The debate over whether mRNA vaccines are better than inactivated vaccines has gained significant attention, particularly in the context of COVID-19 immunization. mRNA vaccines, such as those developed by Pfizer-BioNTech and Moderna, work by delivering genetic material that instructs cells to produce a harmless piece of the virus, triggering an immune response. In contrast, inactivated vaccines, like Sinovac and Sinopharm, use a killed version of the virus to stimulate immunity. Proponents of mRNA vaccines highlight their higher efficacy rates, ability to induce robust immune responses, and potential for rapid adaptation to new variants. However, inactivated vaccines are often favored for their established safety profile, ease of storage, and familiarity in global vaccination programs. Ultimately, the choice between the two depends on factors such as regional availability, logistical constraints, and individual health considerations, making it essential to weigh the benefits and limitations of each technology.
Explore related products






What You'll Learn
- Efficacy comparison: mRNA vs. inactivated vaccines in preventing COVID-19 infection and severe illness
- Safety profiles: Side effects, allergic reactions, and long-term risks of both vaccine types
- Immunity duration: How long protection lasts with mRNA versus inactivated vaccines
- Variant effectiveness: Performance against emerging COVID-19 variants for both vaccine types
- Storage and distribution: Logistics, stability, and accessibility differences between mRNA and inactivated vaccines
![]()
Efficacy comparison: mRNA vs. inactivated vaccines in preventing COVID-19 infection and severe illness
The COVID-19 pandemic spurred an unprecedented global vaccination effort, with mRNA and inactivated vaccines emerging as leading technologies. Clinical trials and real-world data reveal distinct efficacy profiles for each. mRNA vaccines, such as Pfizer-BioNTech and Moderna, demonstrated higher initial efficacy against symptomatic infection, ranging from 94% to 95% after two doses. In contrast, inactivated vaccines like Sinovac’s CoronaVac showed lower efficacy, typically between 50% and 80%, depending on the population and variant. However, efficacy isn’t the sole measure of success—both vaccine types significantly reduce severe illness and hospitalization, though mRNA vaccines consistently outperform in this regard, particularly against the Delta and Omicron variants.
Consider the dosage and administration differences. mRNA vaccines require lower doses (30 µg for Pfizer, 100 µg for Moderna) and a shorter interval between doses (3–4 weeks) compared to inactivated vaccines, which often require higher doses (e.g., 3 µg for CoronaVac) and longer intervals (4–8 weeks). This affects not only immune response but also logistical challenges in low-resource settings. For instance, mRNA vaccines’ ultra-cold storage requirements initially limited their accessibility, while inactivated vaccines’ stability at standard refrigeration temperatures made them more deployable in developing regions.
Age-specific efficacy further complicates the comparison. mRNA vaccines have shown robust protection across age groups, including older adults, with studies indicating over 90% efficacy in preventing severe disease in individuals over 65. Inactivated vaccines, however, exhibit waning efficacy in this demographic, often dropping below 60% after six months. Booster doses mitigate this decline, but the timing and frequency differ—mRNA boosters are recommended 6 months post-primary series, while inactivated vaccine boosters are often administered earlier, after 3–6 months, to maintain protection.
Practical considerations also influence vaccine choice. mRNA vaccines’ rapid development and adaptability to new variants position them as frontrunners in the evolving pandemic landscape. For example, updated bivalent mRNA boosters targeting Omicron subvariants have shown enhanced neutralizing antibody responses. Inactivated vaccines, while slower to adapt, remain a critical tool in regions with limited access to mRNA options. To maximize protection, individuals should follow local health guidelines, prioritize timely boosters, and consider vaccine availability when making decisions.
In summary, while mRNA vaccines offer superior efficacy against infection and severe illness, inactivated vaccines play a vital role in global vaccination strategies, particularly in resource-constrained settings. The choice between the two depends on factors like age, variant prevalence, and logistical feasibility. Regardless of type, vaccination remains the cornerstone of pandemic control, and staying informed about updates ensures optimal protection.
Does Monzo Hold a UK Banking License? A Comprehensive Guide
You may want to see also
Explore related products






![]()
Safety profiles: Side effects, allergic reactions, and long-term risks of both vaccine types
Both mRNA and inactivated vaccines have undergone rigorous testing, but their safety profiles differ in ways that matter to specific populations. mRNA vaccines, like Pfizer-BioNTech and Moderna, introduce genetic material that prompts cells to produce a viral protein, triggering an immune response. Inactivated vaccines, such as Sinovac’s CoronaVac, use a killed version of the virus to achieve the same goal. While both are generally safe, their side effect profiles vary. mRNA vaccines are more likely to cause short-term reactions like fatigue, headache, and muscle pain, particularly after the second dose. These symptoms, though uncomfortable, are a sign of the immune system responding and typically resolve within a few days. Inactivated vaccines tend to produce milder side effects, such as soreness at the injection site, but are less likely to cause systemic reactions.
