The question of whether the adult varicella vaccine is administered intramuscularly (IM) or subcutaneously (SC) is a common one, as the route of administration can impact the vaccine's efficacy and safety. According to the Centers for Disease Control and Prevention (CDC) and the vaccine manufacturer's guidelines, the varicella vaccine for adults, such as Varivax, is typically given subcutaneously, just below the skin's surface, usually in the upper arm. This route is preferred because it allows for proper absorption and immune response while minimizing potential side effects. Intramuscular injection is generally not recommended for the varicella vaccine, as it may lead to reduced effectiveness and increased local reactions. Healthcare providers must adhere to the specific administration instructions to ensure optimal protection against varicella-zoster virus, which causes chickenpox.
Explore related products






What You'll Learn
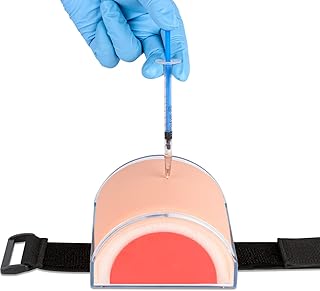
- Vaccine Administration Route: Varicella vaccine is typically administered subcutaneously, not intramuscularly
- Subcutaneous Technique: Inject into fatty tissue, usually in the upper arm or thigh
- IM vs. Subcut: Intramuscular route is incorrect for varicella vaccine; subcut is standard
- Dosage and Site: 0.65 mL for adults, given subcutaneously in deltoid or anterolateral thigh
- Adverse Reactions: Subcutaneous administration reduces risk of localized pain or swelling compared to IM
![]()
Vaccine Administration Route: Varicella vaccine is typically administered subcutaneously, not intramuscularly
The varicella vaccine, designed to protect against chickenpox, is administered subcutaneously, not intramuscularly. This distinction is crucial for healthcare providers to ensure optimal immune response and minimize adverse effects. The subcutaneous route involves injecting the vaccine into the fatty tissue just beneath the skin, typically in the upper arm or thigh. This method allows for slower absorption of the vaccine, which is essential for the varicella vaccine’s live attenuated virus to stimulate a robust immune response. In contrast, intramuscular injections, which deliver the vaccine directly into muscle tissue, are not recommended for this vaccine due to the risk of reduced efficacy and increased local reactions.
For adults receiving the varicella vaccine, the dosage is 0.65 mL per dose, administered as a two-dose series separated by 4 to 8 weeks. Proper technique is critical: the needle should be inserted at a 45-degree angle for individuals with thinner subcutaneous tissue or a 90-degree angle for those with more substantial tissue. Healthcare providers must avoid injecting the vaccine too deeply, as this could lead to intramuscular administration and compromise its effectiveness. Adhering to these guidelines ensures the vaccine reaches its intended target site, maximizing protection against varicella-zoster virus.
A comparative analysis highlights why the subcutaneous route is preferred for the varicella vaccine. Unlike vaccines such as influenza or COVID-19, which are often given intramuscularly, the varicella vaccine’s live attenuated nature requires a slower release into the bloodstream. Intramuscular administration could result in rapid absorption, potentially overwhelming the immune system and reducing the vaccine’s ability to replicate and trigger immunity. Additionally, subcutaneous injection is associated with fewer local reactions, such as pain or swelling, making it a more patient-friendly option for this specific vaccine.
Practical tips for healthcare providers include ensuring the vaccine is stored at the correct temperature (2°C to 8°C) to maintain its potency and using a small-gauge needle (e.g., 25-gauge) to minimize discomfort during administration. Patients should be informed that mild redness, soreness, or swelling at the injection site is normal and typically resolves within a few days. If administering the vaccine to adults who are unsure of their immunity status, providers should consider serologic testing or a history of chickenpox to avoid unnecessary vaccination. By following these specifics, healthcare professionals can ensure safe and effective varicella vaccine administration.
