The question of whether the COVID-19 vaccine is a live vaccine is a common one, often arising from concerns about how vaccines work and their potential risks. Unlike live attenuated vaccines, which use a weakened form of the virus to trigger an immune response, most COVID-19 vaccines, such as those developed by Pfizer-BioNTech and Moderna, utilize mRNA technology. These vaccines deliver genetic instructions to cells to produce a harmless piece of the SARS-CoV-2 spike protein, prompting the immune system to recognize and combat the virus without introducing any live virus particles. Other COVID-19 vaccines, like the Johnson & Johnson and AstraZeneca options, use viral vector technology, which employs a modified, non-replicating virus to deliver the spike protein instructions. None of these mechanisms involve live SARS-CoV-2, making them safe for individuals with weakened immune systems and eliminating the risk of causing COVID-19 infection. Understanding these distinctions is crucial for addressing vaccine hesitancy and promoting informed decision-making.
| Characteristics | Values |
|---|---|
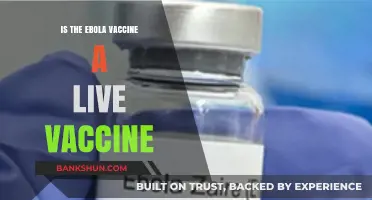
| Vaccine Type | Most COVID-19 vaccines are not live vaccines. They are primarily mRNA, viral vector, or protein subunit vaccines. |
| mRNA Vaccines (e.g., Pfizer-BioNTech, Moderna) | Do not contain live virus; use genetic material to instruct cells to produce a harmless piece of the virus (spike protein) to trigger an immune response. |
| Viral Vector Vaccines (e.g., AstraZeneca, Johnson & Johnson) | Use a modified, non-replicating virus (vector) to deliver genetic material encoding the spike protein; does not contain live SARS-CoV-2 virus. |
| Protein Subunit Vaccines (e.g., Novavax) | Contain harmless pieces of the virus (spike protein) but no live virus. |
| Live Attenuated Vaccines | None of the widely approved COVID-19 vaccines are live attenuated. Some candidates in development (e.g., COVI-VAC) use live attenuated virus, but these are not yet authorized for widespread use. |
| Safety for Immunocompromised | Non-live vaccines (mRNA, viral vector, protein subunit) are considered safe for immunocompromised individuals, unlike live vaccines. |
| Storage Requirements | Varies by type; mRNA vaccines require ultra-cold storage, while others (e.g., AstraZeneca, Novavax) have less stringent requirements. |
| Efficacy | High efficacy against severe disease, hospitalization, and death across all non-live vaccine types. |
| Side Effects | Generally mild to moderate (e.g., pain at injection site, fatigue, fever) and short-lived. |
| Booster Recommendations | Boosters are recommended for all vaccine types to maintain immunity against variants. |
Explore related products