Allergic reactions are a critical safety consideration for both vaccine types. mRNA vaccines have a slightly higher risk of immediate allergic reactions, including anaphylaxis, though this remains rare—occurring in approximately 2 to 5 cases per million doses. Individuals with a history of severe allergies to vaccine components, such as polyethylene glycol (PEG) in mRNA vaccines, are advised to consult a healthcare provider before vaccination. Inactivated vaccines have a lower risk of allergic reactions, as they do not contain the same stabilizers or lipids found in mRNA formulations. However, no vaccine is entirely risk-free, and monitoring for symptoms like hives, swelling, or difficulty breathing is essential after any vaccination.
Long-term risks are a common concern, but current data provide reassurance for both vaccine types. mRNA vaccines have been administered to billions of people worldwide since 2020, with no evidence of long-term adverse effects. Their transient nature—the mRNA degrades quickly after vaccination—reduces the likelihood of persistent issues. Inactivated vaccines, with decades of use in other diseases like polio and rabies, have a well-established safety record. However, long-term studies specific to COVID-19 inactivated vaccines are still ongoing, though no red flags have emerged. Both vaccines are considered safe for long-term use, but ongoing surveillance remains crucial.
Practical tips can help manage side effects and minimize risks. For mRNA vaccines, scheduling the second dose on a day when you can rest afterward is advisable, as side effects are often more pronounced. Staying hydrated and using over-the-counter pain relievers like acetaminophen can alleviate discomfort. For inactivated vaccines, applying a cold compress to the injection site can reduce soreness. Regardless of the vaccine type, reporting any severe or persistent symptoms to a healthcare provider is essential. Understanding these safety profiles empowers individuals to make informed decisions and build trust in vaccination programs.
Repos and Bank Balance Sheets: What's the Connection?
You may want to see also
Explore related products






![]()
Immunity duration: How long protection lasts with mRNA versus inactivated vaccines
The duration of immunity provided by vaccines is a critical factor in their effectiveness, especially in the context of rapidly evolving pathogens like SARS-CoV-2. mRNA vaccines, such as Pfizer-BioNTech and Moderna, have demonstrated robust initial immune responses, with studies showing high levels of neutralizing antibodies within weeks of the second dose. However, the longevity of this protection is a subject of ongoing research. Data from real-world studies indicate that mRNA vaccines maintain significant efficacy against severe disease for at least 6 to 8 months, though protection against mild infection may wane more quickly, particularly against emerging variants. For instance, a study published in *The New England Journal of Medicine* found that the Pfizer vaccine’s efficacy against symptomatic infection dropped from 96% to 84% after 4 months, while protection against hospitalization remained above 90%.
In contrast, inactivated vaccines, like Sinovac’s CoronaVac and Sinopharm’s BBIBP-CorV, typically elicit a more moderate immune response, often requiring additional doses to achieve comparable levels of protection. These vaccines rely on whole, inactivated virus particles to stimulate immunity, which can result in a slower and less durable response compared to mRNA vaccines. Studies have shown that inactivated vaccines may provide strong protection for 3 to 6 months, but their efficacy tends to decline more rapidly, particularly in older adults or those with comorbidities. For example, a study in *The Lancet* reported that CoronaVac’s efficacy against symptomatic infection fell to around 50% after 6 months, prompting many countries to recommend booster doses.
Booster shots play a pivotal role in extending immunity for both vaccine types. mRNA boosters, often administered 6 months after the initial series, have been shown to restore and even enhance antibody levels, providing renewed protection against both severe disease and infection. Inactivated vaccine boosters, while effective, may require more frequent administration due to the initial lower immune response. For instance, some countries administering inactivated vaccines have opted for a third dose after 3 to 6 months, followed by additional boosters every 6 months for high-risk populations.
Practical considerations also differ between the two vaccine types. mRNA vaccines, stored at ultra-cold temperatures, are logistically challenging to distribute in resource-limited settings, whereas inactivated vaccines are more stable and easier to transport. This has influenced global vaccination strategies, with inactivated vaccines being widely used in low- and middle-income countries. However, the need for more frequent boosters with inactivated vaccines can strain healthcare systems, underscoring the importance of balancing accessibility with long-term efficacy.
In summary, mRNA vaccines generally provide longer-lasting protection against severe disease, with immunity lasting at least 6 to 8 months, while inactivated vaccines may require more frequent boosters to maintain efficacy. Both types have their strengths and limitations, and the choice between them often depends on factors like availability, infrastructure, and population-specific needs. As research continues, understanding these differences will be crucial for optimizing global vaccination strategies and ensuring sustained immunity against evolving pathogens.
