The polio vaccine has been a cornerstone in the global effort to eradicate poliomyelitis, a highly contagious viral disease that can lead to paralysis or death. There are two primary types of polio vaccines: the oral polio vaccine (OPV) and the inactivated polio vaccine (IPV), which is administered via injection. The OPV, developed by Albert Sabin, contains a live but weakened form of the poliovirus and is delivered orally, often in the form of drops. In contrast, the IPV, developed by Jonas Salk, uses a killed poliovirus and is given as an injection, typically in the arm or leg. The choice between the two vaccines depends on factors such as regional polio prevalence, healthcare infrastructure, and individual health considerations, making it essential to understand their differences and applications in the fight against polio.
| Characteristics | Values |
|---|---|
| Type of Vaccine | Both oral (OPV) and injectable (IPV) forms are available. |
| Oral Polio Vaccine (OPV) | Live attenuated virus; administered orally (drops or liquid); induces mucosal immunity; can provide intestinal immunity to prevent viral shedding. |
| Inactivated Polio Vaccine (IPV) | Killed virus; administered via injection (intramuscular or subcutaneous); does not induce mucosal immunity but provides systemic immunity. |
| Efficacy | OPV: Highly effective in preventing paralytic polio and viral shedding; IPV: Highly effective in preventing paralytic polio but does not prevent viral shedding. |
| Dose Schedule | OPV: Multiple doses (usually 3-4) starting at 6 weeks of age; IPV: 3-4 doses starting at 2 months of age, depending on the country. |
| Side Effects | OPV: Rarely, vaccine-associated paralytic polio (VAPP); IPV: Mild pain, redness, or swelling at the injection site. |
| Global Usage | OPV: Primarily used in polio-endemic regions for eradication efforts; IPV: Used in polio-free countries or as part of combination vaccines. |
| Storage | OPV: Requires refrigeration (2-8°C); IPV: Also requires refrigeration (2-8°C). |
| Cost | OPV: Generally less expensive; IPV: More expensive due to production complexity. |
| Latest Data (as of 2023) | Global polio cases have decreased by over 99% since 1988, with both OPV and IPV playing critical roles in eradication efforts. |
Explore related products






What You'll Learn
![]()
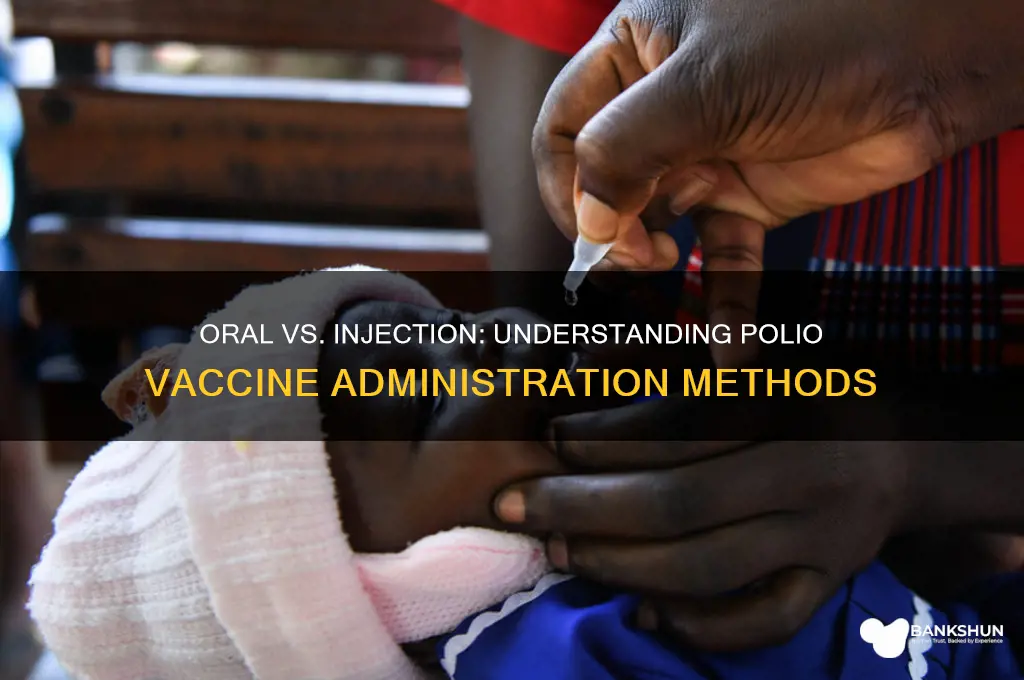
Oral Polio Vaccine (OPV) Types
The Oral Polio Vaccine (OPV) is a cornerstone of global polio eradication efforts, administered as drops rather than an injection. Unlike the inactivated polio vaccine (IPV), which is injected, OPV contains live, attenuated (weakened) strains of the poliovirus. This unique characteristic allows OPV to induce both humoral (bloodstream) and mucosal (intestinal) immunity, making it highly effective in preventing the spread of the virus in communities. However, not all OPVs are created equal. There are three primary types of OPV, each targeting specific strains of the poliovirus, and understanding their differences is crucial for effective immunization strategies.
