The question of whether a subunit vaccine is a live vaccine is a common one, often arising from the need to understand the different types of vaccines and their mechanisms. Subunit vaccines, unlike live vaccines, do not contain a live pathogen but instead use specific pieces of the pathogen, such as proteins or sugars, to stimulate an immune response. This key difference means that subunit vaccines cannot cause the disease they are designed to prevent, making them a safer option for individuals with weakened immune systems. Live vaccines, on the other hand, contain a weakened or attenuated form of the pathogen, which can replicate in the body and induce a strong immune response, but also carry a small risk of causing the disease in certain individuals. Understanding these distinctions is crucial for informed decision-making regarding vaccination.
| Characteristics | Values |
|---|---|
| Contains Live Pathogens | No |
| Type of Vaccine | Subunit, Recombinant, Polysaccharide, or Conjugate |
| Immunogenic Components | Specific antigens (protein, polysaccharide, or peptide) from the pathogen |
| Adjuvants | Often required to enhance immune response |
| Risk of Causing Disease | None (cannot replicate or cause disease) |
| Storage Requirements | Typically stable at standard refrigeration temperatures |
| Examples | Hepatitis B vaccine, HPV vaccine, Acellular Pertussis vaccine |
| Immune Response | Primarily humoral (antibody-mediated) immunity, limited cell-mediated immunity |
| Safety Profile | High, suitable for immunocompromised individuals |
| Manufacturing Complexity | High (requires precise antigen isolation or synthesis) |
| Cost | Generally higher compared to live attenuated vaccines |
| Dose Frequency | Multiple doses often required for full immunity |
| Efficacy | High for specific antigens targeted, but may not provide broad immunity |
Explore related products






What You'll Learn
- Definition of Subunit Vaccines: Contains specific antigens, not whole pathogens, to trigger immune response safely
- Live vs. Subunit Vaccines: Live vaccines use weakened pathogens; subunit vaccines use only parts
- Immune Response Differences: Subunit vaccines elicit targeted immunity; live vaccines mimic natural infection
- Safety Profiles: Subunit vaccines are safer, cannot cause disease, ideal for immunocompromised
- Examples of Subunit Vaccines: Includes HPV, Hepatitis B, and acellular pertussis vaccines
![]()
Definition of Subunit Vaccines: Contains specific antigens, not whole pathogens, to trigger immune response safely
Subunit vaccines represent a precision tool in modern immunology, designed to stimulate a targeted immune response without the risks associated with live or whole-pathogen vaccines. Unlike traditional vaccines that use weakened or inactivated pathogens, subunit vaccines contain only specific pieces of the pathogen—such as proteins, peptides, or polysaccharides—known as antigens. These antigens are carefully selected for their ability to trigger a robust immune reaction while eliminating the possibility of causing disease. For example, the hepatitis B vaccine uses a single protein from the virus’s surface, produced through recombinant DNA technology, to safely confer immunity.
The safety profile of subunit vaccines is one of their most compelling advantages, particularly for vulnerable populations. Because they do not contain live pathogens, they cannot revert to a virulent form or cause infection, making them suitable for individuals with compromised immune systems, such as the elderly, infants, or those undergoing chemotherapy. For instance, the acellular pertussis vaccine (DTaP) uses purified antigens from the *Bordetella pertussis* bacterium, reducing the risk of adverse reactions compared to the older whole-cell vaccine. This targeted approach minimizes side effects while maintaining efficacy, often requiring a series of doses (e.g., three to four injections over several months) to build lasting immunity.
However, the specificity of subunit vaccines also presents a challenge: their focused nature can sometimes result in a weaker immune response compared to live vaccines. To compensate, adjuvants—substances like aluminum salts or oil-in-water emulsions—are often added to enhance the immune system’s reaction. For example, the HPV vaccine (Gardasil) includes an aluminum adjuvant to boost its effectiveness. This combination ensures that even though the vaccine contains only a fraction of the pathogen, it still elicits a protective immune memory.