Step-by-Step Guide to Creating a Bank of America Bank Draft
You may want to see also
Explore related products

$26.9 $43.96





![]()
Variant effectiveness: Performance against emerging COVID-19 variants for both vaccine types
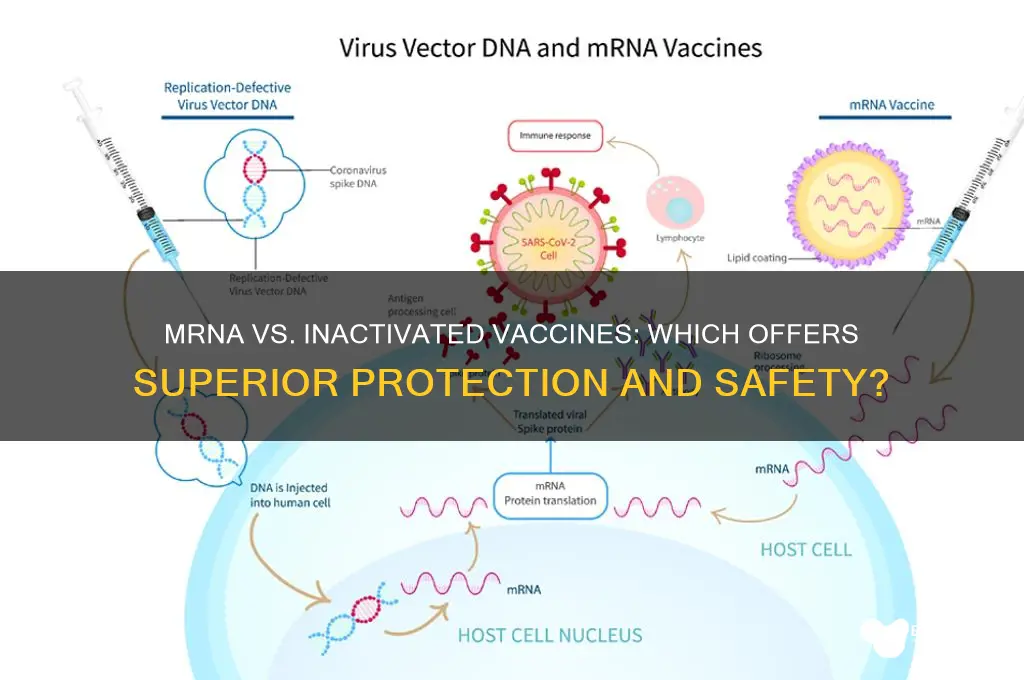
The emergence of COVID-19 variants has raised critical questions about vaccine effectiveness, particularly when comparing mRNA and inactivated vaccines. While both types have demonstrated robust protection against the original SARS-CoV-2 strain, their performance against variants like Delta and Omicron varies significantly. mRNA vaccines, such as Pfizer-BioNTech and Moderna, rely on genetic material to instruct cells to produce a spike protein, triggering an immune response. Inactivated vaccines, like Sinovac’s CoronaVac, use a killed version of the virus to elicit immunity. This fundamental difference in mechanism influences how each vaccine adapts to mutations in the virus.
Consider the Omicron variant, which carries over 30 mutations in the spike protein. Studies show that mRNA vaccines maintain higher neutralizing antibody levels against Omicron after a booster dose, with efficacy against severe disease remaining above 75% in adults. For instance, a third dose of Pfizer’s mRNA vaccine (30 µg) restores protection to levels comparable to the original strain. In contrast, inactivated vaccines exhibit a more pronounced drop in efficacy against Omicron, with studies indicating a 50-60% reduction in neutralizing antibodies after two doses. However, a heterologous booster (e.g., an mRNA dose following inactivated vaccine priming) can significantly enhance protection, particularly in older adults and immunocompromised individuals.
The age factor plays a crucial role in variant effectiveness. For individuals over 65, mRNA vaccines consistently outperform inactivated vaccines in preventing hospitalization and death across variants. This is partly due to the stronger and more durable T-cell response generated by mRNA technology. Younger populations, however, may achieve adequate protection with either vaccine type, though mRNA vaccines still offer a slight edge in preventing symptomatic infection. Practical tip: If you’ve received an inactivated vaccine, consider an mRNA booster to broaden your immune response against emerging variants.
A comparative analysis of real-world data from countries like Chile and the UAE highlights the impact of vaccine type on variant control. Chile, which primarily used Sinovac’s inactivated vaccine, experienced a surge in Delta cases despite high vaccination rates, prompting a mass mRNA booster campaign. Conversely, the UAE, which deployed a mix of Pfizer and Sinopharm, saw milder Omicron waves due to strategic booster rollouts. This underscores the importance of vaccine flexibility and the need for ongoing surveillance to tailor immunization strategies to local variant prevalence.
