Pneumonia and RSV (Respiratory Syncytial Virus) are both respiratory infections, but they are caused by different pathogens, and as a result, the vaccines designed to prevent them are distinct. The pneumonia vaccine, such as the pneumococcal conjugate vaccine (PCV13) or pneumococcal polysaccharide vaccine (PPSV23), targets specific strains of Streptococcus pneumoniae bacteria, a common cause of bacterial pneumonia. In contrast, the RSV vaccine, which has recently been developed for older adults and is under investigation for infants, focuses on preventing infections caused by the respiratory syncytial virus. While both vaccines aim to protect against serious respiratory illnesses, they are not interchangeable, and individuals may need both depending on their age, health status, and risk factors.
Explore related products






What You'll Learn
- Vaccine Composition Differences: Pneumonia vaccines target pneumococcal bacteria; RSV vaccines target respiratory syncytial virus
- Targeted Age Groups: Pneumonia vaccines for all ages; RSV vaccines primarily for infants, elderly
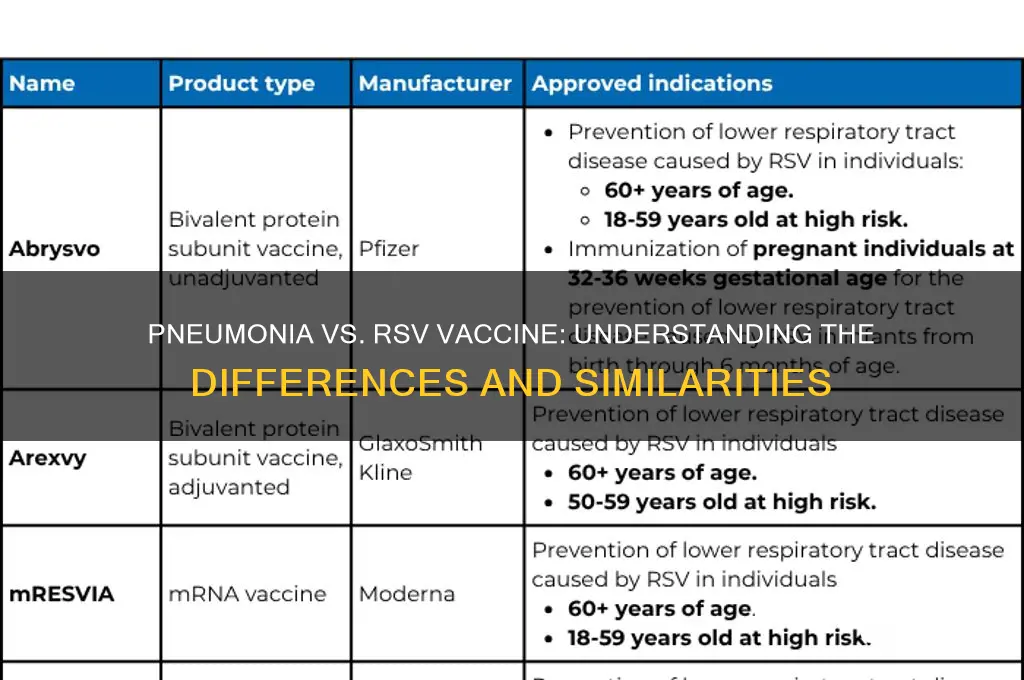
- Vaccine Types Available: Pneumonia: PCV13, PPSV23; RSV: nirsevimab, arexvy
- Immune Response Focus: Pneumonia vaccines prevent bacterial infections; RSV vaccines prevent viral infections
- Administration Timing: Pneumonia vaccines often routine; RSV vaccines seasonal or high-risk specific
![]()
Vaccine Composition Differences: Pneumonia vaccines target pneumococcal bacteria; RSV vaccines target respiratory syncytial virus
Pneumonia and RSV vaccines are distinct in their composition and purpose, primarily because they target different pathogens. Pneumonia vaccines, such as Prevnar 13 (PCV13) and Pneumovax 23 (PPSV23), are designed to protect against *Streptococcus pneumoniae*, a bacterium responsible for pneumococcal pneumonia. These vaccines contain purified polysaccharides or conjugated polysaccharides from the bacterial capsule, which stimulate the immune system to recognize and combat the bacteria. For instance, PCV13 covers 13 serotypes of *S. pneumoniae* and is recommended for children under 2 years, adults over 65, and immunocompromised individuals, typically administered as a 2- to 4-dose series depending on age and risk factors.