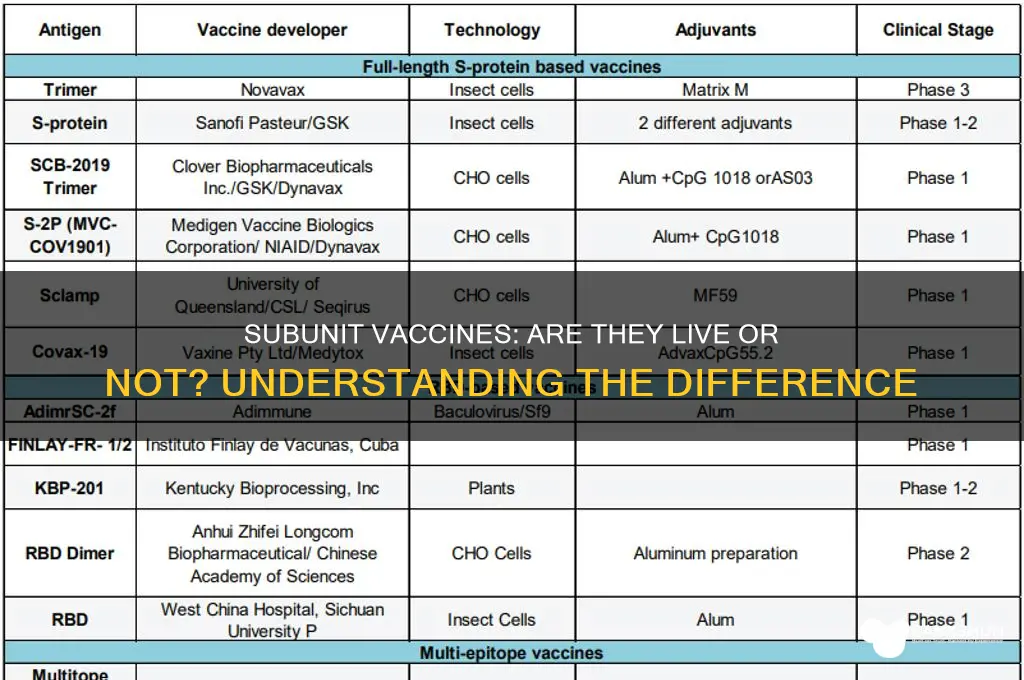
From a practical standpoint, subunit vaccines offer flexibility in administration and storage. Their stability often allows for refrigeration at standard temperatures (2°C–8°C), unlike some live vaccines that require ultra-cold storage. Additionally, they can be administered to individuals with allergies to components of whole-pathogen vaccines, such as egg proteins in the influenza vaccine. The COVID-19 subunit vaccines, like Novavax, exemplify this versatility, using nanoparticle technology to deliver SARS-CoV-2 spike proteins, providing an alternative to mRNA-based options.
In summary, subunit vaccines embody a balance of safety and specificity, leveraging isolated antigens to protect without the risks of live pathogens. While they may require adjuvants or multiple doses to optimize efficacy, their precision makes them invaluable for diverse populations and disease targets. As vaccine technology advances, subunit designs will likely play an increasingly critical role in global health, offering tailored solutions for both emerging and longstanding pathogens.
How Banks Gather Your Data: Privacy Concerns and Collection Methods
You may want to see also
Explore related products






![]()
Live vs. Subunit Vaccines: Live vaccines use weakened pathogens; subunit vaccines use only parts
Live vaccines and subunit vaccines represent two distinct approaches to immunization, each with unique mechanisms and applications. Live vaccines, such as the measles, mumps, and rubella (MMR) vaccine, contain weakened (attenuated) forms of the pathogen. These pathogens are alive but modified to be non-virulent, allowing them to stimulate a robust immune response without causing disease. For instance, the MMR vaccine is administered as a single 0.5 mL dose to children aged 12–15 months, with a second dose at 4–6 years, providing lifelong immunity in most cases. This method mimics a natural infection, often conferring long-lasting immunity with fewer doses.