The trivalent OPV (tOPV), once the workhorse of polio vaccination campaigns, contains all three types of poliovirus (1, 2, and 3). It was widely used until 2016, when the World Health Organization (WHO) recommended a global switch from tOPV to bivalent OPV (bOPV). This shift was driven by the eradication of wild poliovirus type 2 in 1999, making the type 2 component in tOPV unnecessary and potentially risky due to rare cases of vaccine-derived poliovirus (VDPV). Bivalent OPV targets only types 1 and 3, reducing the risk of type 2 VDPV while maintaining protection against the remaining wild types. The transition required meticulous planning, including a synchronized global switch and the introduction of at least one dose of IPV to maintain immunity to type 2.
In addition to tOPV and bOPV, monovalent OPVs (mOPVs) are used in outbreak response. These vaccines target a single poliovirus type, either 1, 2, or 3, and are deployed in areas experiencing outbreaks of vaccine-derived or wild poliovirus. For example, mOPV type 2 has been used to combat type 2 VDPV outbreaks, while mOPV types 1 and 3 are reserved for regions where wild poliovirus persists. The strategic use of mOPVs allows for a targeted response, minimizing the risk of further spread while avoiding unnecessary exposure to other vaccine strains.
Administering OPV requires precision, especially in resource-limited settings. The vaccine is given orally, typically in two drops for each dose, and is most effective when administered to children under five years old. Multiple doses are necessary to build robust immunity, with the WHO recommending at least three doses in routine immunization schedules. In outbreak settings, supplementary immunization activities (SIAs) may involve additional rounds of vaccination to ensure high coverage. Parents and caregivers should ensure children receive all scheduled doses, as partial immunization leaves them vulnerable to infection.
While OPV has been instrumental in reducing polio cases by over 99% since 1988, it is not without limitations. The live attenuated virus in OPV can, in rare instances, revert to a virulent form, causing VDPV. This risk underscores the importance of transitioning to IPV in the endgame of polio eradication. However, in regions where polio remains endemic or outbreaks occur, OPV remains the most effective tool for interrupting transmission. Its ease of administration, low cost, and ability to induce mucosal immunity make it indispensable in the fight against polio. Understanding the types of OPV and their appropriate use is essential for health workers, policymakers, and communities alike to ensure a polio-free future.
Mastering Customer Delight: Strategies for Banking Excellence and Loyalty
You may want to see also
Explore related products






![]()
Inactivated Polio Vaccine (IPV) Administration
The inactivated polio vaccine (IPV) is administered via injection, typically into the muscle (intramuscularly) or just under the skin (subcutaneously), depending on the recipient’s age and the healthcare provider’s protocol. Unlike the oral polio vaccine (OPV), which uses a weakened live virus, IPV contains inactivated (killed) poliovirus, making it incapable of causing polio but highly effective in triggering a strong immune response. This method of delivery ensures safety, particularly for individuals with weakened immune systems, as there is no risk of vaccine-derived poliovirus infection.
For infants and young children, the Centers for Disease Control and Prevention (CDC) recommends a series of four doses of IPV, starting at 2 months of age, followed by doses at 4 months, 6–18 months, and 4–6 years. Each dose is typically 0.5 mL, administered intramuscularly in the vastus lateralis muscle of the thigh for infants and young children, or in the deltoid muscle of the upper arm for older children and adults. Adhering to this schedule is critical, as it ensures the development of robust immunity against all three poliovirus types.
Healthcare providers must follow precise techniques when administering IPV to maximize efficacy and minimize discomfort. The injection site should be cleaned with an alcohol swab, and the needle inserted at a 90-degree angle for intramuscular administration. For subcutaneous injections, a 45-degree angle is used. After administration, the site should be gently pressed with a dry cotton ball, but a bandage is usually unnecessary. Parents and caregivers can help by distracting young children during the procedure and applying a cool compress afterward to reduce soreness.
One of the key advantages of IPV is its safety profile, particularly for immunocompromised individuals who cannot receive live vaccines. However, it’s important to note that IPV does not induce intestinal immunity as effectively as OPV, which means vaccinated individuals can still carry and transmit the virus, albeit rarely. This limitation underscores the importance of high vaccination coverage to achieve herd immunity and eradicate polio globally.
In summary, IPV administration via injection is a cornerstone of polio prevention, offering a safe and effective way to protect individuals of all ages. By following recommended schedules, proper injection techniques, and post-vaccination care, healthcare providers and caregivers can ensure optimal immunity and contribute to the global effort to eliminate polio.
