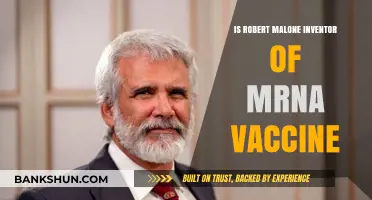
Remicade, also known as infliximab, is a biologic medication used to treat various autoimmune conditions such as rheumatoid arthritis, Crohn's disease, and ulcerative colitis. It is not a protein vaccine or an antibody in the traditional sense but rather a monoclonal antibody. Monoclonal antibodies are laboratory-produced molecules engineered to serve as substitute antibodies that can restore, enhance, or mimic the immune system's attack on unhealthy cells. Remicade specifically targets and neutralizes tumor necrosis factor-alpha (TNF-α), a protein involved in inflammation, thereby reducing the symptoms of autoimmune diseases. Unlike vaccines, which stimulate the immune system to produce its own antibodies, Remicade directly provides the therapeutic antibody to the patient. Understanding its classification as a monoclonal antibody is crucial for distinguishing it from vaccines and other immunological treatments.
Explore related products






What You'll Learn
- Remicade's classification: Is it a protein vaccine or monoclonal antibody
- Mechanism of action: How Remicade differs from traditional vaccines
- Composition analysis: What makes Remicade an antibody, not a vaccine
- Therapeutic use: Remicade as a biologic, not a vaccine
- Manufacturing process: Why Remicade is produced as an antibody, not a vaccine
![]()
Remicade's classification: Is it a protein vaccine or monoclonal antibody?
Remicade, known generically as infliximab, is a biologic medication primarily used to treat autoimmune conditions such as rheumatoid arthritis, Crohn’s disease, and ulcerative colitis. Its classification is often misunderstood, with some confusing it for a protein vaccine. However, Remicade is not a vaccine; it does not stimulate the immune system to produce antibodies against a pathogen. Instead, it is a monoclonal antibody, a laboratory-produced molecule engineered to target specific proteins in the body. This distinction is critical for understanding its mechanism of action and appropriate use.
To clarify, monoclonal antibodies like Remicade are designed to bind to a single, specific target, in this case, tumor necrosis factor-alpha (TNF-α), a protein involved in inflammation. By neutralizing TNF-α, Remicade reduces inflammation and alleviates symptoms in autoimmune diseases. Protein vaccines, on the other hand, introduce a harmless protein or protein fragment to the immune system, prompting it to generate a protective immune response. For example, the HPV vaccine uses a virus-like particle (a protein) to induce immunity. Remicade’s role is therapeutic, not preventive, and it acts directly on the immune system rather than training it to respond to future threats.
A key practical difference lies in administration and dosage. Remicade is administered intravenously, typically in a clinical setting, with dosages tailored to the patient’s weight and condition. For instance, adults with rheumatoid arthritis often receive an initial dose of 3 mg/kg, followed by additional doses at weeks 2 and 6, then every 8 weeks thereafter. In contrast, protein vaccines are usually given intramuscularly or subcutaneously in standardized doses, often in a series (e.g., two or three shots over several months). Remicade’s dosing regimen underscores its role as a targeted therapy, not a vaccine.
From a comparative standpoint, while both monoclonal antibodies and protein vaccines are biologics, their purposes and mechanisms diverge. Monoclonal antibodies like Remicade are used to treat active disease by modulating the immune response in real-time. Protein vaccines, such as the shingles vaccine, prevent disease by preparing the immune system for future encounters with pathogens. This fundamental difference highlights why Remicade is not a vaccine but a powerful tool for managing chronic inflammatory conditions.
In conclusion, Remicade’s classification as a monoclonal antibody is clear when its mechanism, administration, and purpose are examined. Patients and healthcare providers must understand this distinction to ensure appropriate use and avoid confusion with vaccines. For those prescribed Remicade, adherence to the dosing schedule and monitoring for potential side effects, such as infections or infusion reactions, are essential for optimal outcomes. This clarity not only enhances treatment efficacy but also reinforces the importance of precise medical terminology in patient care.
Does the World Bank Comply with U.S. Labor Laws?
You may want to see also
Explore related products

