The question of whether a vaccine is a cure for coronavirus is a common yet nuanced one. Vaccines are designed to prevent infections by training the immune system to recognize and combat the virus, thereby reducing the likelihood of severe illness, hospitalization, or death. However, they are not a cure for individuals already infected with the virus. Treatment for COVID-19 typically involves managing symptoms, administering antiviral medications, or providing supportive care in severe cases. Vaccines play a critical role in preventing the disease and slowing its spread, but they do not eliminate the virus once it has established an infection. Understanding this distinction is essential for informed decision-making and public health strategies.
| Characteristics | Values |
|---|---|
| Definition | A vaccine is a biological preparation that provides active acquired immunity to a particular infectious disease. It is not a cure but a preventive measure. |
| Purpose | To train the immune system to recognize and combat the virus (e.g., SARS-CoV-2) before exposure, reducing the risk of severe illness, hospitalization, and death. |
| Mechanism | Stimulates the production of antibodies and immune memory cells without causing the disease. |
| Effectiveness | Reduces the likelihood of infection and severity of COVID-19 symptoms but does not guarantee complete prevention (efficacy varies by vaccine type, e.g., 65-95% for approved vaccines). |
| Duration of Protection | Varies; booster doses may be required to maintain immunity (e.g., 6 months to a year for COVID-19 vaccines). |
| Treatment vs. Prevention | Vaccines are prophylactic (preventive) and not therapeutic (curative). Treatment for COVID-19 involves medications like antivirals (e.g., Paxlovid) or monoclonal antibodies. |
| Variants | Effectiveness may decrease against new variants (e.g., Omicron), but still provides significant protection against severe outcomes. |
| Side Effects | Mild to moderate (e.g., soreness, fatigue, fever) and rare severe reactions (e.g., anaphylaxis, myocarditis). |
| Global Availability | Uneven distribution; high-income countries have better access compared to low-income regions. |
| Current Status (2023) | Multiple vaccines approved (e.g., Pfizer-BioNTech, Moderna, AstraZeneca, Johnson & Johnson) with ongoing research for updated formulations. |
Explore related products






What You'll Learn
![]()
Vaccine effectiveness against COVID-19 variants
The emergence of COVID-19 variants has raised critical questions about vaccine effectiveness. While vaccines were initially developed to combat the original strain, their efficacy against mutations like Delta and Omicron has become a central concern. Studies show that vaccines remain highly effective in preventing severe illness, hospitalization, and death across variants, but their ability to prevent infection and transmission has waned over time. For instance, two doses of mRNA vaccines (Pfizer or Moderna) offer approximately 95% protection against severe disease from the original strain, but this drops to around 70-80% against Delta and 50-60% against Omicron. Booster doses, however, significantly restore protection, with a third shot increasing efficacy against severe Omicron outcomes to over 90%.
Analyzing the data reveals a clear pattern: vaccines are not a cure for COVID-19, but they are a powerful tool in reducing its severity. The immune response generated by vaccines targets the spike protein of the virus, which mutates frequently in variants. While these mutations can reduce antibody neutralization, the immune system’s memory cells (B and T cells) provide a robust defense against severe disease. For example, T cells, which are less affected by spike protein mutations, continue to recognize and combat infected cells, preventing progression to critical illness. This explains why vaccinated individuals are far less likely to require hospitalization or intensive care, even when infected with variants.
Practical considerations for maximizing vaccine effectiveness against variants include adhering to recommended dosing schedules and staying updated with boosters. For mRNA vaccines, a primary series of two doses followed by a booster at least 3-6 months later is advised for adults. Immunocompromised individuals may require an additional dose in their primary series. Age-specific recommendations also apply; for instance, children aged 5-11 receive a lower dosage (10 micrograms per shot for Pfizer, compared to 30 micrograms for adults) to balance efficacy and safety. Pregnant individuals are strongly encouraged to get vaccinated, as data shows no safety concerns and significant benefits in preventing severe illness.
Comparing vaccine types highlights differences in effectiveness against variants. mRNA vaccines (Pfizer and Moderna) have demonstrated superior performance compared to viral vector vaccines (AstraZeneca and Johnson & Johnson), particularly against Omicron. However, all approved vaccines provide substantial protection against severe outcomes. In regions with limited access to mRNA vaccines, viral vector options remain a critical tool in controlling the pandemic. Mixing vaccine types (heterologous boosting) has also shown promise, with studies indicating that combining an initial viral vector dose with an mRNA booster can enhance immune responses and broaden protection against variants.
