The question of whether a health record bank is the same as a Personal Health Record (PHR) often arises due to their overlapping roles in managing health information. While both systems aim to centralize and store medical data, they differ significantly in their structure, ownership, and functionality. A health record bank typically operates as a third-party repository that securely stores and manages health records on behalf of individuals or organizations, often with a focus on interoperability and data sharing across healthcare providers. In contrast, a PHR is a digital tool that allows individuals to maintain and control their own health information, enabling them to input, update, and share their records as needed. Understanding these distinctions is crucial for individuals and healthcare professionals seeking to leverage these systems effectively for better health management and care coordination.
Explore related products






What You'll Learn
![]()
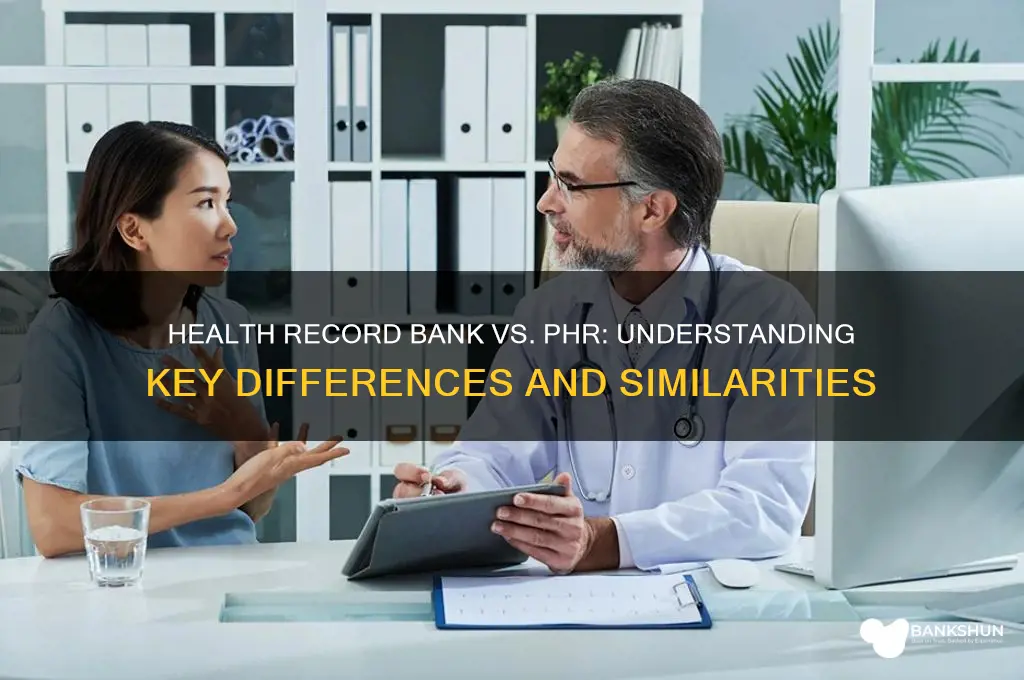
Definition of Health Record Bank vs. PHR
Health record banks and personal health records (PHRs) are often conflated, but they serve distinct purposes in managing health information. A health record bank functions as a centralized repository where medical data from various sources—hospitals, clinics, labs, and pharmacies—is stored and secured. Think of it as a digital vault, accessible primarily by authorized healthcare providers, ensuring data integrity and interoperability. In contrast, a PHR is a patient-centric tool, typically managed by individuals, that allows them to input, track, and share their health information. While both systems handle health data, their ownership, control, and primary users differ fundamentally.
To illustrate, consider a patient diagnosed with diabetes. A health record bank would automatically aggregate their lab results, prescriptions, and specialist notes from multiple providers, creating a comprehensive, up-to-date profile. Meanwhile, a PHR would enable the patient to log daily blood sugar levels, diet, and exercise, offering a personalized view of their health journey. The bank focuses on clinical data consolidation, whereas the PHR emphasizes patient engagement and self-management. This distinction highlights their complementary roles rather than interchangeable functions.
From a practical standpoint, understanding these differences is crucial for informed decision-making. For instance, a health record bank is ideal for ensuring seamless care coordination during emergencies, as it provides immediate access to critical medical history. However, a PHR empowers patients to take proactive steps, such as setting medication reminders or tracking symptoms over time. Healthcare providers should educate patients on leveraging both systems: using the bank for accurate, provider-verified data and the PHR for day-to-today health monitoring. This dual approach maximizes the benefits of each tool.
A cautionary note: while health record banks prioritize security, they are not immune to breaches or accessibility issues. Patients relying solely on such systems may face delays in accessing their data during technical outages. Conversely, PHRs, often hosted on consumer platforms, may lack robust privacy protections. For example, a PHR app might inadvertently share sensitive information if not configured correctly. Users must weigh these risks and adopt best practices, such as enabling two-factor authentication and regularly updating passwords, to safeguard their health data across both platforms.
In conclusion, the health record bank and PHR are not synonymous but rather complementary components of modern healthcare infrastructure. The bank excels in data aggregation and provider accessibility, while the PHR fosters patient autonomy and engagement. By understanding their unique strengths and limitations, individuals and healthcare professionals can harness these tools effectively, ultimately improving health outcomes and care delivery.
Step-by-Step Guide to Registering MCB Mobile Banking App Easily
You may want to see also
Explore related products