US Banks and Ignition Poker: A Risky Relationship?
You may want to see also
Explore related products






![]()
OPV vs. IPV Comparison
The polio vaccine exists in two primary forms: Oral Polio Vaccine (OPV) and Inactivated Polio Vaccine (IPV). Each has distinct characteristics, administration methods, and use cases, making them suitable for different scenarios in global polio eradication efforts. Understanding their differences is crucial for healthcare providers, policymakers, and parents navigating vaccination choices.
Administration and Composition
OPV is administered orally, typically as two drops for infants and children. It contains live, attenuated (weakened) poliovirus strains, which replicate in the intestine, triggering immunity. IPV, on the other hand, is delivered via injection (intramuscular or intradermal) and consists of inactivated (killed) poliovirus strains. A standard IPV dose is 0.5 mL for children under 7 years and 0.5 mL for older individuals, often given in combination with other vaccines like DTaP and Hepatitis B.
Immunity and Protection
OPV confers both humoral (bloodstream) and intestinal immunity, reducing viral shedding and transmission in communities. This makes it highly effective in outbreak settings. However, IPV primarily provides humoral immunity, offering strong individual protection but limited impact on viral circulation. For comprehensive immunity, many countries use a sequential schedule: IPV for initial doses (to avoid rare vaccine-derived polio cases from OPV) followed by OPV boosters to enhance gut immunity.
Advantages and Limitations
OPV’s oral delivery is logistically advantageous, requiring no needles and enabling mass vaccination campaigns in low-resource areas. However, its live virus component can, in rare cases (1 in 2.7 million doses), cause vaccine-associated paralytic polio (VAPP). IPV eliminates this risk but demands cold chain maintenance and trained personnel for injection. Cost-wise, OPV is significantly cheaper, while IPV’s higher price reflects production complexity and administration needs.
Global Usage and Recommendations
The World Health Organization (WHO) recommends OPV for routine immunization in polio-endemic regions due to its herd immunity benefits. IPV is favored in polio-free countries to avoid VAPP risks. For travelers to high-risk areas, a single IPV booster is advised, even if previously vaccinated with OPV. Parents should follow local health guidelines, ensuring children complete the full vaccine series (e.g., 4 OPV doses or 3–4 IPV doses, depending on the country).
Practical Tips for Caregivers
For OPV, ensure the child swallows the drops without spitting. Avoid feeding 30 minutes prior if the child is unwell. IPV injections may cause mild soreness at the site; apply a cold compress if needed. Keep vaccination cards updated, as some regions require proof of polio vaccination for school enrollment or international travel. Always consult healthcare providers for personalized advice, especially for immunocompromised individuals or those with specific medical conditions.
HSBC vs. Traditional Banks: Unique Features and Global Banking Advantages
You may want to see also
Explore related products






![]()
Global Polio Vaccination Methods
The global fight against polio has relied on two primary vaccination methods: the oral polio vaccine (OPV) and the inactivated polio vaccine (IPV), administered via injection. Each method has distinct advantages, limitations, and roles in eradication efforts, shaped by factors like cost, ease of delivery, and immunological outcomes. Understanding these differences is critical for tailoring vaccination strategies to local contexts and achieving global polio eradication.
Oral Polio Vaccine (OPV): The Workhorse of Eradication
OPV, a live-attenuated vaccine, is administered orally in drops, typically to children under 5 years old. Its simplicity—requiring no needles or trained medical personnel—makes it ideal for mass immunization campaigns in low-resource settings. A single dose costs as little as $0.12, and the vaccine confers both individual and community (herd) immunity by shedding the weakened virus, indirectly protecting unvaccinated individuals. However, rare cases of vaccine-derived poliovirus (VDPV) can emerge in underimmunized populations, necessitating supplementary IPV use in later stages of eradication.
Inactivated Polio Vaccine (IPV): The Safety Net
IPV, delivered via intramuscular or intradermal injection, contains killed poliovirus and eliminates the risk of VDPV. It is often used in high-income countries or as part of combination vaccines (e.g., DTaP-IPV-Hib). While IPV does not induce intestinal immunity, it provides robust humoral immunity, preventing paralytic disease. Its higher cost ($2–$3 per dose) and logistical requirements (trained staff, sterile needles) limit its use in mass campaigns but make it essential for sustaining polio-free regions.
Hybrid Strategies: Combining OPV and IPV
Global vaccination programs increasingly adopt hybrid approaches, leveraging the strengths of both vaccines. For instance, the World Health Organization recommends a "sequential schedule" of one IPV dose followed by multiple OPV doses, balancing safety and efficacy. In polio-endemic regions, bivalent OPV (types 1 and 3) is prioritized, while IPV is introduced to address type 2 VDPV risks. Practical tips include administering OPV on the tongue for infants and ensuring IPV is stored at 2–8°C to maintain potency.
