in regions with limited resources. For example, a rural clinic in sub-Saharan Africa would find it far easier to manage the AstraZeneca vaccine’s storage requirements than those of Pfizer’s.
However, cost-effectiveness isn’t solely determined by production price. Dosage regimens play a role too. The Johnson & Johnson vaccine, priced at around $10 per dose, offers a single-shot regimen, reducing administration costs and logistical complexity compared to the two-dose regimens of AstraZeneca and Pfizer. For mass vaccination campaigns, this simplicity can translate to significant savings in personnel, transportation, and follow-up efforts, particularly in hard-to-reach areas.
When considering affordability for mass distribution, it’s also crucial to factor in intellectual property waivers and technology transfers. For example, the World Health Organization’s COVID-19 Technology Access Pool (C-TAP) has facilitated the sharing of AstraZeneca’s vaccine technology with manufacturers in developing countries, enabling local production and reducing costs further. In contrast, mRNA vaccines have faced more barriers in this regard, though recent initiatives aim to change this.
In practice, governments and health organizations must weigh these cost differences against efficacy, storage requirements, and population needs. For instance, while the AstraZeneca vaccine is more affordable, its slightly lower efficacy against certain variants might prompt a country with higher infection rates to opt for a more expensive but effective option. Conversely, a country with limited healthcare infrastructure might prioritize cost and ease of distribution. Ultimately, the "better" vaccine depends on the specific context, but cost remains a critical factor in ensuring global vaccine equity.
Empowering Conversations: Strategies to Engage Vaccine Skeptics Effectively
You may want to see also
Frequently asked questions
All authorized COVID-19 vaccines have been proven effective in preventing severe illness, hospitalization, and death. While some vaccines may have slightly higher efficacy rates in clinical trials, the best vaccine is the one available to you.
mRNA vaccines and viral vector vaccines both offer strong protection against COVID-19. mRNA vaccines have shown slightly higher efficacy rates in trials, but viral vector vaccines are still highly effective and may be preferred in certain situations, such as for individuals who cannot receive mRNA vaccines.
The number of doses depends on the vaccine’s design, not its overall effectiveness. Single-dose vaccines like Johnson & Johnson are convenient, while two-dose vaccines like Pfizer and Moderna provide robust immunity after the full series. Both options are effective in preventing severe outcomes.
Newer vaccines may be updated to target specific variants, but the original vaccines remain highly effective in preventing severe illness. The choice of vaccine should be based on availability, individual health conditions, and local recommendations.