The question of whether a vaccine confers adaptive acquired or passive immunity is central to understanding how vaccines protect against diseases. Vaccines primarily stimulate the body’s adaptive immune system, which involves the production of antibodies and memory cells specific to the pathogen. This process is considered adaptive acquired immunity because it is a long-lasting, active response developed by the individual’s immune system after exposure to a vaccine antigen. In contrast, passive immunity involves the transfer of pre-formed antibodies from an external source, such as through maternal antibodies or antibody injections, which provide immediate but temporary protection. While vaccines do not confer passive immunity, they can indirectly lead to passive protection in populations through herd immunity. Thus, vaccines are a cornerstone of adaptive acquired immunity, equipping the body to recognize and combat pathogens more effectively upon future encounters.
| Characteristics | Values |
|---|---|
| Type of Immunity | Adaptive (Acquired) |
| Mechanism | Stimulates the immune system to produce antibodies and memory cells |
| Duration | Long-term (months to years, depending on the vaccine) |
| Specificity | Specific to the pathogen targeted by the vaccine |
| Natural vs. Artificial | Artificial (induced by vaccination) |
| Passive Involvement | No passive immunity; active immune response is triggered |
| Examples | MMR (Measles, Mumps, Rubella), Influenza, COVID-19 vaccines |
| Memory Response | Yes, memory cells provide rapid response upon future exposure |
| Immediate Protection | No, takes time (usually weeks) for immunity to develop |
| Booster Requirement | Often requires boosters to maintain immunity |
| Contrast with Passive Immunity | Passive immunity is short-term and involves direct transfer of antibodies (e.g., from mother to baby or via antibody injections) |
Explore related products





What You'll Learn
![]()
Vaccine-induced immunity type
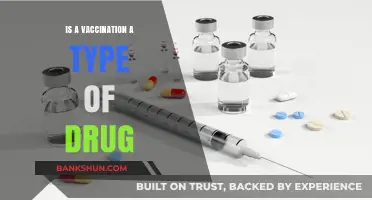
Vaccines are a cornerstone of modern medicine, but understanding the type of immunity they confer is crucial for appreciating their role in public health. Vaccine-induced immunity is adaptive and active, a fact that distinguishes it from passive immunity. Unlike passive immunity, which is acquired through the transfer of antibodies (such as from mother to child via breast milk or via antibody injections), adaptive immunity is a learned response by the body’s immune system. When a vaccine is administered, it introduces a harmless form of a pathogen (or its components) to the immune system, triggering the production of memory cells and antibodies. This process primes the body to recognize and combat the actual pathogen if exposed in the future. For instance, the measles, mumps, and rubella (MMR) vaccine contains weakened viruses that stimulate the immune system without causing disease, leading to long-term protection.
To illustrate, consider the COVID-19 mRNA vaccines, which provide a fascinating example of adaptive immunity in action. These vaccines deliver genetic material that instructs cells to produce a harmless piece of the SARS-CoV-2 spike protein. The immune system identifies this protein as foreign, prompting the production of antibodies and the activation of T cells. This response not only neutralizes the protein but also creates memory cells that persist for months or years. Studies show that after a two-dose regimen (typically 3–4 weeks apart for Pfizer-BioNTech and Moderna), individuals develop robust immunity, with efficacy rates initially exceeding 90% against symptomatic infection. Booster doses, administered 6–12 months later, further enhance this adaptive response by reactivating memory cells and increasing antibody levels, particularly against emerging variants.
While adaptive immunity is powerful, it is not instantaneous. After vaccination, it takes approximately 1–2 weeks for the immune system to begin producing antibodies and several more weeks to establish full protection. This delay underscores the importance of adhering to recommended vaccine schedules. For example, the influenza vaccine is typically administered annually in the fall to ensure peak immunity during flu season. Similarly, childhood vaccination schedules are designed to build immunity at critical developmental stages, such as the DTaP vaccine series (diphtheria, tetanus, and pertussis) starting at 2 months of age, with boosters at 4, 6, and 15–18 months. These schedules maximize the adaptive immune response while minimizing vulnerability during the interim period.
