The question of whether the measles vaccine is included in the tetanus vaccine is a common misconception. The measles vaccine is typically administered as part of the MMR (Measles, Mumps, and Rubella) vaccine or the MMRV (Measles, Mumps, Rubella, and Varicella) vaccine, which are specifically designed to protect against these viral infections. On the other hand, the tetanus vaccine, often given as part of the Tdap (Tetanus, Diphtheria, and Pertussis) or DTaP (Diphtheria, Tetanus, and Pertussis) vaccines, targets bacterial infections and does not include protection against measles. These vaccines serve distinct purposes and are administered separately based on recommended immunization schedules to ensure comprehensive protection against different diseases.
Explore related products






What You'll Learn
- Vaccine Types: Measles and tetanus vaccines are separate, targeting different diseases
- Vaccine Schedules: Measles vaccine is part of MMR; tetanus is in DTaP/Tdap
- Ingredients Comparison: Measles vaccine contains weakened virus; tetanus has toxoid
- Disease Prevention: Measles vaccine prevents measles; tetanus vaccine prevents lockjaw
- Common Misconceptions: Combining measles and tetanus vaccines is not standard practice
![]()
Vaccine Types: Measles and tetanus vaccines are separate, targeting different diseases
Measles and tetanus vaccines are distinct entities, each designed to combat specific diseases with unique mechanisms. The measles vaccine, typically administered as part of the MMR (Measles, Mumps, Rubella) vaccine, contains weakened strains of the measles virus. This live-attenuated vaccine stimulates the immune system to produce antibodies, offering long-term protection. In contrast, the tetanus vaccine, often combined with diphtheria and pertussis (DTaP or Tdap), contains inactivated toxins (toxoids) from the tetanus bacterium. These toxoids teach the immune system to recognize and neutralize the harmful effects of tetanus without exposing the body to the disease itself. Understanding this fundamental difference is crucial for appreciating why these vaccines are not interchangeable.
From a practical standpoint, the administration of these vaccines differs significantly. The MMR vaccine is usually given in two doses: the first at 12–15 months of age and the second at 4–6 years. This schedule ensures robust immunity against measles, a highly contagious viral infection. Tetanus vaccination, on the other hand, follows a different timeline. The initial DTaP series is administered in five doses starting at 2 months of age, with boosters recommended every 10 years thereafter. For adolescents and adults, the Tdap vaccine is used as a booster, providing continued protection against tetanus, diphtheria, and pertussis. These distinct schedules highlight the separate roles of each vaccine in disease prevention.
A common misconception is that vaccines can be combined arbitrarily, but this is not the case with measles and tetanus vaccines. Their formulations and purposes are incompatible. Measles vaccines rely on live viruses to trigger immunity, while tetanus vaccines use inactivated components. Combining them into a single shot would not only be ineffective but could also compromise the immune response to one or both diseases. This separation ensures that each vaccine can perform its intended function without interference, maximizing protection against measles and tetanus individually.
For parents and caregivers, knowing the differences between these vaccines is essential for informed decision-making. Measles vaccines are critical in preventing outbreaks of a highly contagious disease that can lead to severe complications, including pneumonia and encephalitis. Tetanus vaccines, meanwhile, protect against a bacterial infection that enters the body through wounds and can cause painful muscle stiffness and life-threatening complications. By adhering to the recommended vaccination schedules for each, individuals can safeguard themselves and their communities from these distinct but equally dangerous diseases.
In summary, measles and tetanus vaccines are separate tools in the public health arsenal, each tailored to combat a specific threat. Their differences in composition, administration, and purpose underscore the importance of treating them as distinct interventions. Whether you’re a healthcare provider, parent, or individual seeking vaccination, recognizing these distinctions ensures that you receive the appropriate protection against measles and tetanus, contributing to broader disease prevention efforts.
Mastering Hit the Bank: Proven Strategies to Win Every Time
You may want to see also
Explore related products