In contrast, RSV vaccines target the respiratory syncytial virus, a common viral cause of respiratory infections, particularly in infants, older adults, and immunocompromised individuals. RSV vaccines, such as Arexvy and Abrysvo, are protein subunit vaccines that contain the stabilized prefusion F protein of the virus. This protein is crucial for viral entry into host cells, and by targeting it, the vaccine elicits a robust neutralizing antibody response. Arexvy, approved for adults 60 and older, is administered as a single 0.5 mL dose, while Abrysvo is used for maternal immunization to protect newborns through passive antibody transfer.
The differences in vaccine composition reflect the distinct biology of their targets. Bacterial vaccines often rely on polysaccharides or conjugated antigens to mimic the bacterial surface, whereas viral vaccines typically use viral proteins or genetic material to induce immunity. This divergence necessitates tailored vaccination strategies, such as the use of adjuvants in RSV vaccines to enhance immune responses to the viral protein.
Practically, these differences mean that individuals at risk for both pneumococcal pneumonia and RSV may require separate vaccinations. For example, an older adult might receive both PCV13 and Arexvy, but these vaccines cannot be combined into a single dose due to their unique formulations. Understanding these distinctions is crucial for healthcare providers to recommend appropriate immunizations based on patient age, health status, and risk factors.
In summary, while both pneumonia and RSV vaccines aim to prevent respiratory infections, their compositions and targets are fundamentally different. Pneumonia vaccines focus on pneumococcal bacteria using polysaccharide-based antigens, whereas RSV vaccines target the viral F protein. This specificity underscores the importance of administering the correct vaccine to the right population, ensuring optimal protection against these distinct but significant respiratory pathogens.
Securely Adding Bank Details to Eventbrite: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Targeted Age Groups: Pneumonia vaccines for all ages; RSV vaccines primarily for infants, elderly
Pneumonia and RSV (Respiratory Syncytial Virus) vaccines, while both targeting respiratory infections, are tailored to protect distinct age groups. Pneumonia vaccines, such as the pneumococcal conjugate vaccine (PCV13) and pneumococcal polysaccharide vaccine (PPSV23), are recommended across all age groups. For infants, PCV13 is administered in a series of doses starting at 2 months, with boosters at 4, 6, and 12–15 months. Adults, particularly those over 65, receive PPSV23, often after a dose of PCV13, to broaden protection against pneumococcal strains. This universal approach reflects the widespread risk of pneumonia across the lifespan.
In contrast, RSV vaccines are primarily targeted at infants and the elderly, the populations most vulnerable to severe RSV infections. For infants, monoclonal antibody treatments like palivizumab are used prophylactically during RSV season, typically from November to March. These injections are given monthly to high-risk infants, such as preterm babies or those with heart or lung conditions. Recently approved RSV vaccines for pregnant individuals, like Pfizer’s Abrysvo, offer passive immunity to newborns by transferring maternal antibodies, providing protection during the first 6 months of life.
The elderly, particularly those over 60 with comorbidities, are another key focus for RSV vaccines. New vaccines like GSK’s Arexvy and Pfizer’s Abrysvo are administered as a single dose to reduce the risk of severe RSV-related illnesses, such as pneumonia and bronchitis. Unlike pneumonia vaccines, RSV vaccines are not yet recommended for the general adult population, highlighting their targeted approach to high-risk groups.
Practical considerations for caregivers and healthcare providers include timing RSV prophylaxis for infants during peak season and ensuring elderly patients receive RSV vaccines alongside their annual flu shots. For pneumonia vaccines, adherence to the recommended schedule is crucial, especially for children and older adults. Parents should consult pediatricians to confirm their child’s vaccination status, while seniors should discuss pneumococcal and RSV vaccination with their primary care provider to address age-specific risks.
In summary, while pneumonia vaccines offer broad protection across all ages, RSV vaccines are strategically focused on infants and the elderly, addressing their heightened susceptibility to severe outcomes. Understanding these distinctions ensures appropriate vaccine utilization, maximizing protection for those most at risk.
US Vaccine Distribution: Tracking the Number of Doses Delivered
You may want to see also
Explore related products






![]()
Vaccine Types Available: Pneumonia: PCV13, PPSV23; RSV: nirsevimab, arexvy
Pneumonia and RSV (Respiratory Syncytial Virus) are distinct respiratory infections, each requiring specific vaccines for prevention. While both target the respiratory system, the vaccines available for pneumonia and RSV differ in composition, mechanism, and target populations. Understanding these differences is crucial for informed decision-making and optimal protection.
