The question of whether the H1N1 vaccine is an mRNA vaccine is a common one, especially given the increased attention on mRNA technology following the COVID-19 pandemic. The H1N1 vaccine, developed to combat the 2009 swine flu pandemic, is not an mRNA vaccine. Instead, it is primarily based on traditional vaccine technologies, such as inactivated virus or recombinant protein methods. mRNA vaccines, like those used for COVID-19, work by delivering genetic material that instructs cells to produce a specific protein, triggering an immune response. In contrast, the H1N1 vaccine relies on introducing a killed or weakened form of the virus or its components to stimulate immunity, highlighting the diversity of approaches in vaccine development.
| Characteristics | Values |
|---|---|
| Vaccine Type | The H1N1 vaccine is not an mRNA vaccine. |
| Technology Used | Primarily inactivated virus or live attenuated virus vaccines. |
| mRNA Technology | mRNA technology was not used in H1N1 vaccines. |
| Development Timeline | H1N1 vaccines were developed using traditional methods in 2009. |
| Storage Requirements | Typically requires refrigeration (2-8°C), not ultra-cold storage. |
| Administration | Given via injection (inactivated) or nasal spray (live attenuated). |
| Efficacy | High efficacy against the H1N1 strain, similar to seasonal flu vaccines. |
| Side Effects | Mild side effects like soreness, fever, or fatigue, similar to other flu vaccines. |
| Availability | Widely available during the 2009 H1N1 pandemic and included in seasonal flu vaccines later. |
| Current Use | H1N1 strain is now included in seasonal flu vaccines, not as a standalone mRNA vaccine. |
Explore related products






What You'll Learn
![]()
H1N1 vaccine technology overview
The H1N1 vaccine, developed in response to the 2009 swine flu pandemic, relies on traditional vaccine technologies rather than mRNA platforms. Unlike the COVID-19 mRNA vaccines, which use genetic material to instruct cells to produce a viral protein, H1N1 vaccines are primarily inactivated or live attenuated vaccines. Inactivated vaccines contain killed viruses incapable of replicating, while live attenuated vaccines use weakened viruses to stimulate immunity. These methods have been cornerstone technologies in vaccinology for decades, offering proven safety and efficacy profiles. For instance, the 2009 H1N1 vaccine was produced using egg-based manufacturing, a well-established process that involves growing the virus in chicken eggs before inactivating it. This approach ensured rapid scalability during the pandemic, with doses typically administered in 0.5 mL for adults and 0.25 mL for children aged 6 months to 3 years.
Analyzing the technology behind the H1N1 vaccine reveals its adaptability to existing infrastructure. The use of inactivated or live attenuated viruses allowed manufacturers to leverage decades of experience with seasonal flu vaccines. This familiarity expedited regulatory approvals and distribution, critical during a global health crisis. However, the technology is not without limitations. Egg-based production can be time-consuming and less flexible compared to newer platforms like mRNA. For example, mutations in the virus during egg adaptation occasionally reduced vaccine effectiveness, as seen in some H3N2 strains. Despite this, the H1N1 vaccine remains a testament to the reliability of traditional methods, with over 80 million doses administered in the U.S. alone during the pandemic.
A key takeaway for individuals considering the H1N1 vaccine is its safety and accessibility. The vaccine is approved for individuals aged 6 months and older, with specific formulations tailored to age groups. For children under 9, two doses administered four weeks apart are recommended if it’s their first flu vaccination. Adults and older children typically require a single dose. Practical tips include scheduling vaccination early in the flu season and monitoring for mild side effects, such as soreness at the injection site or low-grade fever. Unlike mRNA vaccines, which require ultra-cold storage, H1N1 vaccines are stable at standard refrigeration temperatures, simplifying distribution in resource-limited settings.