In conclusion, while vaccines are not a cure for COVID-19, their effectiveness against variants underscores their role as a cornerstone of pandemic management. By preventing severe disease and reducing strain on healthcare systems, vaccines have saved millions of lives. Staying informed about variant-specific data, adhering to dosing guidelines, and embracing booster shots are essential steps for individuals and communities. As the virus continues to evolve, ongoing research and global vaccination efforts remain vital in staying ahead of new variants and mitigating their impact.
Is the West Bank Landlocked? Exploring Its Geographic Status and Borders
You may want to see also
Explore related products






![]()
Difference between prevention and cure in vaccines
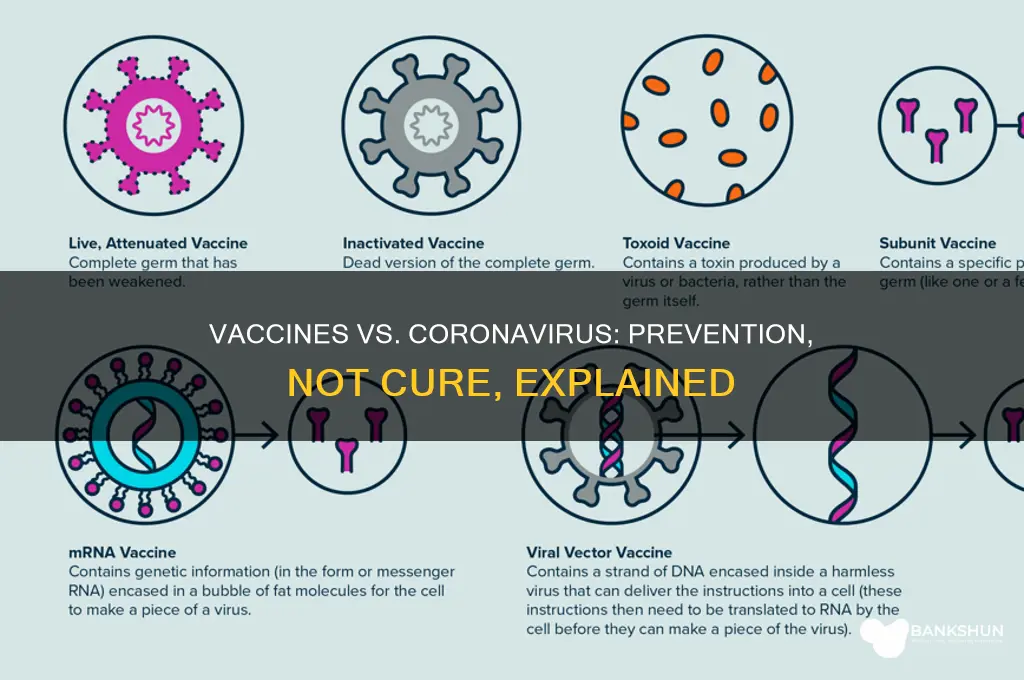
Vaccines are not cures for diseases like COVID-19; they are preventive tools designed to train the immune system to recognize and combat pathogens before infection occurs. This distinction is critical because it shapes how vaccines are developed, administered, and understood in public health strategies. While a cure targets the disease after it has taken hold, often requiring immediate action to alleviate symptoms or eradicate the pathogen, vaccines operate proactively, building immunity to prevent the disease from establishing itself in the first example. For instance, COVID-19 vaccines, such as those by Pfizer-BioNTech and Moderna, require a specific dosage regimen—typically two doses spaced 3–4 weeks apart for mRNA vaccines—to achieve optimal immune response in individuals aged 12 and older.
The mechanism of prevention versus cure is rooted in biology and timing. Vaccines introduce a harmless component of the virus, like the spike protein in COVID-19 vaccines, to stimulate the production of antibodies and memory cells. This process takes weeks, as the immune system needs time to mount a robust response. In contrast, cures, such as antiviral medications, act directly on the virus once it has infected the body, often targeting its replication process. For example, Paxlovid, an antiviral treatment for COVID-19, is prescribed within 5 days of symptom onset to reduce the risk of severe illness, highlighting its reactive nature compared to the proactive approach of vaccines.
From a public health perspective, prevention through vaccination is far more cost-effective and scalable than relying on cures. Vaccines reduce the overall disease burden by lowering transmission rates, hospitalizations, and deaths, thereby alleviating strain on healthcare systems. During the COVID-19 pandemic, countries with high vaccination rates saw significantly fewer severe cases, even as new variants emerged. However, cures remain essential for treating breakthrough infections and vulnerable populations, such as the immunocompromised, who may not respond adequately to vaccines. This dual approach—prevention and cure—is necessary for comprehensive disease management.