For pneumonia, two primary vaccines are available: PCV13 (Pneumococcal Conjugate Vaccine) and PPSV23 (Pneumococcal Polysaccharide Vaccine). PCV13 is recommended for children under 2 years old, adults over 65, and individuals with certain medical conditions. It covers 13 strains of pneumococcus and is administered as a series of doses, typically 0.5 mL intramuscularly. PPSV23, on the other hand, protects against 23 strains and is advised for adults over 65 and younger individuals with high-risk conditions. A single 0.5 mL dose is given, often in combination with PCV13 for broader coverage. These vaccines primarily target *Streptococcus pneumoniae*, a leading bacterial cause of pneumonia.
In contrast, RSV vaccines are a newer development, with nirsevimab and Arexvy leading the way. Nirsevimab is a monoclonal antibody designed for infants under 12 months, providing immediate protection during their first RSV season. A single 500 mg intramuscular dose is administered, ideally before RSV season peaks. Arexvy, the first RSV vaccine approved for adults over 60, offers active immunization. It is given as a single 0.5 mL dose and targets the RSV F protein, preventing severe disease. These vaccines address RSV, a viral pathogen, rather than bacterial causes like pneumococcus.
A key distinction lies in the vaccines' mechanisms. Pneumonia vaccines (PCV13 and PPSV23) stimulate the immune system to produce antibodies against pneumococcal bacteria, while RSV vaccines (nirsevimab and Arexvy) either provide direct antibody protection (nirsevimab) or induce an immune response to RSV proteins (Arexvy). This difference highlights the tailored approach required for viral versus bacterial infections.
Practical considerations include timing and eligibility. Pneumonia vaccines are often part of routine immunization schedules, with PCV13 given in infancy and PPSV23 recommended later in life. RSV vaccines, however, are seasonal and targeted. Nirsevimab is best administered before RSV season, typically fall to winter, while Arexvy can be given year-round to eligible adults. Consulting healthcare providers ensures appropriate timing and dosage, especially for those with comorbidities or immunocompromised states.
In summary, while pneumonia and RSV vaccines both protect against respiratory infections, they are not interchangeable. Pneumonia vaccines (PCV13, PPSV23) target bacterial strains, whereas RSV vaccines (nirsevimab, Arexvy) address a viral pathogen. Each has specific indications, dosages, and mechanisms, underscoring the importance of tailored vaccination strategies for optimal respiratory health.
Track Your Axis Bank FASTag Status Easily: A Quick Guide
You may want to see also
Explore related products






![]()
Immune Response Focus: Pneumonia vaccines prevent bacterial infections; RSV vaccines prevent viral infections
Pneumonia vaccines and RSV vaccines target distinct pathogens, necessitating different immune responses. Pneumonia vaccines, such as the pneumococcal conjugate vaccine (PCV13) and pneumococcal polysaccharide vaccine (PPSV23), primarily combat bacterial infections caused by *Streptococcus pneumoniae*. These vaccines stimulate the production of antibodies against the bacterium’s polysaccharide capsule, a key virulence factor. For instance, PCV13 is recommended for children under 2 years old in a 4-dose series (at 2, 4, 6, and 12–15 months) and for adults 65 and older as a one-time dose, often followed by PPSV23 a year later. In contrast, RSV vaccines, like the recently approved Arexvy and Abrysvo, target respiratory syncytial virus, a viral pathogen. These vaccines induce neutralizing antibodies against the RSV fusion (F) protein, preventing viral entry into host cells. Arexvy is administered as a single 0.5 mL intramuscular dose for adults 60 and older, while Abrysvo is approved for pregnant individuals at 32–36 weeks’ gestation to protect newborns via maternal antibodies.
The immune mechanisms triggered by these vaccines reflect their pathogen-specific designs. Pneumonia vaccines rely on T-cell-independent responses, as the bacterial polysaccharides directly activate B cells to produce antibodies. This is why multiple doses are often needed to achieve robust immunity, particularly in young children and older adults whose immune systems may be less responsive. RSV vaccines, however, elicit a T-cell-dependent response, as the viral protein antigens require processing and presentation by antigen-presenting cells. This pathway typically results in longer-lasting immunity, though RSV’s ability to evade immune memory has historically complicated vaccine development. For example, natural RSV infection provides only partial and temporary protection, underscoring the need for a targeted vaccine approach.
A critical distinction lies in the populations most vulnerable to these infections. Pneumonia vaccines are prioritized for high-risk groups, including infants, older adults, and immunocompromised individuals, as *S. pneumoniae* can cause severe complications like bacteremia and meningitis. RSV vaccines, however, focus on protecting the very young and the elderly, as RSV is a leading cause of bronchiolitis in infants and severe respiratory illness in older adults. Pregnant individuals are also targeted to confer passive immunity to newborns, who are too young to receive the vaccine directly. This tailored approach highlights the importance of understanding the pathogen’s epidemiology and immune evasion strategies.