Comparing the H1N1 vaccine to mRNA technologies highlights the evolution of vaccinology. While mRNA vaccines offer rapid development and high efficacy, as seen with COVID-19, traditional methods remain indispensable for widespread immunization campaigns. The H1N1 vaccine’s success underscores the importance of diversifying vaccine platforms to address different public health challenges. For instance, mRNA vaccines excel in targeting rapidly mutating viruses, but traditional vaccines provide a robust, cost-effective solution for well-characterized pathogens like influenza. This duality ensures global health systems can respond effectively to both emerging and established threats.
In conclusion, the H1N1 vaccine’s technology exemplifies the strength of traditional vaccinology in managing global pandemics. Its reliance on inactivated or live attenuated viruses, coupled with established manufacturing processes, enabled rapid deployment during the 2009 crisis. While newer platforms like mRNA offer innovative solutions, the H1N1 vaccine remains a vital tool in the fight against influenza. Understanding its technology not only highlights its historical significance but also informs future vaccine development strategies, ensuring a balanced approach to global health preparedness.
How Long Do Australian Banks Retain Financial Records?
You may want to see also
Explore related products

$27.74 $32.99





![]()
Difference between mRNA and H1N1 vaccines
The H1N1 vaccine, developed to combat the 2009 swine flu pandemic, is not an mRNA vaccine. Instead, it relies on traditional vaccine technology, primarily using inactivated or attenuated forms of the virus. This fundamental difference in design distinguishes it from mRNA vaccines, such as those used for COVID-19, which deliver genetic instructions to cells to produce a viral protein, triggering an immune response. Understanding this distinction is crucial for appreciating the evolution of vaccine technology and its implications for public health.
From a technological standpoint, mRNA vaccines represent a leap forward in vaccine development. They encode for a specific viral protein, typically the spike protein, which the immune system recognizes as foreign. For instance, the Pfizer-BioNTech and Moderna COVID-19 vaccines use mRNA to instruct cells to produce the SARS-CoV-2 spike protein. In contrast, the H1N1 vaccine contains either inactivated virus particles or weakened live viruses, directly exposing the immune system to the pathogen in a non-infectious form. This traditional approach has been used for decades in vaccines like the seasonal flu shot, which often includes H1N1 strains as part of its formulation.
The manufacturing process further highlights the differences between these vaccines. mRNA vaccines can be produced rapidly because they rely on synthesizing genetic material, a process that can be scaled up quickly. This was evident during the COVID-19 pandemic, where mRNA vaccines were developed and deployed within a year. Conversely, the H1N1 vaccine requires growing the virus in eggs or cell cultures, a time-consuming process that limits production speed. For example, during the 2009 H1N1 pandemic, vaccine distribution was delayed due to these manufacturing constraints, affecting global immunization efforts.
Efficacy and administration also vary between the two types. mRNA vaccines typically require two doses, spaced 3–4 weeks apart, to achieve optimal immunity. For instance, the COVID-19 mRNA vaccines have shown efficacy rates of around 95% after the second dose. The H1N1 vaccine, on the other hand, often requires a single dose for adults, though young children may need two doses spaced 4 weeks apart. Its efficacy varies but generally provides robust protection against severe illness. Additionally, mRNA vaccines are stored at ultra-cold temperatures (e.g., -70°C for Pfizer), whereas H1N1 vaccines are stable at standard refrigerator temperatures (2–8°C), making them easier to distribute in resource-limited settings.
Practically, these differences influence how vaccines are deployed during outbreaks. mRNA technology’s speed and adaptability make it ideal for responding to novel pathogens, as seen with COVID-19. However, its storage requirements can pose challenges in low-income regions. The H1N1 vaccine, with its established production methods and simpler storage needs, remains a reliable option for seasonal flu campaigns. For individuals, understanding these distinctions can help demystify vaccine types and build trust in immunization programs. For example, knowing that the H1N1 vaccine uses a proven method may reassure those hesitant about newer technologies like mRNA.