$134 $167.95





![]()
Mechanism of action: How Remicade differs from traditional vaccines
Remicade, unlike traditional vaccines, is not designed to stimulate the immune system to produce antibodies against a specific pathogen. Instead, it is a monoclonal antibody therapy that directly targets and neutralizes a specific protein in the body, namely tumor necrosis factor-alpha (TNF-α). This mechanism of action sets Remicade apart from protein vaccines, which typically introduce a harmless piece of a pathogen to trigger an immune response.
To understand the difference, consider the process of vaccination. Traditional vaccines, such as those for influenza or measles, contain weakened or inactivated pathogens, or specific proteins from these pathogens, which prompt the immune system to produce antibodies and memory cells. These antibodies and cells then provide future protection against the actual disease-causing agent. In contrast, Remicade is administered intravenously in a clinical setting, with dosages tailored to the patient's weight and condition. For example, in adults with rheumatoid arthritis, the initial dose is typically 3 mg/kg, followed by additional doses at 2 and 6 weeks, and then every 8 weeks thereafter. This targeted approach allows Remicade to modulate the immune response by binding to TNF-α, a cytokine that plays a key role in inflammation, thereby reducing its activity.
The distinction between Remicade and traditional vaccines becomes clearer when examining their applications. While vaccines are primarily used for prevention, Remicade is employed as a treatment for chronic inflammatory conditions like Crohn's disease, ulcerative colitis, rheumatoid arthritis, and ankylosing spondylitis. Its mechanism of action is particularly effective in these cases because it addresses the underlying cause of inflammation rather than merely alleviating symptoms. For instance, in pediatric patients (ages 6 and older) with moderately to severely active Crohn's disease, Remicade has been shown to induce and maintain clinical remission, with dosages adjusted based on body weight and disease severity.
A critical aspect of Remicade's mechanism is its ability to provide rapid relief, often within weeks of the first infusion. This is in stark contrast to vaccines, which may take weeks or months to confer full immunity. However, this rapid action also necessitates careful monitoring for potential side effects, such as infections or allergic reactions. Patients receiving Remicade should be educated about the importance of reporting any unusual symptoms promptly. Additionally, healthcare providers must consider the patient's medical history, particularly any prior exposure to tuberculosis or other infections, before initiating treatment.
In summary, Remicade's mechanism of action as a monoclonal antibody therapy offers a distinct approach compared to traditional protein vaccines. By directly targeting TNF-α, it provides a tailored treatment for chronic inflammatory conditions, offering rapid relief and improved quality of life for patients. Understanding these differences is crucial for healthcare professionals and patients alike, ensuring appropriate use and management of this powerful therapeutic tool. Practical considerations, such as dosage adjustments and vigilant monitoring, further underscore the unique role of Remicade in modern medicine.
Mechanics Bank Yreka CA: Identifying the Correct Branch Location
You may want to see also
Explore related products

$128.4 $159


![Birth of new drug Actemra - antibody drug of Japan's first (Iwanami Library of Science) (2013) ISBN: 4000296051 [Japanese Import]](https://m.media-amazon.com/images/I/71+JlHvPNGL._AC_UL320_.jpg)