Practical considerations further underscore the difference between prevention and cure. Vaccines often require widespread distribution and adherence to dosing schedules, making community engagement and accessibility critical. For instance, mobile vaccination clinics and workplace vaccination drives have been instrumental in reaching underserved populations. Cures, on the other hand, demand rapid diagnosis and treatment, necessitating robust testing infrastructure and supply chains for medications. Patients must follow specific instructions, such as taking Paxlovid every 12 hours for 5 days, to ensure efficacy. Understanding these differences empowers individuals and policymakers to make informed decisions about when and how to use vaccines and cures effectively.
In summary, while vaccines and cures both combat disease, their roles are distinct and complementary. Vaccines prevent infection by preparing the immune system in advance, whereas cures treat active infections by targeting the pathogen directly. Recognizing this difference is essential for maximizing the impact of both strategies in managing diseases like COVID-19. By combining prevention through vaccination with timely treatment options, societies can build resilience against current and future health threats.
Exploring US Bank's Presence in Springfield, Ohio: Facts and Locations
You may want to see also
Explore related products






![]()
Vaccine role in reducing severe illness
Vaccines do not cure COVID-19, but they excel at reducing the risk of severe illness, hospitalization, and death. Clinical trials and real-world data consistently show that vaccinated individuals are far less likely to experience critical outcomes compared to the unvaccinated. For instance, the Pfizer-BioNTech and Moderna mRNA vaccines demonstrated 90-95% efficacy in preventing severe disease in their initial trials, a protection level that remains robust even against many variants. This reduction in severity is particularly crucial for vulnerable populations, such as the elderly and those with comorbidities, who are at highest risk for complications.
Consider the mechanism: vaccines train the immune system to recognize and combat the virus swiftly. Upon exposure, vaccinated individuals mount a faster, more coordinated response, often halting the virus before it causes severe damage. This contrasts with an unvaccinated immune response, which can be slower and less effective, allowing the virus to replicate unchecked and trigger dangerous inflammation. For example, studies show that vaccinated individuals have significantly lower viral loads, reducing the likelihood of progressing to acute respiratory distress syndrome (ARDS) or requiring mechanical ventilation.
Practical tips for maximizing this protective effect include adhering to the recommended dosage schedule. Most vaccines require two primary doses, with a booster dose advised 6-12 months later to maintain immunity. For older adults or immunocompromised individuals, additional boosters may be necessary, as their immune responses can wane more quickly. It’s also critical to monitor local public health guidelines, as recommendations may evolve with new variants or data. Combining vaccination with other preventive measures, like masking in crowded spaces, further reduces risk, especially during surges.
Comparatively, the role of vaccines in reducing severe illness is akin to fortifying a house against a storm. While the house (body) may still face the storm (virus), the reinforced structure (immune system) prevents catastrophic damage. This analogy underscores why vaccines are not a cure but a powerful tool for damage control. For example, in countries with high vaccination rates, such as Portugal or Singapore, COVID-19 shifted from a leading cause of death to a manageable illness, with hospitals no longer overwhelmed by severe cases.
In conclusion, while vaccines do not eliminate the possibility of infection, their impact on reducing severe illness is undeniable. By preventing the virus from overwhelming the body, they transform COVID-19 from a potentially life-threatening disease into a condition that most people can recover from at home. This shift not only saves lives but also alleviates strain on healthcare systems, enabling resources to be directed where they’re most needed. Understanding this role empowers individuals to make informed decisions, protecting themselves and their communities.
Step-by-Step Guide to Creating an IPIN in HDFC Bank Online
You may want to see also
Explore related products






![]()
Duration of immunity post-vaccination
The duration of immunity post-COVID-19 vaccination is a critical factor in determining the long-term effectiveness of these vaccines. Clinical trials and real-world data have shown that the Pfizer-BioNTech and Moderna mRNA vaccines provide robust protection against severe disease for at least 6 months after the second dose. However, immunity begins to wane over time, with studies indicating a gradual decline in antibody levels starting around 4–6 months post-vaccination. This does not mean the vaccines become ineffective, but rather that their ability to prevent mild or moderate infections may decrease, while protection against severe illness and hospitalization remains high.
To address this, health authorities have recommended booster doses for certain populations. For instance, individuals aged 65 and older, residents of long-term care facilities, and those with underlying medical conditions are advised to receive a booster shot 6 months after their initial series. Healthy adults aged 18–64 may also benefit from a booster, particularly if they are at increased risk of exposure or live in areas with high transmission rates. The booster dose, typically a single shot, has been shown to significantly increase antibody levels, restoring protection to levels comparable to those seen shortly after the second dose.