![]()
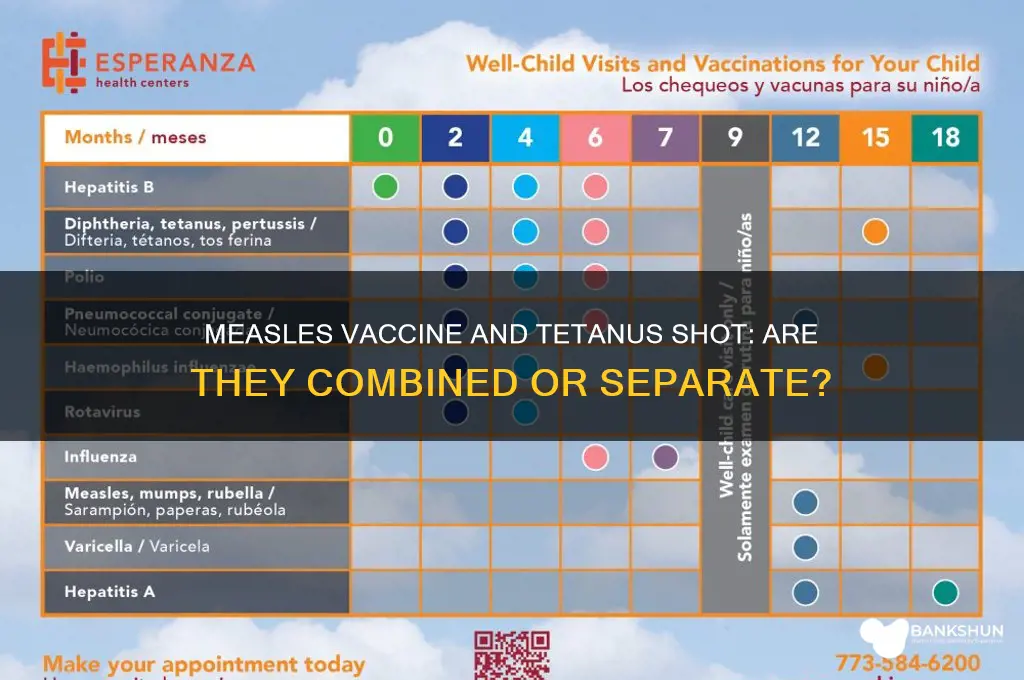
Vaccine Schedules: Measles vaccine is part of MMR; tetanus is in DTaP/Tdap
The measles vaccine is not included in the tetanus vaccine; they are separate components of different combination vaccines. Measles is part of the MMR (Measles, Mumps, Rubella) vaccine, typically administered in two doses: the first at 12–15 months and the second at 4–6 years. Tetanus, on the other hand, is included in the DTaP (Diphtheria, Tetanus, Pertussis) vaccine for children under 7, given in a series of five shots starting at 2 months. For older children and adults, Tdap (Tetanus, Diphtheria, Pertussis) is used as a booster, with the first dose recommended at age 11–12 and subsequent boosters every 10 years. Understanding these schedules ensures proper protection against distinct but equally serious diseases.
From an analytical perspective, the separation of measles and tetanus vaccines into different combinations reflects their unique disease profiles and immunological requirements. Measles, a highly contagious viral infection, demands a live attenuated vaccine, which is incompatible with the inactivated tetanus toxoid. Combining them would risk reducing efficacy or safety. This strategic division also allows for targeted administration based on age and risk factors. For instance, the MMR vaccine aligns with childhood immunization timelines, while Tdap addresses the waning immunity to tetanus and pertussis in adolescents and adults. Such tailored approaches maximize protection while minimizing logistical complexity.
For parents and caregivers, navigating vaccine schedules can feel overwhelming, but a few practical tips simplify the process. First, keep a detailed record of all vaccinations, noting dates and types (e.g., MMR, DTaP). Second, adhere to the CDC’s recommended timeline, but don’t panic if doses are slightly delayed—healthcare providers can adjust schedules as needed. Third, use well-child visits as opportunities to confirm immunization status and address concerns. Finally, stay informed about school or travel requirements, as some regions mandate specific vaccines like MMR for enrollment. Proactive planning ensures timely protection without unnecessary stress.
Comparatively, the MMR and DTaP/Tdap vaccines highlight the evolution of immunization strategies. While both are combination vaccines, their components address distinct disease threats. MMR’s focus on viral infections contrasts with DTaP/Tdap’s targeting of bacterial toxins. This distinction underscores the importance of comprehensive vaccine development, which considers pathogen type, transmission routes, and population vulnerabilities. For example, measles’ airborne spread necessitates high community immunity, achieved through widespread MMR vaccination. Tetanus, acquired through wound exposure, relies on individual immunity via Tdap boosters. These differences exemplify the precision of modern vaccine science.
In conclusion, the measles vaccine and tetanus vaccine are not interchangeable but are integral parts of separate combination vaccines tailored to specific health needs. MMR protects against measles, mumps, and rubella, while DTaP and Tdap safeguard against diphtheria, tetanus, and pertussis. Adhering to recommended schedules ensures lifelong immunity and reduces disease burden. By understanding these distinctions, individuals can make informed decisions, contributing to both personal and public health. Clarity on vaccine components and schedules is essential for dispelling misconceptions and fostering trust in immunization programs.
Is Your Banker Address the Same as Your Street Address?
You may want to see also
Explore related products


