The H1N1 vaccine, developed to combat the 2009 swine flu pandemic, often required a two-shot process for certain populations, particularly children and individuals with weakened immune systems. This approach was necessary to ensure adequate immunity, as a single dose might not provide sufficient protection against the virus. The two doses were typically administered several weeks apart, allowing the immune system to build a robust response. However, for healthy adults and older children, a single dose was often deemed sufficient. The specific recommendation for one or two doses depended on factors such as age, health status, and prior exposure to similar influenza strains. Public health guidelines during the pandemic emphasized the importance of following the recommended dosing schedule to maximize the vaccine's effectiveness in preventing H1N1 infection.
| Characteristics | Values |
|---|---|
| Vaccine Type | Inactivated influenza vaccine (IIV) or live attenuated influenza vaccine (LAIV) |
| Dosing Schedule for Children (6 months to 8 years) | Two doses, 4 weeks apart, if it’s the first time receiving flu vaccine |
| Dosing Schedule for Adults and Children (9 years and older) | One dose |
| Vaccine Availability | Seasonal flu vaccines often include H1N1 protection |
| Immunity Development | Full immunity typically develops 2 weeks after the final dose |
| Booster Requirement | Annual flu vaccination recommended due to evolving strains |
| Special Populations | Pregnant women and immunocompromised individuals may require specific guidance |
| Side Effects | Mild side effects (soreness, fever, headache) are common |
| Effectiveness | Varies annually based on strain match; generally 40-60% effective |
| Latest Recommendation (2023) | Follow CDC or WHO guidelines for annual flu vaccination |
Explore related products



$9.99 $10.69


What You'll Learn
- Initial Dosing Schedule: Most H1N1 vaccines required two doses for full immunity in 2009
- Age-Based Requirements: Children under 10 often needed two shots; adults typically one
- Immune Response: Two doses ensured stronger antibody production in certain populations
- Vaccine Type: Adjuvanted vaccines sometimes allowed single-dose protection
- Current Guidelines: H1N1 is now included in annual flu shots, one dose
![]()
Initial Dosing Schedule: Most H1N1 vaccines required two doses for full immunity in 2009
During the 2009 H1N1 pandemic, health authorities faced the challenge of rapidly immunizing populations against a novel influenza strain. One critical decision was the dosing schedule for the newly developed vaccines. Unlike the annual flu shot, which typically requires a single dose for most individuals, the H1N1 vaccine was initially recommended as a two-dose regimen for full immunity. This decision was based on early clinical trials indicating that a single dose might not provide sufficient protection, particularly in younger children and those with no prior exposure to similar influenza strains.
The two-dose schedule was straightforward: individuals received an initial dose, followed by a second dose 21 to 28 days later. This interval allowed the immune system to mount a robust response after the first dose, with the second dose acting as a booster to ensure long-lasting immunity. For children aged 6 months to 9 years, the recommended dosage was typically 0.25 mL per dose for the inactivated vaccine, while adults and older children received 0.5 mL per dose. Pregnant women, healthcare workers, and individuals with underlying health conditions were prioritized due to their higher risk of severe complications.
Practical implementation of this schedule posed logistical challenges. Public health systems had to coordinate mass vaccination campaigns, ensuring that recipients returned for their second dose within the prescribed timeframe. Reminder systems, such as phone calls, emails, and follow-up appointments, were employed to minimize missed doses. Additionally, vaccine supply constraints required careful allocation to ensure enough doses were available for both initial and booster shots. Despite these hurdles, the two-dose regimen was deemed necessary to maximize protection during a rapidly spreading pandemic.
Comparatively, the two-dose approach for H1N1 contrasted with the single-dose strategy for seasonal flu vaccines, highlighting the unique characteristics of the novel virus. Subsequent studies showed that individuals with prior exposure to similar H1N1 strains or those over 10 years old often developed adequate immunity after a single dose. However, the initial two-dose recommendation was a precautionary measure to address the uncertainty surrounding the virus’s behavior and the population’s immune response. This underscores the importance of tailoring vaccination strategies to the specific threat at hand.