Subunit vaccines, in contrast, use only specific parts of the pathogen, such as proteins or sugars, to trigger an immune response. Examples include the hepatitis B vaccine, which contains a single viral protein (hepatitis B surface antigen), and the acellular pertussis vaccine, which uses purified components of the *Bordetella pertussis* bacterium. These vaccines are highly targeted, reducing the risk of adverse reactions, and are often recommended for individuals with weakened immune systems. For hepatitis B, a 3-dose series (0.5 mL each) is typically given at 0, 1, and 6 months, with booster doses as needed. Subunit vaccines are safer for immunocompromised populations because they cannot revert to a disease-causing form.
The choice between live and subunit vaccines depends on the pathogen and the population being vaccinated. Live vaccines are particularly effective for viruses like measles, where a strong, broad immune response is essential. However, they are contraindicated in pregnant individuals or those with severe immunodeficiency due to the theoretical risk of the attenuated virus causing disease. Subunit vaccines, while safer, may require adjuvants (e.g., aluminum salts) to enhance immunity and often need multiple doses to achieve comparable protection. For example, the recombinant shingles vaccine (a subunit vaccine) requires two 0.5 mL doses administered 2–6 months apart in adults over 50, whereas the live shingles vaccine is a single dose.
Practically, understanding these differences helps healthcare providers tailor vaccination strategies. Live vaccines are ideal for healthy individuals needing rapid, durable immunity, while subunit vaccines are preferred for vulnerable populations or when safety is paramount. For travelers, live vaccines like yellow fever (a 0.5 mL dose providing lifelong immunity) may be prioritized, whereas subunit vaccines like the recombinant COVID-19 vaccines (e.g., Novavax, 2 doses of 0.5 mL) offer alternatives for those hesitant about live formulations. Always consult vaccination schedules and contraindications to ensure optimal protection.
In summary, live vaccines leverage weakened pathogens for potent immunity, while subunit vaccines use precise components for safety and specificity. Each has its place in modern medicine, with selection guided by pathogen characteristics, patient health, and desired immune outcomes. By understanding these nuances, individuals and healthcare providers can make informed decisions to maximize vaccine efficacy and minimize risks.
Is WSFS Bank Ideal for Small Businesses? Pros, Cons, and Insights
You may want to see also
Explore related products






![]()
Immune Response Differences: Subunit vaccines elicit targeted immunity; live vaccines mimic natural infection
Subunit vaccines and live vaccines differ fundamentally in how they engage the immune system, each with distinct advantages and limitations. Subunit vaccines, composed of specific antigens like proteins or sugars from a pathogen, trigger a highly targeted immune response. For instance, the hepatitis B vaccine contains only the virus’s surface antigen, prompting the body to produce antibodies specifically against this component. This precision minimizes the risk of adverse reactions, making subunit vaccines suitable for immunocompromised individuals or those with specific allergies. In contrast, live vaccines, such as the measles, mumps, and rubella (MMR) vaccine, use weakened forms of the pathogen to mimic a natural infection. This approach stimulates a broader immune response, including both humoral (antibody-mediated) and cell-mediated immunity, closely resembling the body’s defense against a real infection.
The targeted nature of subunit vaccines allows for precise control over the immune response, but it often requires adjuvants—substances like aluminum salts—to enhance effectiveness. For example, the HPV vaccine uses a recombinant protein paired with an adjuvant to ensure robust antibody production. This design typically necessitates multiple doses, such as the three-dose regimen for HPV, to achieve full immunity. Live vaccines, however, often require fewer doses because the weakened pathogen replicates within the body, amplifying the immune signal. A single dose of the yellow fever vaccine, for instance, provides lifelong immunity for most recipients. This efficiency stems from the vaccine’s ability to mimic the duration and intensity of a natural infection, albeit in a controlled manner.