A key advantage of vaccine-induced adaptive immunity is its durability. Unlike passive immunity, which wanes within weeks to months, adaptive immunity can last for years or even a lifetime. For example, the yellow fever vaccine provides lifelong protection after a single dose, while the tetanus vaccine requires boosters every 10 years. However, this durability is not universal; some vaccines, like those for pertussis, may require more frequent boosters due to waning immunity or evolving pathogens. Practical tips for maintaining vaccine-induced immunity include keeping vaccination records up to date, consulting healthcare providers about booster needs, and staying informed about new vaccine recommendations, especially for travel or occupational risks.
In conclusion, vaccine-induced immunity is a prime example of the body’s adaptive immune system at work, offering active, long-term protection against infectious diseases. By understanding its mechanisms—from the initial immune response to the role of memory cells—individuals can make informed decisions about vaccination. Whether it’s following a childhood immunization schedule, getting an annual flu shot, or staying current with COVID-19 boosters, these actions collectively contribute to both personal and community health. The specificity and durability of adaptive immunity make vaccines one of the most effective tools in preventing disease, highlighting their indispensable role in global health strategies.
Exploring Ally Bank's Size, Reach, and Financial Impact
You may want to see also
Explore related products






![]()
Difference between adaptive and passive immunity
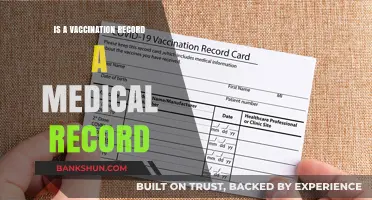
Vaccines harness the body’s immune system to prevent disease, but they don’t all work the same way. The key distinction lies in whether they trigger adaptive immunity or confer passive immunity. Adaptive immunity, the cornerstone of most vaccines, involves training the immune system to recognize and combat specific pathogens. Passive immunity, on the other hand, provides immediate but temporary protection by delivering pre-formed antibodies. Understanding this difference is crucial for appreciating how vaccines like the MMR (adaptive) or rabies immunoglobulin (passive) function.
Consider the mechanism of each. Adaptive immunity is a personalized defense system. When you receive a vaccine like the flu shot, it introduces a weakened or inactivated pathogen, prompting your immune cells to produce antibodies and memory cells. This process takes time—typically weeks—but the resulting immunity can last years or even a lifetime. For instance, the hepatitis B vaccine series, administered in three doses over 6 months, confers long-term protection by stimulating this adaptive response. In contrast, passive immunity bypasses this training phase. Products like the tetanus antitoxin deliver ready-made antibodies directly into the bloodstream, offering instant protection that wanes within weeks to months. This approach is ideal for urgent situations, such as preventing tetanus after a puncture wound, but it doesn’t leave behind immune memory.
The duration and application of these immunities further highlight their differences. Adaptive immunity is ideal for long-term prevention, as seen in childhood vaccines like DTaP (diphtheria, tetanus, pertussis), which require multiple doses to build robust, lasting immunity. Passive immunity, however, is a short-term solution. For example, the Rho(D) immune globulin given to Rh-negative pregnant women prevents maternal-fetal complications but only provides protection for about 12 weeks. Similarly, monoclonal antibody treatments for COVID-19 offer immediate relief but require repeated doses for sustained benefit.
Practical considerations also differentiate the two. Adaptive immunity vaccines often require booster shots to maintain effectiveness, as seen with the Tdap vaccine for teens and adults. Passive immunity, being transient, is reserved for specific scenarios: post-exposure prophylaxis (e.g., rabies immunoglobulin), immunocompromised individuals, or newborns who receive maternal antibodies via the placenta or breast milk. Dosage is critical here—for instance, rabies immunoglobulin is administered at 20 IU/kg body weight alongside the vaccine for maximum efficacy.
In summary, while both adaptive and passive immunity aim to protect against disease, their methods, durations, and applications diverge significantly. Vaccines like the COVID-19 mRNA shots exemplify adaptive immunity, fostering long-term defense through immune training. Passive immunity, as seen in antibody therapies, offers a rapid but fleeting shield. Knowing these distinctions empowers individuals to make informed decisions about their health and underscores the versatility of immunological tools in modern medicine.