What You'll Learn
- Definition of Live Vaccines: Live vaccines use weakened viruses to trigger immune responses
- COVID-19 Vaccine Types: Most COVID-19 vaccines are mRNA or viral vector, not live
- Pfizer and Moderna: These mRNA vaccines do not contain live coronavirus particles
- Johnson & Johnson: Uses viral vector, not live COVID-19 virus, to deliver instructions
- Safety Concerns: Live vaccines are avoided for immunocompromised; COVID-19 vaccines are safe for them
![]()
Definition of Live Vaccines: Live vaccines use weakened viruses to trigger immune responses
Live vaccines harness the power of weakened viruses to teach the immune system how to fight off future infections. Unlike inactivated or subunit vaccines, which use dead pathogens or fragments, live vaccines introduce a modified, less virulent form of the virus that can still replicate inside the body. This replication mimics a natural infection, prompting a robust immune response without causing the disease itself. The key lies in attenuation—a process that reduces the virus’s ability to cause illness while preserving its immunogenicity. Examples include the measles, mumps, and rubella (MMR) vaccine and the varicella (chickenpox) vaccine, both of which use weakened strains to confer long-lasting immunity.
Attenuation is achieved through various methods, such as serial passage in cell cultures or genetic modification. For instance, the oral polio vaccine (OPV) was developed by repeatedly culturing the poliovirus in non-human cells, gradually weakening its ability to infect humans. This process ensures the virus remains viable but no longer poses a significant health risk. Live vaccines are particularly effective because they stimulate both humoral (antibody-mediated) and cell-mediated immunity, providing a more comprehensive defense. However, their use is not without caution—individuals with compromised immune systems, such as those undergoing chemotherapy or living with HIV, may be at risk of adverse effects if given live vaccines.
Dosage and administration of live vaccines are carefully calibrated to balance safety and efficacy. For example, the MMR vaccine is typically administered in two doses: the first at 12–15 months of age and the second at 4–6 years. This schedule ensures optimal immune response while minimizing the risk of complications. It’s crucial to follow these guidelines, as deviations can reduce effectiveness or increase side effects. Practical tips include avoiding live vaccines during pregnancy and ensuring proper storage, as many live vaccines require refrigeration to maintain viability.
Comparing live vaccines to other types highlights their unique advantages and limitations. While inactivated vaccines, like the injectable polio vaccine (IPV), are safer for immunocompromised individuals, they often require booster shots to maintain immunity. Subunit vaccines, such as the hepatitis B vaccine, are highly targeted but may elicit a weaker immune response. Live vaccines, in contrast, offer durable immunity with fewer doses but carry a small risk of vaccine-associated illness. This trade-off underscores the importance of tailoring vaccine choice to individual health status and epidemiological context.
In the context of COVID-19, understanding live vaccines is crucial for distinguishing them from the vaccines currently in use. The Pfizer-BioNTech and Moderna mRNA vaccines, as well as the Johnson & Johnson viral vector vaccine, are not live vaccines. They do not contain weakened SARS-CoV-2 virus but instead use genetic material or a harmless virus to instruct cells to produce the spike protein, triggering an immune response. This distinction is vital for addressing public concerns and ensuring informed decision-making. While live vaccines remain a cornerstone of preventive medicine, their application in COVID-19 vaccination has not been pursued due to safety and logistical considerations.
US Bank's Future: Will It Survive or Close Down?
You may want to see also
Explore related products

$17.99

$17.99

$17.99



![]()
COVID-19 Vaccine Types: Most COVID-19 vaccines are mRNA or viral vector, not live
The COVID-19 vaccines authorized for use globally fall into distinct categories, with mRNA and viral vector vaccines dominating the landscape. Notably, none of the widely distributed vaccines are live vaccines, which use a weakened form of the virus to trigger immunity. Instead, mRNA vaccines (like Pfizer-BioNTech and Moderna) deliver genetic instructions for cells to produce a harmless spike protein, mimicking the virus and prompting an immune response. Viral vector vaccines (such as AstraZeneca and Johnson & Johnson) use a modified, harmless virus to transport the same genetic material. This distinction is critical for understanding vaccine safety, efficacy, and suitability for specific populations, such as immunocompromised individuals or those with allergies.
For instance, mRNA vaccines require ultra-cold storage (Pfizer at -70°C, Moderna at -20°C) initially, though they can be stored in standard refrigerators for up to 30 days after thawing. They are administered in two doses, typically 3–4 weeks apart, with a 94–95% efficacy rate in preventing severe illness. Viral vector vaccines, on the other hand, are more stable at standard refrigeration temperatures (2–8°C) and often require just a single dose (Johnson & Johnson) or two doses spaced 4–12 weeks apart (AstraZeneca). While slightly less efficacious (67–90% depending on the vaccine), they offer robust protection against hospitalization and death. Understanding these differences helps individuals make informed decisions based on availability, storage logistics, and personal health considerations.
A key advantage of mRNA and viral vector vaccines is their safety profile, particularly for those concerned about live vaccines. Since they do not contain live virus particles, they cannot cause COVID-19 infection, making them suitable for individuals with weakened immune systems or chronic conditions. However, rare side effects, such as myocarditis (inflammation of the heart muscle) in young males after mRNA vaccination or thrombosis with thrombocytopenia syndrome (TTS) after viral vector vaccines, have been reported. These risks are exceedingly low (e.g., TTS occurs in approximately 7 per 1 million doses of Johnson & Johnson) and are outweighed by the vaccines' benefits in preventing severe COVID-19 outcomes.
Comparatively, live vaccines, like the measles or chickenpox vaccines, carry a theoretical risk of causing disease in immunocompromised individuals, which is why they are contraindicated in certain populations. The non-live nature of COVID-19 vaccines eliminates this concern, broadening their applicability. For example, the Pfizer vaccine is approved for individuals aged 5 and older, while Moderna is authorized for those 6 months and older, with adjusted dosages for younger age groups (e.g., 25 micrograms for children under 12, compared to 100 micrograms for adults). This flexibility underscores the adaptability of mRNA and viral vector technologies in addressing diverse public health needs.
In practical terms, knowing whether a vaccine is live or not influences storage, distribution, and administration strategies. For healthcare providers, mRNA vaccines require careful handling due to their temperature sensitivity, while viral vector vaccines offer greater logistical ease. For recipients, understanding the vaccine type can alleviate concerns about safety and efficacy, particularly for those with specific health conditions. For example, pregnant individuals or those planning to conceive may prefer mRNA vaccines, as they have a more extensive safety data profile in these populations. Ultimately, the absence of live vaccines in the COVID-19 arsenal reflects a deliberate choice to prioritize safety, efficacy, and accessibility in the global fight against the pandemic.
Foreign Bank Transfers: Risky or Safe?
You may want to see also
Explore related products