Avoid TCF Bank Overdraft Fees: Simple Strategies to Save Money
You may want to see also
Explore related products






![]()
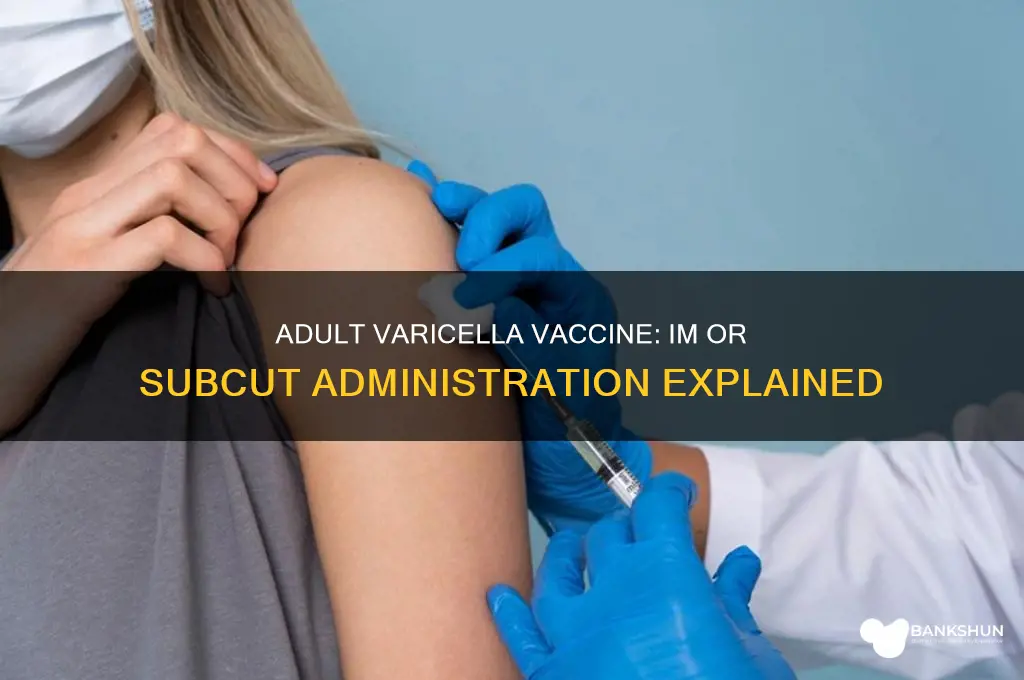
Subcutaneous Technique: Inject into fatty tissue, usually in the upper arm or thigh
The subcutaneous technique for administering the adult varicella vaccine involves injecting the vaccine into the fatty tissue just beneath the skin, typically in the upper arm or thigh. This method ensures the vaccine is delivered into the subcutaneous layer, where it can be effectively absorbed and processed by the immune system. Unlike intramuscular (IM) injections, which target muscle tissue, subcutaneous injections require precision to avoid deeper penetration. The upper arm (deltoid region) and the anterior thigh are preferred sites due to their accessible fatty tissue and lower risk of nerve or muscle damage.
For adults receiving the varicella vaccine, the subcutaneous route is often chosen because it minimizes discomfort and reduces the risk of injection site reactions compared to IM administration. The standard dosage for the varicella vaccine in adults is 0.5 mL, administered as two separate 0.5 mL doses at least 4 weeks apart. When injecting, the needle should be inserted at a 45-degree angle for individuals with less fatty tissue, or a 90-degree angle for those with sufficient subcutaneous fat. This ensures the vaccine remains within the fatty layer and does not enter the muscle or bloodstream directly.
Practical tips for healthcare providers include palpating the injection site to confirm the presence of fatty tissue and avoiding areas with scars, bruises, or inflammation. Patients should be instructed to relax the muscle in the injection area to minimize movement during administration. After injection, apply gentle pressure with a sterile swab if minor bleeding occurs, but avoid massaging the site, as this can disrupt vaccine absorption. Proper technique is critical to ensure the vaccine’s efficacy and patient comfort.
Comparatively, the subcutaneous technique offers advantages over IM injection for the varicella vaccine, particularly in terms of patient tolerance. Studies have shown that subcutaneous administration results in fewer local adverse effects, such as pain, redness, and swelling, making it a preferred method for adults. However, it requires more attention to detail, as improper placement can lead to reduced vaccine efficacy or increased side effects. Healthcare providers must be trained in identifying suitable injection sites and using the correct needle length (typically 5/8 inch for most adults) to ensure optimal outcomes.