![]()
Composition analysis: What makes Remicade an antibody, not a vaccine
Remicade, known generically as infliximab, is a biologic medication classified as a monoclonal antibody, not a vaccine. This distinction is rooted in its molecular composition and mechanism of action. Unlike vaccines, which typically contain antigens or weakened pathogens to stimulate the immune system to produce antibodies, Remicade is itself an antibody. Specifically, it is a chimeric IgG1 antibody, meaning it is engineered from both mouse and human proteins to target tumor necrosis factor-alpha (TNF-α), a cytokine involved in inflammation. This targeted approach differentiates it from vaccines, which aim to prevent disease by priming the immune system rather than directly neutralizing a specific molecule.
The composition of Remicade is a key factor in its classification. It is produced using recombinant DNA technology in Chinese hamster ovary cells, resulting in a complex protein structure that mimics the body’s natural antibodies. Each dose contains 100 mg of infliximab in a sterile, lyophilized powder form, which is reconstituted with sterile water before intravenous administration. Vaccines, in contrast, often consist of simpler components like purified proteins, inactivated viruses, or mRNA sequences, designed to elicit an immune response rather than act as an immune effector themselves.
Another critical aspect is the mode of action. Remicade binds directly to TNF-α, neutralizing its pro-inflammatory effects and reducing tissue damage in conditions like rheumatoid arthritis, Crohn’s disease, and ulcerative colitis. This immediate therapeutic effect contrasts with vaccines, which require time to stimulate the production of antibodies or immune memory. For instance, a vaccine might take weeks to confer protection, whereas Remicade’s effects are evident within hours to days after infusion, depending on the condition being treated.
Practical considerations further highlight the differences. Remicade is administered via intravenous infusion, typically at doses of 3–5 mg/kg body weight, with intervals of 8 weeks after initial induction. Patients must be monitored for infusion reactions and infections due to its immunosuppressive nature. Vaccines, on the other hand, are often given intramuscularly or subcutaneously, with dosing schedules designed to build long-term immunity rather than provide immediate symptom relief. For example, a COVID-19 vaccine might require two doses spaced 3–4 weeks apart, followed by boosters every 6–12 months.
In summary, Remicade’s classification as an antibody, not a vaccine, stems from its engineered protein structure, direct neutralization of TNF-α, and immediate therapeutic effects. Understanding these distinctions is crucial for healthcare providers and patients, as it informs treatment decisions, dosing regimens, and expectations for outcomes. While both antibodies and vaccines play vital roles in medicine, their purposes, compositions, and mechanisms are fundamentally different.
Trump's Gift to Banks: Deregulation and Tax Cuts
You may want to see also
Explore related products






![]()
Therapeutic use: Remicade as a biologic, not a vaccine
Remicade, known generically as infliximab, is a biologic therapy, not a vaccine. This distinction is crucial for understanding its therapeutic use and mechanism of action. Unlike vaccines, which stimulate the immune system to produce antibodies against specific pathogens, Remicade is a monoclonal antibody designed to target and neutralize a specific protein in the body, tumor necrosis factor-alpha (TNF-α). This protein plays a key role in inflammation, making Remicade effective in treating autoimmune conditions such as rheumatoid arthritis, Crohn’s disease, and ulcerative colitis. Its classification as a biologic underscores its role as a targeted therapy rather than a preventive measure like vaccines.
The administration of Remicade involves intravenous infusion, typically in a clinical setting, with dosages tailored to the patient’s condition and weight. For example, in rheumatoid arthritis, the initial dose is often 3 mg/kg, followed by additional infusions at weeks 2 and 6, and then every 8 weeks thereafter. Patients with Crohn’s disease may receive a higher initial dose of 5 mg/kg, followed by the same maintenance schedule. It’s essential for healthcare providers to monitor patients during and after infusion for potential adverse reactions, such as allergic responses or infections, as biologics like Remicade suppress specific immune pathways.
One of the key advantages of Remicade is its ability to provide rapid and sustained relief in conditions where traditional therapies have failed. For instance, in moderate to severe Crohn’s disease, studies show that Remicade induces remission in up to 80% of patients within 14 weeks. However, its use is not without challenges. Long-term therapy may lead to the development of anti-drug antibodies, reducing its effectiveness. To mitigate this, Remicade is often paired with immunomodulators like methotrexate, which help maintain its efficacy and reduce the risk of infusion reactions.
Comparatively, while vaccines are prophylactic and administered to healthy individuals to prevent disease, Remicade is prescribed to patients already suffering from chronic conditions. Its biologic nature allows it to directly intervene in disease processes by blocking TNF-α, a cytokine that drives inflammation. This targeted approach distinguishes it from vaccines, which rely on the body’s immune response to generate protection. Understanding this difference is vital for patients and clinicians to manage expectations and optimize treatment outcomes.
Practical tips for patients on Remicade include maintaining open communication with healthcare providers about side effects, adhering strictly to the infusion schedule, and avoiding live vaccines during treatment due to immunosuppression. Additionally, patients should be aware of signs of infection, such as fever or persistent cough, and seek medical attention promptly. While Remicade is not a cure, its role as a biologic offers significant therapeutic benefits for those with debilitating autoimmune diseases, improving quality of life and reducing disease activity when used appropriately.
Best Free Bank Options for Cash App Users to Save Money
You may want to see also
Explore related products