In retrospect, the two-dose H1N1 vaccine schedule of 2009 exemplifies the balance between scientific caution and public health urgency. While it presented logistical complexities, it prioritized maximizing immunity during a critical period. For those planning vaccinations during a pandemic, this history serves as a reminder to follow dosing guidelines closely, stay informed about updates, and leverage reminders to ensure completion of the full regimen. Understanding such specifics can empower individuals to make informed decisions and contribute to collective immunity.
Understanding Bank Trust Services: Safeguarding Your Assets and Financial Future
You may want to see also
Explore related products






![]()
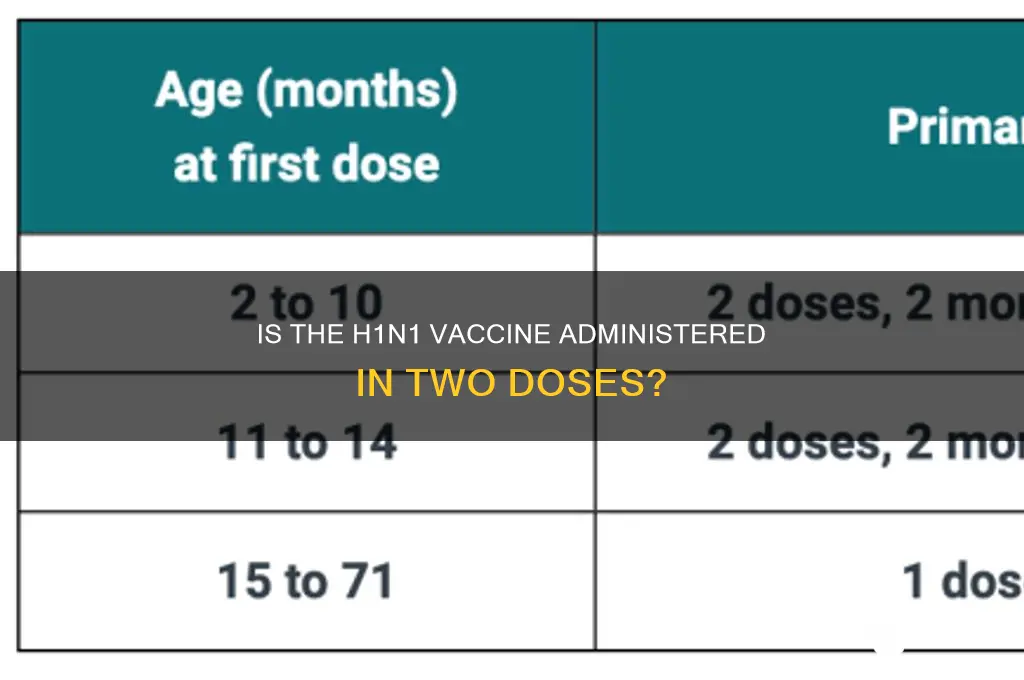
Age-Based Requirements: Children under 10 often needed two shots; adults typically one
Children under 10 often required a two-dose regimen of the H1N1 vaccine, a critical detail for parents navigating immunization schedules. This age-specific requirement stemmed from the immature immune systems of young children, which typically mount a weaker response to vaccines. The first dose primed their immune system, while the second, administered 21 to 28 days later, significantly boosted antibody production, offering robust protection against the H1N1 virus. This two-shot approach ensured that even the youngest recipients achieved adequate immunity, a vital safeguard during the 2009 pandemic.
In contrast, adults and older children generally needed only a single dose of the H1N1 vaccine. This disparity highlights the immune system's maturation process. By age 10, most individuals have developed a more robust immune response, capable of generating sufficient antibodies after just one vaccination. This single-dose protocol streamlined vaccination efforts for older populations, allowing for broader and more efficient distribution during the pandemic.
The age-based dosing strategy for the H1N1 vaccine underscores the importance of tailoring immunization protocols to specific demographic needs. For parents, understanding this requirement was crucial for ensuring their children received complete protection. Healthcare providers played a pivotal role in educating families about the two-dose regimen for younger children, emphasizing the importance of adhering to the recommended schedule. This targeted approach maximized the vaccine's effectiveness across different age groups, contributing to the overall success of the H1N1 vaccination campaign.