In conclusion, the subcutaneous technique for adult varicella vaccination is a precise and patient-friendly approach that maximizes vaccine effectiveness while minimizing discomfort. By targeting fatty tissue in the upper arm or thigh, healthcare providers can ensure proper delivery of the 0.5 mL dose, adhering to the recommended two-dose schedule. Attention to technique, site selection, and patient preparation are key to successful subcutaneous administration, making it a valuable skill for vaccinators in adult immunization programs.
Does GoBank Charge for Cash Back? Fees Explained Simply
You may want to see also
Explore related products






![]()
IM vs. Subcut: Intramuscular route is incorrect for varicella vaccine; subcut is standard
The varicella vaccine, designed to protect against chickenpox, is administered via the subcutaneous (subcut) route, not intramuscularly (IM). This distinction is critical for healthcare providers and recipients alike, as the incorrect route can compromise the vaccine’s efficacy. For adults, the standard dose is 0.65 mL, delivered just below the skin’s surface, typically in the deltoid region of the upper arm for individuals aged 13 and older. Using the IM route, which injects the vaccine into muscle tissue, can lead to suboptimal immune response, as the varicella vaccine’s formulation is specifically tailored for subcutaneous absorption.
From an analytical perspective, the choice of administration route stems from the vaccine’s composition and intended immune response. Subcutaneous delivery allows the vaccine to interact with immune cells located in the dermis and subcutaneous tissue, triggering a robust antibody production. Intramuscular injection, while suitable for vaccines like influenza or COVID-19, bypasses this critical layer, potentially reducing the varicella vaccine’s effectiveness. Studies have shown that subcut administration consistently achieves higher seroconversion rates in adults, reinforcing its status as the gold standard.
For healthcare providers, adhering to the subcutaneous route is non-negotiable. Practical tips include using a 5/8-inch needle for adults and ensuring the needle bevel faces upward during injection to minimize tissue damage. The injection site should be cleaned with an alcohol swab, and the vaccine administered at a 45-degree angle, ensuring it reaches the subcutaneous space. Mistakenly using the IM route not only wastes the dose but also necessitates re-administration, delaying immunity and increasing costs.
Comparatively, the confusion between IM and subcut routes often arises from the variability in vaccine administration guidelines. For instance, the MMR vaccine is also given subcutaneously, but other vaccines, like hepatitis B, are IM. This highlights the importance of vaccine-specific protocols. Adults receiving the varicella vaccine should verify the route with their provider, especially if they have a history of vaccine reactions or immunocompromising conditions, as proper administration is key to safety and efficacy.
In conclusion, the subcutaneous route is the only correct method for administering the adult varicella vaccine. Deviating from this guideline undermines the vaccine’s purpose, emphasizing the need for precision in medical practice. By understanding the rationale behind the subcut route and following proper technique, healthcare providers can ensure optimal protection against varicella-zoster virus for their adult patients.
Barclays Bank: Uruguayan Locations and Services
You may want to see also
Explore related products






![]()
Dosage and Site: 0.65 mL for adults, given subcutaneously in deltoid or anterolateral thigh
The adult varicella vaccine is administered subcutaneously, not intramuscularly, a critical distinction for healthcare providers. This route ensures optimal immune response by delivering the vaccine into the layer of fat and tissue just beneath the skin, where antigen-presenting cells are abundant. The dosage is precisely 0.65 mL, a volume that balances efficacy and safety for adults. This specificity underscores the importance of adhering to guidelines to maximize protection against varicella-zoster virus (VZV), which causes chickenpox and can lead to shingles later in life.
Two injection sites are recommended: the deltoid muscle of the upper arm or the anterolateral thigh. The deltoid is preferred for adults due to its accessibility and lower risk of nerve injury compared to other sites. However, the anterolateral thigh is an alternative, particularly for individuals with insufficient deltoid mass or those who may experience discomfort from arm injections. Proper site selection ensures the vaccine is delivered into the subcutaneous tissue, avoiding deeper muscle layers, which could diminish its effectiveness.
Administering the vaccine requires attention to technique. The needle should be inserted at a 45-degree angle for individuals with thinner subcutaneous tissue or a 90-degree angle for those with more adipose tissue. This approach minimizes the risk of injecting the vaccine too deeply or causing unnecessary pain. Healthcare providers should also ensure the skin is clean and dry before injection to prevent infection and verify the absence of any skin conditions at the chosen site.