In summary, while both mRNA and H1N1 vaccines aim to prevent viral infections, their mechanisms, production, and logistics differ significantly. mRNA vaccines represent cutting-edge innovation, offering rapid development and high efficacy, while H1N1 vaccines rely on time-tested methods, providing accessibility and ease of distribution. Both play vital roles in global health, tailored to the specific demands of the diseases they target.
Understanding Fractional Reserve Banking: A Step-by-Step Formula Calculation Guide
You may want to see also
Explore related products

$118.88 $159





![]()
H1N1 vaccine composition details
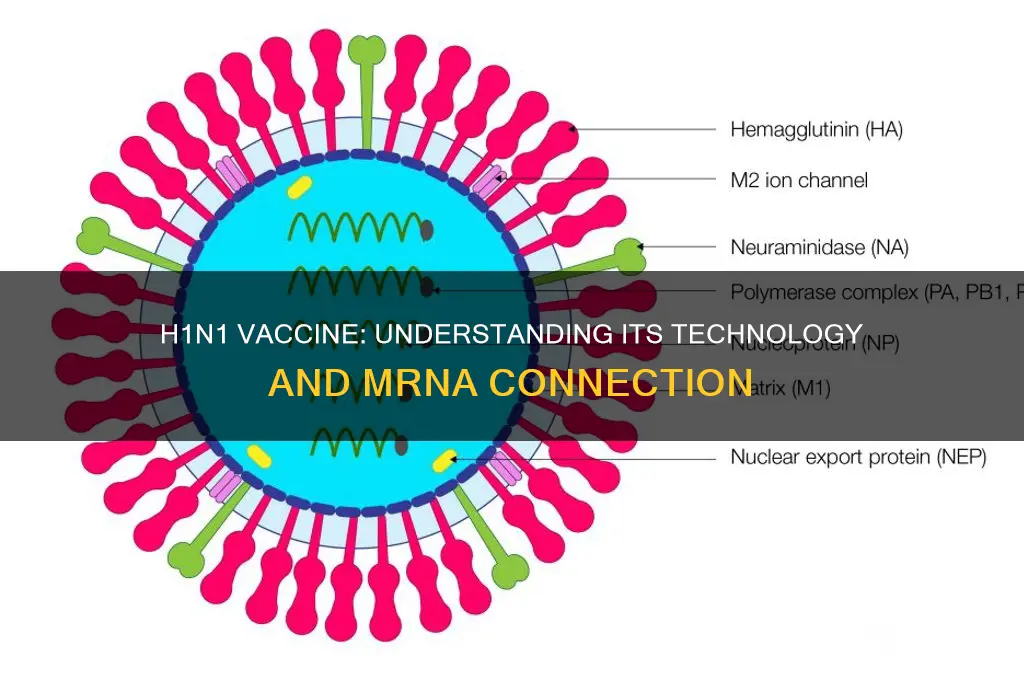
The H1N1 vaccine, developed in response to the 2009 swine flu pandemic, is not an mRNA vaccine. Instead, it primarily utilizes traditional vaccine technologies, such as inactivated virus or recombinant protein-based approaches. Understanding its composition is crucial for distinguishing it from newer mRNA platforms like those used for COVID-19 vaccines. The H1N1 vaccine contains hemagglutinin (HA), a surface protein of the influenza virus, which triggers an immune response. This HA antigen is derived from the specific strain of the H1N1 virus responsible for the outbreak, ensuring targeted protection.
Analyzing the composition further, the H1N1 vaccine often includes adjuvants like aluminum salts to enhance immune response, particularly in doses for younger children or immunocompromised individuals. For example, the 2009 pandemic vaccine for children aged 6 months to 9 years typically required two 0.25 mL doses, spaced 21 days apart, while adults received a single 0.5 mL dose. This dosing strategy highlights the vaccine’s adaptability to different age groups and immune needs. Unlike mRNA vaccines, which deliver genetic material to prompt protein production, the H1N1 vaccine directly introduces the antigen, relying on established vaccine mechanisms.