![]()
Pfizer and Moderna: These mRNA vaccines do not contain live coronavirus particles
The Pfizer and Moderna COVID-19 vaccines are groundbreaking in their use of messenger RNA (mRNA) technology, a platform that does not rely on live coronavirus particles. Unlike traditional live-attenuated vaccines, which introduce a weakened form of the virus to trigger an immune response, mRNA vaccines deliver genetic instructions to our cells, teaching them to produce a harmless piece of the SARS-CoV-2 spike protein. This protein prompts the immune system to recognize and combat the virus without exposing the body to the actual pathogen. For instance, the Pfizer vaccine, administered in two 30-microgram doses 21 days apart for individuals aged 12 and older, and the Moderna vaccine, given in two 100-microgram doses 28 days apart for those aged 18 and older, both operate on this principle. This distinction is crucial for understanding why these vaccines cannot cause COVID-19 infection.
From a practical standpoint, the absence of live coronavirus particles in Pfizer and Moderna vaccines eliminates the risk of vaccine-induced illness, making them safer for individuals with compromised immune systems or chronic conditions. For example, immunocompromised patients, who might be at higher risk from live vaccines, can receive mRNA vaccines without fear of contracting the virus. Additionally, the mRNA itself does not enter the cell’s nucleus, ensuring it does not alter human DNA. This fact addresses a common misconception about these vaccines. Parents, in particular, can feel confident administering these vaccines to eligible children, knowing they are designed to stimulate immunity without introducing live virus particles.
Comparatively, mRNA vaccines offer a faster and more adaptable production process than traditional live vaccines, which often require culturing viruses in eggs or cells. This efficiency became evident during the pandemic, as Pfizer and Moderna were able to develop and distribute their vaccines within a year of the virus’s emergence. The technology’s flexibility also allows for rapid updates to target new variants, such as the Omicron-specific boosters. In contrast, live vaccines typically require more time to modify and produce, making them less suited for rapidly evolving pathogens like SARS-CoV-2.
Persuasively, the safety profile of mRNA vaccines is a strong argument for their widespread adoption. Clinical trials and real-world data have consistently shown that side effects, such as fatigue, headache, or fever, are generally mild and short-lived, resolving within a few days. These symptoms are not signs of infection but rather indicators of the immune system’s response to the vaccine. For those hesitant about vaccination, understanding that these vaccines do not contain live coronavirus particles can alleviate concerns about contracting COVID-19 from the shot itself. This clarity is essential for building trust in vaccination efforts.
In conclusion, the Pfizer and Moderna mRNA vaccines represent a paradigm shift in vaccine technology, offering a safe and effective solution without relying on live coronavirus particles. Their design not only minimizes risks but also showcases the potential of mRNA platforms for future vaccines. By focusing on this unique aspect, individuals can make informed decisions about vaccination, contributing to broader public health goals. Whether for personal protection or community immunity, these vaccines stand as a testament to scientific innovation in the fight against COVID-19.
How to Easily Delete Payees on TSB Banking: Step-by-Step Guide
You may want to see also
Explore related products