![]()
Ownership and Control Differences
Health record banks and personal health records (PHRs) diverge sharply in who owns and controls the data. In a health record bank, the institution—often a hospital, government agency, or third-party provider—retains legal ownership of the records. Patients access their data but cannot unilaterally alter or delete it. For instance, a hospital-managed health record bank might allow patients to view lab results but restricts modifications to authorized healthcare providers. Conversely, a PHR places ownership squarely in the patient’s hands. Using platforms like Apple Health or MyChart, individuals input, edit, and share their health data at will, without institutional oversight. This fundamental difference dictates not only accessibility but also the permanence and portability of the records.
Consider a scenario where a patient moves across state lines. In a health record bank model, transferring records requires institutional approval and may involve delays or fees. The bank’s proprietary systems could also limit compatibility with new providers. With a PHR, the patient simply downloads their data and uploads it to a new platform, retaining full control throughout the process. This autonomy is particularly valuable for chronic disease management, where continuous, uninterrupted access to historical data is critical. However, it also raises questions about data accuracy, as patients might inadvertently input incorrect information without professional verification.
From a legal standpoint, ownership differences have tangible implications. Health record banks are bound by regulations like HIPAA in the U.S., which governs data sharing and security. Patients have limited recourse if the bank mishandles their data, as they do not own it. PHRs, while often subject to the same regulations, empower patients to take legal action for unauthorized access or breaches, since they hold ownership rights. For example, if a PHR platform is hacked, patients can sue for damages, whereas health record bank users must rely on the institution’s response. This shift in liability underscores the trade-off between convenience and responsibility.
Practically, these differences influence how patients engage with their health data. Health record banks foster a passive relationship, where patients rely on providers to update and interpret records. PHRs encourage active participation, enabling users to track trends, set medication reminders (e.g., 200 mg of metformin twice daily for diabetes), or log symptoms over time. For instance, a PHR user might notice a correlation between dietary changes and blood sugar levels, prompting a discussion with their doctor. While this proactive approach can improve outcomes, it demands digital literacy and time—barriers for older adults or those without tech access.
Ultimately, the choice between a health record bank and a PHR hinges on individual priorities. Institutions prioritizing data integrity and standardized care may favor health record banks, ensuring records remain accurate and secure. Patients seeking autonomy and flexibility will lean toward PHRs, despite the added responsibility. For example, a 65-year-old with hypertension might prefer a health record bank’s streamlined interface, while a tech-savvy 30-year-old managing allergies could benefit from a PHR’s customization options. Understanding these ownership and control differences empowers individuals to make informed decisions about their health data management.
Reprint Challan in ICICI Bank: A Step-by-Step Guide
You may want to see also
Explore related products

![PHR Study Cards 2025-2026: PHR Exam Prep and Practice Test Questions for the Professional in Human Resources Exam [2nd Edition]](https://m.media-amazon.com/images/I/51rNR4-zF0L._AC_UY218_.jpg)