Step-by-Step Guide: Paying Your Income Tax at the Bank Easily
You may want to see also
Explore related products






![]()
How vaccines trigger adaptive response
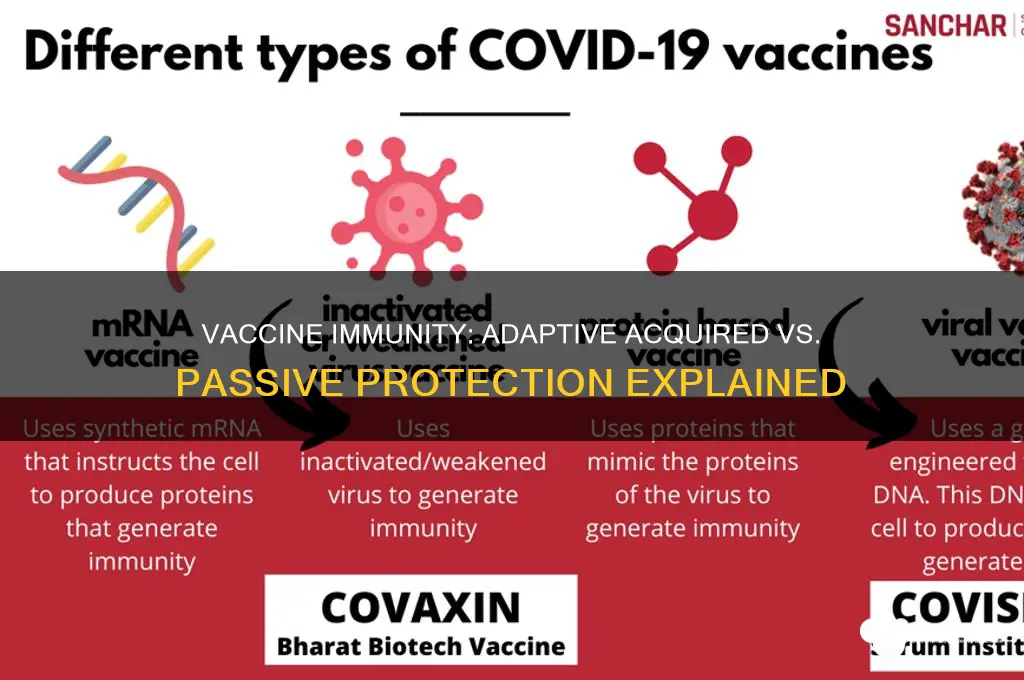
Vaccines are a cornerstone of modern medicine, but their true power lies in their ability to harness the body's own defense system. Unlike passive immunity, which involves the transfer of ready-made antibodies (such as through maternal antibodies or antibody injections), vaccines trigger an adaptive immune response, a process that equips the body to recognize and combat specific pathogens long-term. This distinction is critical: while passive immunity is temporary, adaptive immunity is enduring, providing a memory that allows for rapid response upon future exposure.
The adaptive immune response begins when a vaccine introduces a harmless form of a pathogen, such as a weakened virus, inactivated bacteria, or a fragment of the pathogen (like a protein or mRNA). For instance, the Pfizer-BioNTech COVID-19 vaccine delivers mRNA encoding the SARS-CoV-2 spike protein, prompting cells to produce this protein. Antigen-presenting cells (APCs) then engulf the protein, process it, and display fragments on their surface. These fragments are presented to T cells, which act as the orchestrators of the immune response. Helper T cells activate B cells, prompting them to differentiate into plasma cells that secrete antibodies specific to the pathogen. Simultaneously, cytotoxic T cells are primed to destroy infected cells directly.
A key feature of the adaptive response is immunological memory. After the initial infection is cleared, most activated B and T cells die off, but a small subset persists as memory cells. These memory cells circulate in the body for years or even decades, ready to mount a swift and robust response if the same pathogen is encountered again. This is why a second dose of many vaccines, such as the MMR (measles, mumps, rubella) vaccine, is often required—it boosts the number of memory cells and enhances the quality of antibodies produced. For example, the recommended interval between the first and second doses of the Moderna COVID-19 vaccine is 28 days, optimizing the memory response.