Practical considerations for parents included scheduling both doses well in advance, especially during periods of high vaccine demand. Keeping a record of vaccination dates and ensuring children received the same vaccine brand for both doses (when applicable) were also essential. For adults, the single-dose requirement simplified the process, allowing for quicker immunization and greater flexibility in scheduling. This age-specific approach not only optimized individual protection but also facilitated a more efficient public health response to the H1N1 pandemic.
Bank Teller Interview Success: Key Skills and Qualities Employers Seek
You may want to see also
Explore related products






![]()
Immune Response: Two doses ensured stronger antibody production in certain populations
The 2009 H1N1 pandemic highlighted the importance of vaccine dosing strategies, particularly for vulnerable populations. Studies revealed that a single dose of the H1N1 vaccine often failed to elicit a robust immune response in children under 10 years old. This age group, characterized by immunological immaturity, required a two-dose regimen to achieve adequate antibody titers. The recommended interval between doses was 21 days, allowing the immune system sufficient time to recognize the antigen and mount a stronger, more durable response.
This finding underscores the need for tailored vaccination approaches based on age-specific immune profiles.
Consider the mechanism behind this phenomenon. The first dose primes the immune system, introducing the H1N1 antigen and stimulating the production of memory B cells. These cells, upon encountering the same antigen in the second dose, rapidly proliferate and differentiate into antibody-secreting plasma cells. This amplified response results in significantly higher antibody titers compared to a single dose. Think of it as a two-step training program for the immune system, where the initial exposure lays the groundwork and the second reinforces the learned response.
This principle of immune memory is fundamental to the success of many vaccination protocols.
The benefits of a two-dose regimen extend beyond children. Pregnant women, another vulnerable population, also demonstrated enhanced antibody production after receiving two doses of the H1N1 vaccine. This is crucial as maternal antibodies are transferred to the fetus, providing passive immunity to the newborn during the first few months of life. A single dose, while offering some protection, may not generate sufficient antibodies to ensure adequate protection for both mother and child. Therefore, the two-dose strategy becomes a vital tool in safeguarding these high-risk groups.
It's important to note that the specific dosage and interval recommendations may vary depending on the vaccine formulation and individual health status. Consulting with a healthcare professional is essential for personalized advice.
In conclusion, the H1N1 vaccine's two-dose approach for certain populations exemplifies the nuanced understanding of immune response required for effective vaccination strategies. By tailoring dosing regimens based on age, health status, and other factors, we can optimize antibody production and maximize protection against infectious diseases. This highlights the ongoing research and refinement in vaccine development, ensuring that immunization programs are both safe and highly effective.
Securely Depositing Coins: A Step-by-Step Guide to Banking Your Change
You may want to see also
Explore related products






![]()
Vaccine Type: Adjuvanted vaccines sometimes allowed single-dose protection
Adjuvanted vaccines, which contain additives to enhance the immune response, played a pivotal role in the 2009 H1N1 pandemic by offering single-dose protection in certain populations. Unlike traditional vaccines, adjuvants such as AS03 (found in Pandemrix) or MF59 (used in Focetria) allowed for a robust immune response even with a lower antigen dose. This was particularly critical during the pandemic when rapid vaccination of large populations was necessary, and antigen supply was limited. For instance, studies showed that a single 3.75-microgram dose of adjuvanted H1N1 vaccine induced sufficient immunity in adults, compared to the standard 15-microgram dose of non-adjuvanted vaccines, which often required two doses for full protection.
The effectiveness of adjuvanted vaccines in providing single-dose protection was not universal, however. Age emerged as a key factor in determining the immune response. Adults and older children often achieved protective antibody levels after one dose, while younger children, particularly those under 10, frequently required a second dose to ensure adequate immunity. For example, the European Medicines Agency recommended a two-dose regimen for children aged 6 months to 9 years, spaced 3 weeks apart, to account for their less mature immune systems. This highlights the importance of tailoring vaccination strategies based on age-specific immune responses.
From a practical standpoint, adjuvanted vaccines offered logistical advantages during the H1N1 pandemic. By reducing the number of required doses, healthcare systems could vaccinate more individuals faster, a critical factor in controlling the spread of the virus. However, the use of adjuvants also raised concerns about safety, particularly regarding rare side effects such as narcolepsy, which was later associated with Pandemrix in certain populations. This underscores the need for careful monitoring and risk-benefit analysis when deploying adjuvanted vaccines, especially in emergency situations.