![PHR Study Guide 2022-2023: PHR Exam Prep Book and Practice Test Questions: [7th Edition]](https://m.media-amazon.com/images/I/71Xm33uIg+L._AC_UY218_.jpg)
![]()
Data Accessibility and Sharing
Health record banks and personal health records (PHRs) both aim to centralize health data, but their approaches to data accessibility and sharing differ significantly. Health record banks often operate as third-party repositories, aggregating data from multiple sources like hospitals, labs, and pharmacies. In contrast, PHRs are typically patient-controlled, allowing individuals to input, store, and manage their own health information. This fundamental difference shapes how data is accessed and shared, with health record banks prioritizing interoperability and broad data exchange, while PHRs emphasize patient autonomy and selective sharing.
To illustrate, consider a patient with diabetes who uses a health record bank. Their bank might automatically pull lab results, medication lists, and appointment histories from various providers, creating a comprehensive profile accessible to authorized healthcare professionals. This seamless data flow can improve care coordination, as specialists can quickly review the patient’s history without relying on fragmented records. However, this convenience comes with trade-offs: patients may have less control over who accesses their data, and privacy concerns arise if the bank lacks robust security measures. For instance, a health record bank might share data with researchers, requiring anonymization to protect patient identities, but even this step isn’t foolproof.
In contrast, a PHR empowers the same diabetic patient to decide what information to include and who can view it. For example, they might upload glucose readings from a wearable device but exclude mental health notes from a therapist. When visiting a new endocrinologist, they can grant temporary access to specific records, ensuring the doctor has relevant data without exposing their entire health history. This granular control aligns with principles of patient-centered care but requires active participation. A practical tip for PHR users: regularly update your records and review sharing permissions to avoid outdated information or unintended access.
The choice between a health record bank and a PHR often hinges on the user’s priorities. For those seeking effortless data consolidation and provider collaboration, a health record bank may be ideal. However, patients who value privacy and control might prefer a PHR, despite the added responsibility of manual updates. A comparative analysis reveals that neither system is universally superior; rather, their effectiveness depends on the user’s needs and the context of care. For instance, elderly patients or those with complex conditions may benefit from the automated features of a health record bank, while tech-savvy individuals might thrive with a PHR’s customization options.
Ultimately, the future of data accessibility and sharing in healthcare lies in bridging the gap between these models. Emerging technologies like blockchain could enable secure, patient-controlled data exchange, combining the interoperability of health record banks with the autonomy of PHRs. Until then, patients and providers must weigh the pros and cons of each system, ensuring that data accessibility enhances care without compromising privacy. A key takeaway: whether using a health record bank or a PHR, understanding how your data is shared and protected is essential for informed decision-making in healthcare.
Cord Blood Banking: Optimal Storage Duration for Future Health Benefits
You may want to see also
Explore related products
![PHR Study Guide 2021-2022 - PHR Test Prep Secrets for the Professional in Human Resources Certification, Practice Exam Questions, Detailed Answer Explanations: [3rd Edition Book]](https://m.media-amazon.com/images/I/71kLd7C1onL._AC_UY218_.jpg)

![PHR Study Guide 2025-2026 - 3 Full-Length Practice Tests, Secrets Prep Book for the HRCI PHR Certification Exam: [7th Edition]](https://m.media-amazon.com/images/I/71HWE3nolDL._AC_UL320_.jpg)


![]()
Security and Privacy Measures
Health record banks and personal health records (PHRs) both handle sensitive medical data, but their security and privacy measures differ significantly. Health record banks, often managed by third-party organizations, act as centralized repositories for health information from multiple sources. In contrast, PHRs are typically controlled by individuals, who input and manage their own data. This fundamental difference dictates the security protocols each employs. For instance, health record banks must implement robust access controls to prevent unauthorized data sharing across institutions, while PHRs focus on user authentication and encryption to safeguard personal entries.
To ensure data integrity, health record banks frequently adopt blockchain technology, which creates an immutable ledger of all transactions. This makes it nearly impossible for malicious actors to alter records without detection. PHRs, on the other hand, often rely on end-to-end encryption, ensuring that only the user and authorized parties can access the information. For example, a PHR might use AES-256 encryption, a standard that even governments trust for protecting classified information. Users should also enable two-factor authentication (2FA) to add an extra layer of security, especially if their PHR is cloud-based.
Compliance with regulations like HIPAA in the U.S. or GDPR in Europe is non-negotiable for health record banks, which face stringent audits and penalties for breaches. PHRs, however, may not always fall under these regulations, depending on their provider. Users must therefore scrutinize the privacy policies of their PHR platforms, ensuring they meet personal standards for data protection. For instance, a PHR that stores data on servers in countries with lax privacy laws could expose users to greater risk, even if the platform itself claims to be secure.
Practical steps for individuals using PHRs include regularly updating passwords, avoiding public Wi-Fi for accessing sensitive data, and backing up records offline. Health record banks, meanwhile, should conduct penetration testing quarterly to identify vulnerabilities and invest in employee training to mitigate human error. A real-world example is the 2015 breach of a major health record bank, which exposed millions of records due to a phishing attack—a scenario that could have been prevented with better staff awareness.
Ultimately, while both systems aim to protect health data, their security and privacy measures reflect their distinct purposes. Health record banks prioritize interoperability and institutional safeguards, whereas PHRs emphasize user control and personal encryption. Understanding these differences empowers individuals and organizations to make informed decisions about where and how their health data is stored, ensuring it remains confidential, secure, and accessible only to those who need it.
Bank Forms Retention: How Long Should You Keep Them?
You may want to see also
Explore related products
![PHR Study Guide: 6 Practice Tests and PHR Exam Prep: [8th Edition]](https://m.media-amazon.com/images/I/71VjrKbB49L._AC_UL320_.jpg)