In conclusion, while both mRNA and inactivated vaccines remain essential tools in the fight against COVID-19, mRNA vaccines demonstrate superior adaptability to emerging variants, particularly after a booster dose. Inactivated vaccines, though less effective against mutations, can be optimized through heterologous boosting. For policymakers and individuals alike, the key takeaway is to prioritize booster doses and consider vaccine type in the context of local variant circulation. This approach ensures sustained protection and minimizes the risk of severe outcomes across all age groups.
Global Banking Access: How Many People Have Financial Services?
You may want to see also
Explore related products






![]()
Storage and distribution: Logistics, stability, and accessibility differences between mRNA and inactivated vaccines
One of the most striking differences between mRNA and inactivated vaccines lies in their storage requirements. mRNA vaccines, such as Pfizer-BioNTech and Moderna, demand ultra-cold temperatures, typically between -60°C and -80°C for long-term storage. This necessity stems from the fragile nature of mRNA molecules, which degrade rapidly at warmer temperatures. In contrast, inactivated vaccines, like Sinovac’s CoronaVac or Sinopharm’s BBIBP-CorV, are far more stable, requiring standard refrigeration temperatures of 2°C to 8°C. This disparity creates a logistical chasm, particularly in low-resource settings where ultra-cold chain infrastructure is scarce or nonexistent. For instance, distributing Pfizer’s vaccine to remote areas in Africa or Southeast Asia often requires specialized freezers and dry ice, significantly increasing costs and complexity.
Consider the practical implications for healthcare workers. Administering an mRNA vaccine involves a delicate dance: vials must be thawed, diluted (for Pfizer’s vaccine), and used within 6 hours after removal from refrigeration. Inactivated vaccines, however, can be stored in a regular fridge for months and are ready for use without additional preparation. This simplicity makes inactivated vaccines more accessible in rural clinics or during mass vaccination campaigns. For example, a nurse in a village without reliable electricity can still administer an inactivated vaccine safely, whereas an mRNA vaccine might spoil before reaching the patient.
Stability also affects dosage and wastage. mRNA vaccines often come in multi-dose vials, with Pfizer’s vials containing up to 6 doses and Moderna’s up to 10. Once opened, these vials must be used within a short window, or the remaining doses are wasted. Inactivated vaccines, typically packaged in single-dose vials, eliminate this risk. This difference is critical in regions with fluctuating demand or limited healthcare staff. A clinic in a sparsely populated area might struggle to use all doses in an mRNA vial before expiration, whereas inactivated vaccines offer flexibility without compromising efficacy.
Accessibility is further complicated by global distribution inequities. Wealthier nations with robust cold chain systems can prioritize mRNA vaccines, while lower-income countries often rely on inactivated vaccines due to their logistical feasibility. For instance, COVAX, the global vaccine-sharing initiative, has distributed millions of inactivated doses to countries like Nepal and Ghana, where mRNA vaccines remain out of reach. This disparity highlights a moral dilemma: while mRNA vaccines boast higher efficacy rates (around 90–95% for Pfizer and Moderna vs. 50–80% for inactivated vaccines), their inaccessibility in many regions undermines global herd immunity efforts.
In conclusion, the choice between mRNA and inactivated vaccines is not merely scientific but deeply logistical. mRNA vaccines offer superior efficacy but demand a logistical ballet of ultra-cold storage and rapid administration. Inactivated vaccines, though less efficacious, provide stability, simplicity, and accessibility, making them indispensable in resource-constrained settings. Policymakers and healthcare providers must weigh these trade-offs, ensuring that vaccine distribution strategies align with local infrastructure and population needs. After all, the best vaccine is the one that reaches the arm—not the one that spoils in transit.
Buying Half Dollars from Banks: A Step-by-Step Guide for Collectors
You may want to see also
Frequently asked questions
Both mRNA and inactivated vaccines are highly effective in preventing severe illness, hospitalization, and death from COVID-19. However, studies suggest that mRNA vaccines (like Pfizer-BioNTech and Moderna) may offer slightly higher efficacy rates, especially against symptomatic infection, compared to inactivated vaccines.
Both types of vaccines have been rigorously tested and are considered safe for use. mRNA vaccines have a well-documented safety profile, with common side effects like fatigue, headache, and soreness. Inactivated vaccines also have a long history of safe use, with similar mild side effects. Serious adverse reactions are rare for both.
mRNA vaccines generally provide longer-lasting immunity compared to inactivated vaccines. Booster doses are often recommended for both, but studies indicate that mRNA vaccines may maintain higher antibody levels over time, offering more sustained protection.
No, mRNA vaccines do not alter your DNA. They work by delivering genetic instructions to cells to produce a harmless protein that triggers an immune response. Inactivated vaccines, on the other hand, use a killed version of the virus. Neither vaccine type can change your genetic makeup.