Comparing the COVID-19 vaccines to other vaccines provides context for understanding immunity duration. For example, the influenza vaccine is administered annually due to the virus's rapid mutation and the relatively short duration of immunity it confers. In contrast, vaccines like those for measles or mumps provide lifelong immunity after a two-dose series. COVID-19 vaccines appear to fall somewhere in between, offering strong initial protection that gradually diminishes but remains effective against severe outcomes. Ongoing research is exploring whether additional boosters or updated vaccine formulations will be needed to maintain long-term immunity, particularly as new variants emerge.
Practical tips for maximizing post-vaccination immunity include staying informed about booster recommendations from local health authorities and adhering to public health measures like masking and social distancing, especially in high-risk settings. Monitoring breakthrough infections and vaccine efficacy in real-world scenarios is also crucial for understanding how immunity evolves over time. For those who are immunocompromised, consulting a healthcare provider for personalized advice is essential, as this group may require additional doses or alternative strategies to achieve adequate protection.
In conclusion, while COVID-19 vaccines do not provide indefinite immunity, they offer substantial and lasting protection against severe disease. The duration of this immunity varies, but boosters have proven effective in extending and enhancing protection. As the pandemic continues to evolve, staying proactive and informed about vaccination strategies will remain key to safeguarding individual and public health.
Is BBVA Bank Available in San Antonio, TX? Find Out Here
You may want to see also
Explore related products






![]()
Vaccines vs. treatments for active infections
Vaccines and treatments for active COVID-19 infections serve fundamentally different purposes, yet both are critical in the fight against the coronavirus. Vaccines are designed to prevent infection by training the immune system to recognize and combat the virus before it takes hold. They are administered to healthy individuals, typically in a series of doses—for example, the Pfizer-BioNTech and Moderna mRNA vaccines require two primary shots followed by boosters as recommended by health authorities. These vaccines have proven highly effective in reducing severe illness, hospitalization, and death, particularly among vulnerable populations such as the elderly and immunocompromised. However, vaccines do not cure an active infection; their role is prophylactic, not therapeutic.
In contrast, treatments for active COVID-19 infections aim to alleviate symptoms, shorten the duration of illness, and prevent progression to severe disease. Examples include antiviral medications like Paxlovid, which inhibits viral replication, and monoclonal antibody therapies, which provide immediate immune support. These treatments are typically prescribed for individuals who have already tested positive and are at high risk of complications. For instance, Paxlovid is recommended for adults and children over 12 years old who weigh at least 40 kg, and it must be taken within five days of symptom onset. Unlike vaccines, these treatments are reactive, addressing the virus once it has established itself in the body.
The distinction between prevention and treatment highlights the complementary roles of vaccines and therapies in pandemic management. Vaccines reduce the overall burden on healthcare systems by lowering infection rates, while treatments provide a safety net for those who do become infected. However, the effectiveness of treatments can wane as new variants emerge, necessitating ongoing research and adaptation. For example, some monoclonal antibody treatments have reduced efficacy against Omicron subvariants, underscoring the need for diverse therapeutic options.
Practical considerations further differentiate vaccines from treatments. Vaccines are administered through mass vaccination campaigns, often in community settings, and require cold chain logistics for storage and distribution. Treatments, on the other hand, are typically prescribed by healthcare providers and may require monitoring for side effects, such as Paxlovid’s potential interactions with other medications. Patients must also adhere to specific dosing regimens, which can be challenging for those with limited access to healthcare or health literacy.
In summary, while vaccines and treatments both combat COVID-19, their mechanisms, targets, and applications are distinct. Vaccines prevent infection through immune preparedness, while treatments address active infections to mitigate their impact. Understanding this difference is crucial for individuals and policymakers alike, as it informs decisions about vaccination, treatment access, and public health strategies. By leveraging both tools effectively, societies can better navigate the complexities of the pandemic.
Securely Pay Online: A Step-by-Step Guide to Internet Banking Payments
You may want to see also
Frequently asked questions
No, a vaccine is not a cure for coronavirus. A vaccine helps prevent infection by preparing the immune system to fight the virus if exposed, but it does not treat or cure an existing infection.
No, COVID-19 vaccines are designed to prevent illness, not to treat or cure someone who is already infected. Treatment for COVID-19 involves other medical interventions.
Vaccination reduces the risk of severe illness, hospitalization, and death, but it does not guarantee complete elimination of the virus. The virus may still circulate, especially in unvaccinated populations.
Vaccines are essential because they prevent infection and reduce the severity of illness, protecting individuals and communities. While they don’t cure the virus, they play a critical role in controlling the pandemic and saving lives.