Practical considerations are essential for maximizing vaccine efficacy. Age, health status, and previous exposures can influence the strength of the adaptive response. Infants, for instance, receive multiple doses of vaccines like DTaP (diphtheria, tetanus, pertussis) over several months to build robust immunity, as their immune systems are still maturing. Adults, particularly the elderly, may require adjuvants—substances added to vaccines to enhance the immune response—due to age-related immune decline. For example, the shingles vaccine (Shingrix) contains an adjuvant to stimulate a stronger response in older adults.
In summary, vaccines trigger an adaptive immune response by mimicking infection without causing disease, activating both B and T cells, and establishing immunological memory. This process is tailored by factors like dosage, timing, and individual health, making vaccines a dynamic tool in preventive medicine. Understanding this mechanism underscores the importance of vaccination schedules and highlights why vaccines are a cornerstone of public health, offering long-term protection against infectious diseases.
Independent Bank Georgetown TX: Uncovering Its County Location and Services
You may want to see also
Explore related products






![]()
Passive immunity examples vs. vaccines
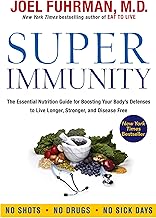
Vaccines and passive immunity both bolster the body's defenses, but they operate through distinct mechanisms with unique implications for protection. Passive immunity involves the direct transfer of ready-made antibodies, providing immediate but temporary defense. For instance, a newborn receives maternal antibodies via the placenta and breast milk, offering protection against pathogens like tetanus and measles during the first 6–12 months of life. Similarly, healthcare providers may administer tetanus immunoglobulin (250–500 units intramuscularly) to individuals with dirty wounds to prevent infection. In contrast, vaccines stimulate the immune system to produce its own antibodies, a process that takes weeks but confers long-term, often lifelong immunity. This fundamental difference shapes their use in different scenarios.
Consider the practical application of these approaches in high-risk situations. If someone is bitten by a rabid animal, they receive both a rabies vaccine and rabies immunoglobulin. The vaccine triggers adaptive immunity, training the body to recognize and combat the virus, while the immunoglobulin provides immediate passive protection during the critical window before the vaccine takes effect. This combination strategy highlights the complementary roles of passive immunity and vaccination. However, passive immunity’s short-lived nature limits its use to urgent, short-term needs, whereas vaccines are the cornerstone of preventive medicine, administered in doses tailored to age—e.g., the MMR vaccine given at 12–15 months and 4–6 years.
From a public health perspective, vaccines are far more cost-effective and scalable than passive immunity. Producing and distributing antibodies for widespread passive protection is impractical due to high costs and limited availability. Vaccines, on the other hand, can be mass-produced and administered through routine immunization programs, as seen with the global eradication efforts for smallpox and the ongoing campaigns against polio. Passive immunity remains a niche tool, reserved for specific cases like post-exposure prophylaxis or immunocompromised individuals who cannot mount a response to vaccines.
A critical distinction lies in the recipient’s immune involvement. Passive immunity bypasses the immune system’s learning process, offering no lasting memory of the pathogen. Vaccines, however, engage the adaptive immune system, creating memory cells that enable rapid response upon future exposure. This is why a single dose of varicella vaccine (93.7% effective) provides decades of protection against chickenpox, while passive immunity from varicella-zoster immunoglobulin lasts only 3–4 weeks. For parents, understanding this difference is key: vaccines are an investment in a child’s long-term health, whereas passive immunity is a temporary shield for immediate threats.
In summary, while passive immunity serves as a rapid, short-term solution, vaccines are the foundation of sustained immune resilience. Each has its place in medicine, but their contrasting mechanisms and durations dictate their appropriate use. For instance, travelers to regions with high yellow fever risk receive the vaccine at least 10 days before departure, ensuring adaptive immunity develops. In contrast, someone exposed to hepatitis A might receive immunoglobulin for immediate protection while awaiting the vaccine’s effects. Recognizing these distinctions empowers individuals to make informed decisions about their health and underscores the irreplaceable role of vaccines in global disease prevention.