One practical consideration is storage and administration. Subunit vaccines are generally more stable, requiring standard refrigeration (2–8°C), which simplifies distribution in diverse settings. Live vaccines, like the varicella (chickenpox) vaccine, often need stricter cold chain management, such as storage at -15°C, to maintain viability. Additionally, live vaccines carry a small risk of the attenuated pathogen reverting to a virulent form, though this is exceedingly rare. Subunit vaccines eliminate this risk entirely, as they contain no live material. For parents or caregivers, understanding these differences can inform decisions about vaccination schedules, especially for children with underlying health conditions.
From a public health perspective, the choice between subunit and live vaccines depends on the disease and population. Subunit vaccines are ideal for preventing infections where a specific antigen drives immunity, such as tetanus or pertussis. Live vaccines excel in diseases requiring robust, multifaceted immunity, like measles or rotavirus. For travelers, the yellow fever live vaccine offers rapid protection after a single dose, while the subunit hepatitis B vaccine requires planning due to its multi-dose schedule. Ultimately, both vaccine types leverage unique mechanisms to protect against disease, highlighting the importance of tailoring immunization strategies to individual and community needs.
Are Halifax and Lloyds the Same Bank? Unraveling the Connection
You may want to see also
Explore related products






![]()
Safety Profiles: Subunit vaccines are safer, cannot cause disease, ideal for immunocompromised
Subunit vaccines stand out in the realm of immunization for their unparalleled safety profile, primarily because they contain only a fragment of the pathogen—such as a protein or sugar—rather than the entire organism. This design eliminates the risk of the vaccine causing the disease it aims to prevent, a concern that can arise with live-attenuated vaccines. For instance, the hepatitis B vaccine, a subunit vaccine, uses only the virus’s surface antigen (HBsAg), which cannot replicate or cause infection. This makes subunit vaccines inherently safer, particularly for vulnerable populations.
Consider the immunocompromised, a group often excluded from live vaccines due to their weakened immune systems. Subunit vaccines are ideal for this demographic because they pose no risk of viral or bacterial replication. The HPV vaccine, Gardasil 9, is a prime example; it contains virus-like particles (VLPs) that mimic the HPV capsid but lack genetic material, ensuring it cannot cause cervical cancer or warts. Similarly, the COVID-19 subunit vaccines, like Novavax, use recombinant spike proteins, offering robust protection without the risk of SARS-CoV-2 infection. For immunocompromised individuals, this means access to life-saving immunization without compromising their health.
The safety of subunit vaccines extends beyond their inability to cause disease. They are less likely to induce severe adverse reactions compared to live vaccines, which can occasionally trigger mild forms of the illness. For example, the MMR vaccine, a live-attenuated vaccine, rarely causes a mild rash or fever, whereas subunit vaccines like the acellular pertussis vaccine (DTaP) have a lower incidence of fever and swelling at the injection site. This reduced reactogenicity makes subunit vaccines more tolerable, especially for children and the elderly, who may be more sensitive to vaccine side effects.
Practical considerations further highlight the advantages of subunit vaccines. They are stable at higher temperatures, simplifying storage and distribution, particularly in resource-limited settings. Additionally, subunit vaccines often require multiple doses to achieve full immunity, but their safety profile allows for flexible dosing schedules. For instance, the hepatitis B vaccine series typically involves three doses over 6 months, with booster shots recommended for certain high-risk groups. This structured approach ensures long-term protection without the risks associated with live vaccines.
In conclusion, subunit vaccines offer a safety profile that is unmatched by live vaccines, making them a cornerstone of modern immunization strategies. Their inability to cause disease, coupled with reduced adverse reactions, renders them particularly suitable for immunocompromised individuals and other vulnerable populations. As vaccine technology advances, subunit vaccines will likely play an increasingly critical role in global health, providing safe and effective protection against a growing list of pathogens.