Instructively, for those considering adjuvanted vaccines, it’s essential to follow age-specific guidelines and consult healthcare providers for personalized advice. For adults, a single dose of an adjuvanted H1N1 vaccine was generally sufficient, while parents of young children should be prepared for a two-dose schedule. Additionally, individuals with compromised immune systems or chronic conditions should discuss their vaccination plan with a healthcare professional, as adjuvanted vaccines may not provide the same level of protection in these groups. Understanding these nuances ensures optimal protection while minimizing potential risks.
Comparatively, adjuvanted vaccines represent a significant advancement in vaccine technology, particularly in pandemic scenarios where speed and efficiency are paramount. Their ability to provide single-dose protection in many cases contrasts sharply with non-adjuvanted vaccines, which often rely on multi-dose regimens. However, this innovation comes with trade-offs, including the need for rigorous safety monitoring and age-specific dosing strategies. As vaccine technology continues to evolve, adjuvanted vaccines will likely remain a valuable tool in the global effort to combat infectious diseases, offering a balance between efficacy, accessibility, and safety.
Square Fees: Tax-Deductible or Bank Charges?
You may want to see also
Explore related products






![]()
Current Guidelines: H1N1 is now included in annual flu shots, one dose
The H1N1 virus, once a standalone threat, has been seamlessly integrated into the annual influenza vaccine, simplifying protection against this strain. Current guidelines from health authorities like the CDC and WHO confirm that the H1N1 component is included in the seasonal flu shot, eliminating the need for a separate vaccine. This consolidation reflects the virus’s evolution from pandemic to endemic status, now treated as one of several influenza strains circulating annually.
For most individuals, a single dose of the seasonal flu vaccine is sufficient to confer immunity against H1N1 and other targeted strains. This one-dose regimen applies to adults and children aged 9 and older, provided they have no history of severe allergic reactions to flu vaccines. The standard dosage for adults is 0.5 mL, administered via intramuscular injection, typically in the upper arm. For children aged 6 months to 8 years, dosage may vary depending on prior vaccination history, with some requiring two doses spaced four weeks apart if it’s their first flu vaccine.
The shift to a single-dose approach for H1N1 is rooted in scientific evidence demonstrating the vaccine’s efficacy when combined with other influenza strains. Studies show that the quadrivalent flu vaccine, which includes H1N1, H3N2, and two influenza B viruses, provides robust protection across age groups. This streamlined process not only reduces the logistical burden on healthcare systems but also improves compliance, as individuals no longer need to track separate H1N1 vaccinations.
Practical tips for maximizing the vaccine’s effectiveness include scheduling the shot early in the flu season (ideally by October) and ensuring proper storage and handling of the vaccine by healthcare providers. Pregnant women, older adults, and individuals with chronic conditions should prioritize vaccination, as they are at higher risk for severe complications from H1N1 and other flu strains. Side effects, such as soreness at the injection site or mild fatigue, are generally mild and short-lived, signaling a normal immune response rather than cause for concern.
Incorporating H1N1 into the annual flu shot represents a public health triumph, transforming a once-urgent pandemic response into routine preventive care. By adhering to current guidelines and receiving a single dose of the seasonal flu vaccine, individuals can protect themselves and contribute to community-wide immunity, minimizing the impact of H1N1 and other influenza viruses.
Understanding the Role of a Commercial Banking Associate: Key Responsibilities
You may want to see also
Frequently asked questions
No, the H1N1 vaccine is typically a single-dose process for most individuals. However, children under 10 years old may require two doses, spaced about 4 weeks apart, to achieve full immunity.
Some individuals, particularly young children with no prior exposure to H1N1, may not develop sufficient immunity with a single dose. The second dose boosts their immune response to ensure protection.
Your healthcare provider will determine if you need two doses based on factors like age, health status, and prior exposure to H1N1. Follow their guidance for the appropriate vaccination schedule.
Adults typically only need one dose of the H1N1 vaccine. A second dose is generally not recommended unless advised by a healthcare professional due to specific health conditions.
If you or your child misses the second dose, consult your healthcare provider. They may recommend rescheduling the second dose to ensure full protection, but the timing may vary based on individual circumstances.