![]()
Johnson & Johnson: Uses viral vector, not live COVID-19 virus, to deliver instructions
The Johnson & Johnson COVID-19 vaccine stands apart from its mRNA counterparts by employing a viral vector technology. This means it uses a modified, harmless version of a different virus (in this case, an adenovirus) as a delivery system. Think of it like a Trojan horse: the adenovirus acts as the horse, carrying genetic instructions into your cells without causing illness itself. These instructions teach your cells to produce a harmless piece of the COVID-19 virus's spike protein, triggering your immune system to recognize and fight off the real virus if exposed.
Crucially, the Johnson & Johnson vaccine does not contain any live COVID-19 virus. This distinction is vital for individuals with compromised immune systems or those hesitant about live-virus vaccines. The single-dose regimen further simplifies the vaccination process, offering convenience and potentially broader accessibility.
This viral vector approach has been used successfully in other vaccines, such as those for Ebola and Zika. While the Johnson & Johnson vaccine's efficacy rate is slightly lower than mRNA vaccines, it still provides robust protection against severe illness, hospitalization, and death from COVID-19. It's authorized for individuals aged 18 and older, offering a valuable tool in the fight against the pandemic, particularly in regions with limited access to ultra-cold storage required for mRNA vaccines.
Remember, consulting with a healthcare professional is essential to determine the most suitable COVID-19 vaccine for your individual needs and medical history.
South Shore Bank QuickBooks Integration: Seamless Financial Management Explained
You may want to see also
Explore related products






![]()
Safety Concerns: Live vaccines are avoided for immunocompromised; COVID-19 vaccines are safe for them
Live vaccines, such as those for measles, mumps, and rubella (MMR), contain weakened forms of the virus that can replicate in the body. For immunocompromised individuals—those with weakened immune systems due to conditions like HIV, cancer treatments, or organ transplants—these vaccines pose a risk. The attenuated virus, though safe for healthy individuals, can potentially cause infection in those with compromised immunity. This is why live vaccines are generally contraindicated for this population, as the benefits may be outweighed by the risk of adverse effects.
In contrast, COVID-19 vaccines, including mRNA (Pfizer-BioNTech, Moderna) and viral vector (Johnson & Johnson, AstraZeneca) types, do not contain live virus. mRNA vaccines deliver genetic instructions for cells to produce a harmless piece of the SARS-CoV-2 spike protein, triggering an immune response. Viral vector vaccines use a modified, non-replicating virus to deliver the same genetic material. Neither type can cause COVID-19 or replicate in the body, making them safe for immunocompromised individuals. Clinical trials and real-world data have confirmed their safety and efficacy in this population, though the immune response may be less robust due to underlying conditions.
For immunocompromised individuals, COVID-19 vaccination is not only safe but critical. This group is at higher risk for severe COVID-19 outcomes, including hospitalization and death. The CDC recommends additional doses for moderate to severely immunocompromised individuals, such as a third dose of mRNA vaccines 28 days after the second, followed by a booster. For example, a 40-year-old cancer patient on chemotherapy should receive this extended regimen to maximize protection. Practical tips include scheduling vaccinations during periods of optimal immune function, if applicable, and consulting healthcare providers for personalized advice.
Comparatively, the safety profile of COVID-19 vaccines for immunocompromised individuals stands in stark contrast to live vaccines. While live vaccines require avoidance in this group, COVID-19 vaccines are actively encouraged. This distinction highlights the importance of vaccine technology in addressing diverse health needs. For instance, a 65-year-old transplant recipient can safely receive a COVID-19 vaccine without the risk of viral replication, whereas an MMR vaccine would be contraindicated. This tailored approach ensures protection without compromising safety, underscoring the advancements in vaccine development.
In conclusion, the safety of COVID-19 vaccines for immunocompromised individuals is a testament to their non-live nature and innovative design. Unlike live vaccines, which are avoided due to replication risks, COVID-19 vaccines offer a critical layer of protection for this vulnerable population. Adhering to recommended dosing schedules and consulting healthcare providers ensures optimal outcomes. This distinction not only addresses safety concerns but also reinforces the importance of vaccine technology in safeguarding public health across all demographics.
Faze Banks and Alissa Violet: The Story of Their First Encounter
You may want to see also
Frequently asked questions
No, none of the COVID-19 vaccines authorized for use (such as Pfizer-BioNTech, Moderna, Johnson & Johnson, or AstraZeneca) are live vaccines. They do not contain a live virus and cannot cause COVID-19.
COVID-19 vaccines work by introducing a harmless piece of the virus (like the spike protein or its genetic instructions) to your immune system, which then learns to recognize and fight the virus without exposing you to the actual disease.
No, there is no risk of getting COVID-19 from the vaccine because it does not contain the live virus. The vaccines are designed to trigger an immune response safely without causing the disease.