Practical considerations further differentiate these vaccines. Pneumonia vaccines often require booster doses to maintain immunity, particularly in older adults whose immune responses wane over time. RSV vaccines, while currently single-dose for most populations, may need to account for viral mutations in future iterations, similar to influenza vaccines. For healthcare providers, ensuring proper vaccine storage (e.g., refrigeration at 2–8°C) and administration technique (intramuscular injection for both) is crucial. Patients should be educated about potential side effects, such as injection site pain or fatigue, which are generally mild and short-lived.
In summary, while both pneumonia and RSV vaccines aim to prevent respiratory infections, their immune response focus, target populations, and practical applications differ significantly. Pneumonia vaccines combat bacterial pathogens through polysaccharide-targeted antibodies, requiring multiple doses for certain groups. RSV vaccines, on the other hand, neutralize a viral threat by inducing protein-specific immunity, often in a single dose. Understanding these distinctions is essential for healthcare providers and patients alike to optimize protection against these distinct yet equally serious respiratory threats.
Exploring Bank Interiors: Design, Security, and Customer Experience Inside
You may want to see also
Explore related products






![]()
Administration Timing: Pneumonia vaccines often routine; RSV vaccines seasonal or high-risk specific
Pneumonia vaccines, such as the pneumococcal conjugate vaccine (PCV13) and the pneumococcal polysaccharide vaccine (PPSV23), are typically administered as part of routine immunization schedules. For infants, PCV13 is given in a series of doses at 2, 4, 6, and 12–15 months of age, ensuring early protection against pneumococcal bacteria. Adults aged 65 and older receive a single dose of PCV13 followed by a dose of PPSV23 a year later, or vice versa, depending on their medical history. This routine approach reflects the persistent threat of pneumococcal disease across all age groups, making consistent vaccination a cornerstone of public health strategies.
In contrast, RSV vaccines are administered seasonally or to high-risk populations due to the virus’s cyclical nature. RSV infections peak during fall and winter, prompting targeted vaccination campaigns during these months. For example, the RSV vaccine nirsevimab is recommended for all infants under 8 months entering their first RSV season, providing immediate protection during the most vulnerable period. High-risk groups, such as premature infants, children with congenital heart disease, or older adults with chronic conditions, may receive RSV vaccines regardless of the season, as their risk of severe illness remains elevated year-round.
The timing of RSV vaccination also differs from pneumonia vaccines in its specificity. While pneumonia vaccines are administered based on age milestones or chronic conditions, RSV vaccines are often tied to epidemiological data, such as local RSV activity. Healthcare providers may use tools like the CDC’s RSV surveillance reports to determine the optimal window for vaccination. For instance, in regions where RSV peaks in December, vaccination in October or November ensures immunity during the highest-risk period.
Practical considerations further highlight the differences in administration timing. Pneumonia vaccines can be integrated into routine healthcare visits, such as well-child checks or annual physicals, making them convenient for patients. RSV vaccines, however, require proactive planning. Parents of infants or caregivers of high-risk individuals must coordinate with healthcare providers to ensure vaccination aligns with seasonal risks. For older adults, combining RSV vaccination with flu shots during fall health campaigns can streamline protection against multiple respiratory threats.
Ultimately, understanding these timing differences empowers individuals and healthcare providers to maximize vaccine efficacy. Pneumonia vaccines’ routine administration ensures broad, consistent coverage, while RSV vaccines’ seasonal or risk-based approach targets the most vulnerable populations during periods of highest risk. By tailoring vaccination strategies to the unique characteristics of each disease, public health efforts can more effectively prevent severe illness and reduce healthcare burdens.
Massachusetts Foreclosure Timeline: How Soon Can Banks Take Your Home?
You may want to see also
Frequently asked questions
No, the pneumonia vaccine and the RSV vaccine are different. The pneumonia vaccine protects against pneumococcal bacteria, which can cause pneumonia, while the RSV vaccine targets respiratory syncytial virus (RSV), a common cause of respiratory infections.
No, the pneumonia vaccine does not protect against RSV infections. It specifically targets pneumococcal bacteria, whereas RSV is a virus requiring a separate vaccine for prevention.
They are not typically given together but may be recommended for certain individuals, especially older adults or those with high-risk conditions, based on their healthcare provider’s advice. Always consult a doctor for personalized recommendations.