![PHR Study Cards 2025-2026: PHR Exam Prep and Practice Test Questions for the Professional in Human Resources Certification [Full Color Cards]](https://m.media-amazon.com/images/I/61YI0jtdPBL._AC_UL320_.jpg)


![]()
Purpose and Usage Scenarios
Health record banks and personal health records (PHRs) serve distinct purposes, though they often overlap in functionality. A health record bank typically acts as a centralized repository for medical data, managed by a third-party organization or institution. Its primary purpose is to store and secure health information, ensuring accessibility for authorized users, such as healthcare providers or researchers. In contrast, a PHR is patient-centric, designed for individuals to manage their own health data, track conditions, and share information with providers. Understanding these differences is crucial for determining which tool aligns with specific usage scenarios.
Consider a scenario where a patient with a chronic condition, like diabetes, needs to monitor glucose levels, medication adherence, and doctor’s notes. A PHR would be ideal here, as it allows the patient to input daily blood sugar readings (e.g., fasting glucose levels of 70–130 mg/dL), log insulin dosages (e.g., 10 units of Lantus daily), and upload lab results. This empowers the individual to take an active role in their care and share real-time data with their endocrinologist during appointments. A health record bank, however, might be less practical for this purpose, as it’s not designed for patient-driven updates but rather for storing comprehensive records from multiple sources.
In another scenario, a researcher studying population health trends might rely on a health record bank to access de-identified data from thousands of patients. This centralized repository enables large-scale analysis, such as identifying risk factors for cardiovascular disease in individuals over 50. Here, the health record bank’s ability to aggregate and secure data from diverse sources (hospitals, clinics, labs) is invaluable. A PHR, on the other hand, would be insufficient for this purpose, as it lacks the scale and standardization required for research.
For families managing care for an elderly relative, a PHR can serve as a shared tool. Adult children could input medication schedules (e.g., 81 mg aspirin daily), track doctor’s appointments, and monitor vital signs like blood pressure (target: <120/80 mmHg). This ensures continuity of care and reduces the risk of errors. A health record bank, while useful for storing historical records, wouldn’t offer the same level of flexibility or family accessibility in this context.
Ultimately, the choice between a health record bank and a PHR depends on the user’s needs. Patients seeking control over their day-to-day health management will benefit from a PHR, while institutions or researchers requiring large-scale data aggregation should opt for a health record bank. Both tools complement each other in the healthcare ecosystem, but their usage scenarios are distinctly tailored to different stakeholders.
Mastering Cross-Selling Strategies to Boost Bank Revenue and Customer Loyalty
You may want to see also
Frequently asked questions
No, a health record bank is a centralized repository that stores and manages health records from multiple sources, often controlled by a third-party organization. A PHR, on the other hand, is a digital health record managed and controlled by the individual patient, allowing them to input, update, and share their health information.
Yes, they can complement each other. A health record bank may provide comprehensive data from various healthcare providers, while a PHR allows the individual to add personal health details, track progress, and maintain control over their health information.
In a health record bank, the data is typically owned or managed by the organization operating the bank, though patients may have access rights. In a PHR, the individual patient owns and controls their data, deciding how and with whom it is shared.


![PHR Practice Question Study Cards 2025-2026: PHR Test Questions Exam Prep for the HRCI PHR Certification [Full Color Cards]](https://m.media-amazon.com/images/I/51WxUc+jZGL._AC_UL320_.jpg)







![PHR Study Guide 2024-2025: 3 Full-Length Practice Tests, Secrets Prep Book for the HRCI PHR Certification Exam: [6th Edition]](https://m.media-amazon.com/images/I/71jgTw5AuLL._AC_UL320_.jpg)