![]()
Manufacturing process: Why Remicade is produced as an antibody, not a vaccine
Remicade, known generically as infliximab, is a monoclonal antibody, not a vaccine. This distinction is rooted in its manufacturing process and intended function. Unlike vaccines, which stimulate the immune system to produce antibodies against a specific pathogen, Remicade is an antibody itself, engineered to directly target and neutralize tumor necrosis factor-alpha (TNF-α), a protein involved in inflammation. This fundamental difference in mechanism dictates its production as a biologic therapy rather than a vaccine.
The manufacturing process for Remicade begins with the cultivation of mammalian cells, typically Chinese hamster ovary (CHO) cells, which are genetically modified to express the infliximab antibody. These cells are grown in bioreactors under tightly controlled conditions, including temperature, pH, and nutrient levels, to optimize antibody production. The process is highly complex and requires sterile environments to prevent contamination. Once the cells have produced sufficient quantities of the antibody, it is harvested, purified, and formulated into the final drug product. This involves multiple steps, including filtration, chromatography, and concentration, to ensure the antibody is pure and stable.
Producing Remicade as an antibody rather than a vaccine offers several advantages. First, it allows for precise targeting of TNF-α, a key driver of autoimmune diseases like rheumatoid arthritis and Crohn’s disease. Vaccines, in contrast, rely on the body’s immune response, which can be variable and less predictable. Second, as a biologic therapy, Remicade can be administered directly at therapeutic doses—typically 3–5 mg/kg intravenously—to achieve immediate effects, whereas vaccines require time for the immune system to mount a response. This makes Remicade more suitable for acute and chronic conditions requiring rapid intervention.
Another critical factor is the scalability and consistency of the manufacturing process. Monoclonal antibodies like Remicade are produced using standardized cell lines and bioreactor systems, ensuring batch-to-batch uniformity. Vaccines, particularly protein-based ones, often rely on more variable processes, such as recombinant protein expression in bacteria or yeast, which can introduce inconsistencies. For Remicade, the use of mammalian cells ensures proper protein folding and glycosylation, critical for its efficacy and safety.
In summary, Remicade is produced as an antibody, not a vaccine, because its manufacturing process and therapeutic mechanism are tailored to its role as a targeted biologic therapy. This approach enables precise, immediate, and consistent treatment for inflammatory conditions, making it a cornerstone of modern medicine. For patients, understanding this distinction highlights why Remicade is administered as an infusion rather than a vaccine and why its production requires advanced biotechnological techniques.
Is Elizabeth Banks in Mockingjay Part 2? Unraveling the Cast Mystery
You may want to see also
Frequently asked questions
No, Remicade (infliximab) is not a protein vaccine. It is a monoclonal antibody, specifically a chimeric IgG1 antibody, designed to target and neutralize tumor necrosis factor alpha (TNF-α), a protein involved in inflammation.
Yes, Remicade is an antibody treatment. It is a biologic therapy that works by binding to TNF-α, thereby reducing inflammation and modulating the immune response in conditions like rheumatoid arthritis, Crohn's disease, and ulcerative colitis.
Yes, Remicade contains proteins, specifically a monoclonal antibody protein. It is a chimeric antibody, meaning it is made from a combination of human and mouse proteins, designed to minimize immune reactions while maintaining effectiveness.