Practical tips can enhance the vaccination experience. For instance, warming the vaccine to room temperature before administration can reduce discomfort. Encouraging the recipient to relax the muscle at the injection site can also minimize pain. After injection, applying gentle pressure with a dry swab for a few seconds can prevent bleeding or bruising. These small steps contribute to a smoother process and may improve patient compliance with vaccination protocols.
In summary, the adult varicella vaccine’s subcutaneous administration of 0.65 mL in the deltoid or anterolateral thigh is a precise and deliberate approach to immunization. Adhering to dosage, site, and technique guidelines ensures the vaccine’s effectiveness while minimizing adverse effects. For healthcare providers, mastering these details is essential for protecting adults from varicella and its complications. For recipients, understanding the process can alleviate concerns and foster confidence in the vaccination.
Is Banks Ale Sold in the USA? Availability and Where to Find It
You may want to see also
Explore related products






![]()
Adverse Reactions: Subcutaneous administration reduces risk of localized pain or swelling compared to IM
The route of administration for the adult varicella vaccine significantly impacts the likelihood of adverse reactions, particularly localized pain and swelling. Subcutaneous (SC) injection, which delivers the vaccine into the fatty tissue just beneath the skin, is associated with a lower risk of these side effects compared to intramuscular (IM) injection, where the vaccine is administered directly into the muscle. This difference is primarily due to the anatomical characteristics of the injection sites and the body’s response to the vaccine in these areas. For instance, the subcutaneous layer has fewer nerve endings and blood vessels than muscle tissue, reducing the potential for discomfort and inflammation.
From a practical standpoint, healthcare providers should consider the patient’s age, medical history, and pain tolerance when choosing the administration route. For adults receiving the varicella vaccine, the SC route is often preferred for its safety profile, especially in individuals with a history of injection-site reactions or those who are particularly sensitive to pain. The standard dosage for the varicella vaccine in adults is 0.65 mL for the first dose and the same amount for the second dose, administered 4 to 8 weeks apart. When given subcutaneously, the needle should be inserted at a 45-degree angle, ensuring the vaccine is delivered into the fatty tissue rather than the muscle.
Comparatively, IM injections, while effective, carry a higher risk of localized adverse reactions due to the muscle’s rich blood supply and nerve density. Patients may experience more pronounced pain, redness, or swelling at the injection site, which can last for several days. This is particularly relevant for adults, who may have a lower pain threshold compared to children or may be more likely to notice and report discomfort. For example, a study comparing SC and IM administration of the varicella vaccine found that 20% of IM recipients reported moderate to severe pain, compared to only 5% of SC recipients.
To minimize the risk of adverse reactions, healthcare providers can employ specific techniques when administering the vaccine subcutaneously. Using a small-gauge needle (e.g., 25-gauge) and ensuring proper patient positioning can further reduce discomfort. Patients should be advised to apply a cold compress to the injection site if mild swelling or pain occurs, though such reactions are less common with SC administration. Additionally, providers should educate patients about the expected side effects and reassure them that localized reactions are typically mild and self-limiting.
In conclusion, subcutaneous administration of the adult varicella vaccine offers a safer alternative to intramuscular injection by significantly reducing the risk of localized pain and swelling. This route is particularly advantageous for adults, who may be more susceptible to injection-site reactions. By understanding the anatomical and physiological differences between SC and IM injections, healthcare providers can make informed decisions that enhance patient comfort and vaccine acceptance. Practical tips, such as proper needle selection and patient education, further contribute to a smoother vaccination experience.
Master MYOB Bank Reconciliation: A Step-by-Step Guide to Accurate Feeds
You may want to see also
Frequently asked questions
The adult varicella vaccine is administered subcutaneously (SubQ), not intramuscularly (IM).
The varicella vaccine is given subcutaneously because the virus in the vaccine is more effectively absorbed and processed by the immune system when delivered into the subcutaneous tissue.
No, the adult varicella vaccine should not be given intramuscularly. It is specifically formulated for subcutaneous administration, and deviating from this route may reduce its effectiveness.
Administering the varicella vaccine intramuscularly can lead to reduced immune response, potentially compromising the vaccine's effectiveness in preventing varicella (chickenpox). Always follow the recommended subcutaneous route.