$21.85 $22




![]()
Ingredients Comparison: Measles vaccine contains weakened virus; tetanus has toxoid
The measles vaccine and the tetanus vaccine are both essential tools in preventing serious diseases, but their mechanisms of action differ fundamentally due to the nature of the pathogens they target. The measles vaccine contains a live, attenuated (weakened) virus, which stimulates the immune system to recognize and combat the virus without causing the disease. This approach is common in vaccines for viral infections, as it mimics a natural infection and provides long-lasting immunity. For instance, the measles, mumps, and rubella (MMR) vaccine typically contains less than 0.5 mL of weakened measles virus, administered subcutaneously to children aged 12–15 months, with a booster at 4–6 years.
In contrast, the tetanus vaccine relies on a toxoid—a chemically inactivated form of the toxin produced by the *Clostridium tetani* bacterium. Tetanus is caused by a bacterial toxin, not the bacterium itself, so the vaccine targets this toxin rather than the organism. The toxoid is purified and often combined with adjuvants to enhance the immune response. A standard dose of the tetanus toxoid (e.g., in the Tdap vaccine) is 0.5 mL, administered intramuscularly, with boosters recommended every 10 years for adults. This method ensures the body produces antibodies specifically against the toxin, neutralizing its harmful effects.
Comparing these ingredients highlights their tailored design. The weakened virus in the measles vaccine triggers a robust cellular and humoral immune response, preparing the body to fight off the actual virus. The tetanus toxoid, however, focuses on neutralizing the toxin’s activity, preventing it from causing muscle stiffness, spasms, and potentially fatal complications. This distinction underscores why combination vaccines like MMR do not include tetanus—their protective mechanisms are fundamentally different and address distinct biological threats.
For practical application, understanding these differences can guide vaccination decisions. Parents should ensure their children receive the MMR vaccine on schedule to prevent measles, a highly contagious viral disease. Similarly, individuals should stay up-to-date with tetanus boosters, especially after injuries that expose them to soil or rust, where *C. tetani* thrives. While the vaccines are not interchangeable, their unique ingredients work synergistically within public health strategies to prevent outbreaks and protect communities. Always consult healthcare providers for personalized vaccination plans, considering factors like age, health status, and exposure risks.
Mortgages for Mobile Homes: What Banks Offer?
You may want to see also
Explore related products



$17.54 $30



![]()
Disease Prevention: Measles vaccine prevents measles; tetanus vaccine prevents lockjaw
The measles vaccine and the tetanus vaccine are distinct immunizations designed to prevent specific, severe diseases. Each targets a unique pathogen and elicits a tailored immune response, underscoring the precision of modern vaccinology. The measles vaccine, typically administered as part of the MMR (Measles, Mumps, Rubella) shot, contains weakened measles viruses that stimulate the body to produce antibodies without causing illness. It is recommended for children in two doses: the first at 12–15 months and the second at 4–6 years. Adults without immunity should also receive at least one dose, especially before international travel to regions with measles outbreaks. In contrast, the tetanus vaccine, often combined with diphtheria and pertussis (DTaP or Tdap), protects against *Clostridium tetani*, a bacterium that causes lockjaw by producing a potent neurotoxin. Tetanus vaccination follows a different schedule: infants receive a series of DTaP shots starting at 2 months, followed by boosters every 10 years or after deep puncture wounds. These vaccines are not interchangeable; their formulations and purposes are entirely separate, ensuring targeted protection against their respective diseases.
Consider the practical implications of these vaccines in daily life. A child playing in a park steps on a rusty nail, a common scenario that could lead to tetanus if the wound is deep and the individual is unvaccinated. Prompt cleaning of the wound and a tetanus booster, if needed, can prevent the disease. Conversely, during a measles outbreak, unvaccinated individuals are at high risk of contracting the virus, which spreads through respiratory droplets. The measles vaccine’s effectiveness is evident in its ability to reduce infection rates by 97% after two doses, making it a cornerstone of public health. Parents should adhere to the recommended vaccination schedules to ensure their children are protected from both diseases. For travelers, verifying vaccination status is crucial, as some countries require proof of measles immunity or tetanus vaccination before entry, particularly for regions with low vaccination coverage or high disease prevalence.
A comparative analysis highlights the differences in vaccine composition and administration. The measles vaccine is a live-attenuated virus, meaning it contains a weakened form of the pathogen, whereas the tetanus vaccine uses inactivated toxins (toxoids) to trigger immunity. This distinction affects storage and handling: the measles vaccine requires refrigeration to maintain viability, while the tetanus vaccine is more stable. Side effects also vary; the measles vaccine may cause mild fever or rash in some recipients, whereas the tetanus vaccine can lead to soreness at the injection site or low-grade fever. Despite these differences, both vaccines are safe and highly effective, with minimal risk of serious adverse reactions. Understanding these nuances helps healthcare providers educate patients and dispel misconceptions, such as the erroneous belief that the measles vaccine is included in the tetanus shot.
Persuasively, the impact of these vaccines on global health cannot be overstated. Measles vaccination has reduced global deaths by 73% since 2000, saving over 25 million lives, according to the WHO. Tetanus vaccination has nearly eliminated maternal and neonatal tetanus in many countries, a testament to its success. Yet, challenges remain. Vaccine hesitancy and access disparities threaten these achievements, particularly in low-income regions. Advocacy for vaccination must emphasize its dual role: protecting individuals and contributing to herd immunity, which shields vulnerable populations like infants and immunocompromised individuals. By framing vaccination as both a personal and communal responsibility, societies can sustain progress in disease prevention. Practical tips include using vaccination reminder apps, keeping immunization records updated, and consulting healthcare providers to address concerns or catch up on missed doses. In the battle against measles and tetanus, knowledge and action are the most potent tools.
Contacting Sterling Bank Customer Care: A Quick and Easy Guide
You may want to see also
Explore related products