Fed Rate Cut: Impact on Banks' Profitability and Lending Strategies
You may want to see also
Explore related products






![]()
Examples of Subunit Vaccines: Includes HPV, Hepatitis B, and acellular pertussis vaccines
Subunit vaccines represent a precision approach in immunization, targeting the immune system with specific components of a pathogen rather than the entire organism. Unlike live vaccines, which use weakened or attenuated forms of the virus or bacteria, subunit vaccines contain only the essential antigens needed to provoke an immune response. This design minimizes the risk of adverse reactions while maintaining efficacy, making them a cornerstone of modern vaccination strategies.
One of the most prominent examples of a subunit vaccine is the Human Papillomavirus (HPV) vaccine. HPV is a leading cause of cervical cancer and other malignancies, and the vaccine targets the virus’s L1 protein, which forms the capsid. Administered in a series of two or three doses depending on age, the HPV vaccine is recommended for adolescents aged 11–12, with catch-up vaccination available through age 26. Its subunit nature ensures safety, as it cannot cause HPV infection, while effectively preventing over 90% of HPV-related cancers.
Another critical subunit vaccine is the Hepatitis B vaccine, which protects against the hepatitis B virus (HBV), a major cause of liver disease. This vaccine uses a recombinant form of the HBV surface antigen (HBsAg), produced in yeast cells. The standard regimen involves three doses over six months, starting at birth for infants, with additional doses for high-risk groups like healthcare workers. Its subunit design eliminates the risk of HBV transmission, making it a safe and effective tool in global hepatitis eradication efforts.
Acellular pertussis (aP) vaccines, part of the DTaP (diphtheria, tetanus, pertussis) combination, illustrate the evolution of subunit vaccines. Unlike the earlier whole-cell pertussis vaccine, which caused significant side effects, aP vaccines contain purified components of *Bordetella pertussis*, such as pertussis toxin and filamentous hemagglutinin. This refinement reduces adverse reactions while maintaining immunity. DTaP is administered in five doses starting at 2 months of age, with boosters recommended throughout life to sustain protection against pertussis, a highly contagious respiratory infection.
These examples highlight the versatility and safety of subunit vaccines. By isolating specific antigens, they offer targeted protection without the risks associated with live vaccines. For instance, the HPV vaccine’s focus on the L1 protein ensures it cannot cause infection, while the Hepatitis B vaccine’s use of HBsAg provides robust immunity without viral exposure. Similarly, the acellular pertussis vaccine’s purified components minimize side effects while effectively preventing disease. This precision makes subunit vaccines ideal for vulnerable populations, including infants and immunocompromised individuals.
In practice, understanding the subunit nature of these vaccines can empower individuals to make informed decisions. For parents, knowing the DTaP vaccine uses purified components may alleviate concerns about side effects. For young adults, recognizing the HPV vaccine’s safety profile can encourage timely vaccination. Healthcare providers can emphasize the absence of live pathogens in the Hepatitis B vaccine to reassure hesitant patients. By focusing on these specifics, subunit vaccines not only exemplify scientific innovation but also serve as practical tools for disease prevention.
Easy Guide to Perform RTGS Transactions via SBI Bank
You may want to see also
Frequently asked questions
No, a subunit vaccine is not a live vaccine. It contains only specific parts (subunits) of a pathogen, such as proteins or sugars, rather than the entire live or weakened pathogen.
A subunit vaccine uses only a fragment of the pathogen to trigger an immune response, while a live vaccine uses a weakened or attenuated form of the entire pathogen. Subunit vaccines cannot cause the disease they protect against.
No, a subunit vaccine cannot cause the disease because it does not contain live or complete pathogens. It only includes harmless components that stimulate the immune system.
Subunit vaccines are generally considered safer than live vaccines, especially for individuals with weakened immune systems, as they cannot replicate or cause the disease. However, safety depends on the specific vaccine and individual health conditions.