Is the AAMC Section Bank Harder Than the Actual MCAT?
You may want to see also
Explore related products






![]()
Duration of vaccine-acquired immunity
Vaccine-acquired immunity, a cornerstone of adaptive immunity, hinges on the duration of protection it confers. Unlike passive immunity, which is short-lived and borrowed (e.g., maternal antibodies or convalescent plasma), vaccine-induced immunity is actively developed by the immune system and can persist for years or even decades. For instance, the measles vaccine provides lifelong immunity in most recipients, while the tetanus vaccine requires booster doses every 10 years to maintain protection. This variability underscores the importance of understanding the factors that influence the longevity of vaccine-acquired immunity.
The duration of vaccine-acquired immunity depends on several factors, including the type of vaccine, the pathogen it targets, and individual immune responses. Live-attenuated vaccines, such as the MMR (measles, mumps, rubella) vaccine, often confer long-lasting immunity because they mimic natural infection, stimulating robust memory B and T cell responses. In contrast, inactivated or subunit vaccines, like the seasonal flu shot, may require annual administration due to antigenic drift in the virus and a less durable immune memory. Age also plays a role; older adults may experience waning immunity due to immunosenescence, necessitating higher doses or adjuvanted formulations, as seen with the shingles vaccine (Shingrix), which is administered in two doses spaced 2–6 months apart for those over 50.
Practical considerations for maintaining vaccine-acquired immunity include adhering to recommended booster schedules and staying informed about updates to vaccination guidelines. For example, the Tdap vaccine (tetanus, diphtheria, pertussis) is recommended during pregnancy to protect newborns, while the HPV vaccine is most effective when administered in two doses to adolescents aged 9–14, compared to three doses for those vaccinated at 15–26 years. Travelers to regions with endemic diseases like yellow fever or typhoid should verify their vaccination status, as immunity may wane over time, requiring a booster dose.
Comparatively, the duration of vaccine-acquired immunity highlights the superiority of adaptive immunity over passive immunity in long-term protection. While passive immunity offers immediate but temporary defense, vaccines train the immune system to recognize and combat pathogens efficiently, often with memory responses that outlast the initial exposure. This distinction is critical in public health strategies, as evidenced by the eradication of smallpox and the near-elimination of polio through sustained vaccination campaigns. By prioritizing vaccines that induce durable immunity, societies can reduce disease burden and healthcare costs over time.
In conclusion, the duration of vaccine-acquired immunity is a dynamic and multifaceted aspect of adaptive immunity, shaped by vaccine type, pathogen characteristics, and individual factors. Maximizing this duration requires adherence to vaccination schedules, consideration of age-specific needs, and awareness of evolving guidelines. As a practical guide, individuals should consult healthcare providers to ensure their immunizations remain up-to-date, particularly when traveling or facing increased exposure risks. This proactive approach not only safeguards personal health but also contributes to community-wide immunity, reinforcing the enduring value of vaccines in modern medicine.
Reporting a Bank to the FDIC: A Step-by-Step Guide
You may want to see also
Frequently asked questions
A vaccine is considered adaptive acquired immunity because it stimulates the body's immune system to recognize and remember a specific pathogen, leading to long-term protection.
A vaccine triggers the body to produce its own antibodies and memory cells, which is adaptive acquired immunity, whereas passive immunity involves receiving pre-formed antibodies from an external source, providing immediate but temporary protection.
No, a vaccine does not provide passive immunity. It activates the immune system to develop its own response, which is characteristic of adaptive acquired immunity.
Vaccination is classified as adaptive acquired immunity because it involves the immune system learning to recognize and respond to a pathogen, resulting in long-lasting immunity, unlike passive immunity, which is short-lived and does not involve immune memory.
No, vaccines are designed to induce adaptive acquired immunity. Passive immunity is typically achieved through antibody injections or transplacental transfer, not through vaccination.