![]()
Common Misconceptions: Combining measles and tetanus vaccines is not standard practice
A common misconception circulating online is that the measles vaccine is included in the tetanus vaccine. This confusion likely stems from the fact that both vaccines are often administered during childhood, but they are entirely separate formulations. The measles vaccine, typically given as part of the MMR (measles, mumps, rubella) or MMRV (measles, mumps, rubella, varicella) vaccine, is a live attenuated virus vaccine. In contrast, the tetanus vaccine, often combined with diphtheria and pertussis (DTaP or Tdap), contains inactivated toxins (toxoids) to stimulate immunity. These vaccines target different pathogens and use distinct mechanisms to confer protection, making their combination neither practical nor standard in immunization schedules.
To clarify, the measles vaccine is recommended for children in two doses: the first at 12–15 months and the second at 4–6 years. The tetanus vaccine, on the other hand, is administered in a series starting at 2 months, with booster shots required every 10 years throughout life. These schedules are designed to maximize efficacy and safety, ensuring that each vaccine’s protection is optimized for its specific target. Combining these vaccines into a single shot would not only complicate manufacturing but also risk reducing their individual effectiveness due to potential interference between components.
From a practical standpoint, parents and caregivers should adhere to the recommended immunization schedules provided by health authorities like the CDC or WHO. For instance, if a child sustains a deep wound and requires a tetanus booster, this does not replace or include protection against measles. Similarly, receiving the MMR vaccine does not confer immunity to tetanus. Understanding these distinctions is crucial to avoid gaps in protection and ensure comprehensive immunity against both vaccine-preventable diseases.
A comparative analysis highlights why combining these vaccines is not standard practice. Measles, a highly contagious viral infection, requires a live vaccine to stimulate a robust immune response. Tetanus, caused by a bacterial toxin, relies on toxoids to neutralize the toxin’s effects. Merging these formulations would necessitate extensive research to ensure safety, stability, and efficacy, which has not been pursued due to the success of current separate vaccines. Additionally, the logistical challenges of storing and administering a combined vaccine would outweigh the minimal convenience of a single shot.
In conclusion, while the measles and tetanus vaccines are both critical components of preventive healthcare, they are distinct in composition, administration, and purpose. Misconceptions about their combination can lead to confusion and potentially delay necessary immunizations. By understanding their differences and following established guidelines, individuals can ensure they receive the appropriate vaccines at the right times, safeguarding themselves and their communities against these preventable diseases.
DIY Postal Lockbox Bank: Securely Store Cash and Valuables at Home
You may want to see also
Frequently asked questions
No, the measles vaccine is not included in the tetanus vaccine. They are separate vaccines designed to protect against different diseases.
Yes, the measles vaccine and tetanus vaccine can be administered at the same time, but they are typically given as part of different vaccination schedules or combinations.
No, there is no single vaccine that combines measles and tetanus protection. Measles is usually part of the MMR (Measles, Mumps, Rubella) vaccine, while tetanus is included in vaccines like DTaP (Diphtheria, Tetanus, Pertussis) or Tdap.