A comparative perspective reveals that while mRNA vaccines offer rapid development and high efficacy, the H1N1 vaccine’s composition prioritizes stability and familiarity. Its inactivated virus or subunit formulations have been used for decades in seasonal flu vaccines, providing a proven safety profile. This makes it a reliable choice for mass immunization campaigns, especially during urgent public health crises. However, its production timeline is longer compared to mRNA vaccines, as it requires culturing the virus in eggs or cell lines, a process that can take months.
For practical application, individuals receiving the H1N1 vaccine should be aware of potential side effects, such as soreness at the injection site, mild fever, or fatigue, which typically resolve within a few days. Pregnant women and those with severe egg allergies should consult healthcare providers, as some formulations are egg-based. The vaccine’s composition ensures broad accessibility, with options like thimerosal-free versions available for specific populations. This tailored approach underscores its role as a cornerstone of influenza prevention, distinct from the innovative but newer mRNA technology.
In conclusion, the H1N1 vaccine’s composition reflects a blend of tradition and precision, designed to combat a specific viral threat using well-established methods. Its reliance on inactivated virus or recombinant proteins, coupled with adjuvants and age-specific dosing, sets it apart from mRNA vaccines. This distinction is vital for public health education, ensuring clarity about the tools available for different infectious diseases. By understanding its unique makeup, individuals can make informed decisions about vaccination, appreciating both its historical significance and ongoing relevance.
Financial Counselling: Banks' Obligation or Opportunity?
You may want to see also
Explore related products






![]()
mRNA vaccines vs. traditional vaccines
The H1N1 vaccine, developed in response to the 2009 swine flu pandemic, is not an mRNA vaccine. Instead, it falls into the category of traditional vaccines, specifically an inactivated influenza vaccine. This distinction highlights the fundamental differences between mRNA technology and conventional vaccination methods, which have been pivotal in shaping global health responses to infectious diseases.
A Tale of Two Technologies: Traditional vaccines, like the H1N1 shot, typically contain inactivated or weakened forms of the virus, stimulating the immune system to recognize and combat the pathogen. These vaccines have been the cornerstone of immunization for decades, with well-established production processes and safety profiles. For instance, the seasonal flu vaccine, often administered annually, employs this approach, offering protection against multiple influenza strains. In contrast, mRNA vaccines represent a revolutionary shift. They deliver genetic material (mRNA) encoding a viral protein, prompting our cells to produce it, thereby triggering an immune response. This method, as seen in the Pfizer-BioNTech and Moderna COVID-19 vaccines, offers unprecedented speed and flexibility in vaccine development.
Speed and Adaptability: One of the most significant advantages of mRNA vaccines is their rapid development timeline. Traditional vaccines often require years of research and production, as seen in the case of the H1N1 vaccine, which was developed and distributed within months of the outbreak. mRNA technology, however, allows for a more agile response. Once the genetic sequence of a virus is known, mRNA vaccines can be designed and produced in a matter of weeks, as demonstrated during the COVID-19 pandemic. This speed is crucial in addressing emerging infectious diseases and potential pandemic threats.
Efficacy and Safety: Both vaccine types have proven effective, but their mechanisms differ. Traditional vaccines often require adjuvants to enhance the immune response, while mRNA vaccines inherently stimulate a robust reaction. mRNA vaccines have shown impressive efficacy rates, with some studies reporting over 90% effectiveness against symptomatic COVID-19. However, traditional vaccines remain essential, especially for certain populations. For example, the H1N1 vaccine was recommended for individuals aged 6 months and older, including pregnant women and those with underlying medical conditions, ensuring broad protection during the pandemic.
Storage and Distribution: The logistical aspects of vaccine distribution also differ significantly. Traditional vaccines often require refrigeration, but not freezing, making them more accessible for global distribution. mRNA vaccines, on the other hand, typically need ultra-cold storage, presenting challenges for transportation and storage, especially in low-resource settings. This has led to innovative solutions, such as the development of more stable mRNA vaccine formulations and specialized storage equipment.
In the ongoing battle against infectious diseases, both mRNA and traditional vaccines play critical roles. While the H1N1 vaccine is not an mRNA product, the comparison highlights the evolution of vaccine technology, offering a glimpse into the future of immunization strategies. Understanding these differences is essential for healthcare professionals and the public alike, ensuring informed decisions and effective public health measures.
Mesa Verde Bank's Role in Breaking Bad: Fact or Fiction?
You may want to see also
Explore related products






![]()
H1N1 vaccine development process
The H1N1 vaccine, developed in response to the 2009 swine flu pandemic, is not an mRNA vaccine. Instead, it relies on traditional vaccine technologies, primarily using inactivated virus particles or recombinant proteins. Understanding its development process sheds light on how rapidly scientists can mobilize to combat emerging infectious diseases, a framework that later informed the COVID-19 vaccine response.
Step 1: Strain Identification and Isolation
The process began with isolating the H1N1 virus from infected individuals. Once identified, the virus strain was sequenced and shared globally through the World Health Organization (WHO). This step was critical, as the specific genetic makeup of the virus determined the vaccine’s effectiveness. For instance, the 2009 H1N1 strain was a novel reassortment of swine, avian, and human flu viruses, requiring urgent attention to prevent widespread transmission.
Step 2: Vaccine Production Methods
Unlike mRNA vaccines, which use genetic material to instruct cells to produce a viral protein, the H1N1 vaccine employed two primary methods: egg-based production and cell-based production. Egg-based vaccines involved injecting the virus into fertilized chicken eggs, allowing it to replicate, and then inactivating it for use in the vaccine. Cell-based vaccines used animal cell cultures, offering a faster and more scalable alternative. Both methods produced inactivated virus particles, which were then purified and formulated into doses. A typical adult dose contained 15 micrograms of hemagglutinin antigen, the key component triggering an immune response.
Step 3: Clinical Trials and Approval
Accelerated clinical trials ensured the vaccine’s safety and efficacy. Phase I and II trials assessed dosage and immune response in healthy adults and children, while Phase III trials expanded to larger populations. Results showed that a single dose provided sufficient immunity for adults, while children under 10 required two doses, spaced three weeks apart. Regulatory agencies like the FDA granted emergency use authorization within months, a testament to the urgency and global collaboration during the pandemic.
Cautions and Considerations
While the H1N1 vaccine was safe for most, rare side effects like allergic reactions and Guillain-Barré syndrome were monitored. Pregnant women, healthcare workers, and individuals with chronic conditions were prioritized due to their higher risk of severe illness. Practical tips included avoiding the vaccine if allergic to eggs (for egg-based versions) and staying hydrated post-vaccination to minimize mild side effects like soreness or fever.
Legacy and Takeaway
The H1N1 vaccine development process demonstrated the adaptability of traditional vaccine technologies in crisis situations. Its success laid the groundwork for future pandemic responses, highlighting the importance of global collaboration, rapid regulatory pathways, and public trust in vaccination campaigns. While mRNA technology has since revolutionized vaccine development, the H1N1 effort remains a pivotal example of how established methods can save lives when time is of the essence.
Which Banks Are Accepting PPP Forgiveness Applications?
You may want to see also
Frequently asked questions
No, the H1N1 vaccine is not an mRNA vaccine. It is primarily an inactivated or live attenuated vaccine, depending on the formulation.
The H1N1 vaccine uses traditional vaccine technologies, such as inactivated viruses or live attenuated viruses, not mRNA technology.
No, mRNA vaccines like those developed for COVID-19 are not used for H1N1. H1N1 vaccines rely on older, established methods of vaccine production.