Regional Adaptations: Tailoring Methods to Context
Vaccination methods vary by region based on polio prevalence, infrastructure, and cultural acceptance. In conflict zones or hard-to-reach areas, OPV’s ease of distribution is invaluable, while IPV is favored in countries transitioning to post-eradication strategies. For example, India’s successful eradication relied on door-to-door OPV campaigns, while the U.S. uses IPV exclusively to prevent VDPV cases. Age-specific protocols, such as administering IPV at 2, 4, and 6–18 months, ensure comprehensive protection across populations.
Future Directions: Innovations and Challenges
As polio nears eradication, innovations like fractional-dose IPV (0.1 mL intradermally) and novel OPV formulations aim to reduce costs and improve accessibility. However, challenges persist, including vaccine hesitancy, supply chain disruptions, and the need for sustained political commitment. By understanding the unique roles of OPV and IPV, global health initiatives can adapt strategies to overcome these barriers and ensure a polio-free world.
How to Easily Request a Bank Certificate from UnionBank
You may want to see also
Explore related products






![]()
Side Effects of Both Vaccines
The polio vaccine exists in two primary forms: oral (OPV) and injectable (IPV). Both are highly effective in preventing polio, but they come with distinct side effect profiles that individuals and healthcare providers should consider. Understanding these differences is crucial for informed decision-making, especially in regions where both vaccines are available.
Analytical Perspective:
The oral polio vaccine (OPV) is a live-attenuated vaccine, meaning it contains a weakened form of the polio virus. While it stimulates robust immunity, including gut immunity, it carries a rare but serious risk: vaccine-associated paralytic polio (VAPP). This occurs in approximately 1 in 2.7 million doses, primarily in individuals with weakened immune systems. In contrast, the inactivated polio vaccine (IPV), administered via injection, is a killed-virus vaccine with no risk of VAPP. However, IPV does not induce gut immunity, making it less effective in stopping viral transmission in communities. The choice between OPV and IPV often hinges on balancing individual safety with public health goals.
Instructive Approach:
Common side effects of OPV are generally mild and include fever, irritability, and loss of appetite in children. These symptoms typically resolve within a few days and can be managed with over-the-counter fever reducers like acetaminophen. IPV, on the other hand, may cause soreness, redness, or swelling at the injection site. Rarely, individuals may experience mild fever or fatigue. For both vaccines, it’s essential to monitor recipients, especially infants and young children, and follow the recommended dosage schedules: OPV is typically given in multiple doses starting at 6 weeks of age, while IPV is administered in a series of 3–4 doses, depending on the country’s immunization program.
Comparative Insight:
While OPV’s risk of VAPP is a significant concern, it remains the vaccine of choice in polio-endemic regions due to its ease of administration (oral drops) and ability to interrupt viral transmission. IPV, though safer in terms of paralytic risks, requires trained personnel for injection and is more costly, making it less accessible in resource-limited settings. For travelers or individuals in non-endemic areas, IPV is often preferred due to its safety profile. Notably, some countries use a sequential schedule, starting with IPV to minimize VAPP risk and following up with OPV to enhance gut immunity.
Persuasive Argument:
Despite their side effects, both polio vaccines are overwhelmingly safe and lifesaving. The benefits of protection against a debilitating and potentially fatal disease far outweigh the risks. For parents and caregivers, staying informed about the vaccine type being administered and adhering to the recommended schedule is key. Healthcare providers should educate recipients about potential side effects and emphasize the importance of completing the full vaccination series to ensure long-term immunity. In the global fight against polio, both OPV and IPV play indispensable roles, each with its unique advantages and considerations.
Practical Tips:
If your child receives OPV, avoid close contact with immunocompromised individuals for 6 weeks post-vaccination, as the live virus can shed in stool. For IPV, apply a cold compress to the injection site if swelling occurs. Always report severe or persistent symptoms to a healthcare provider. Remember, the choice of vaccine may depend on regional guidelines, availability, and individual health status, so consult a healthcare professional for personalized advice.
Exploring Banking Careers: Degrees to Launch Your Financial Journey
You may want to see also
Frequently asked questions
Both forms exist. The oral polio vaccine (OPV) is given as drops, while the inactivated polio vaccine (IPV) is administered via injection.
The inactivated polio vaccine (IPV), given by injection, is more commonly used globally due to its safety profile and effectiveness.
Yes, the oral polio vaccine (OPV) is still used in some countries, particularly in regions where polio remains endemic, as it provides better intestinal immunity.
Both vaccines are effective, but they work differently. IPV provides strong protection against paralytic polio, while OPV offers additional protection against poliovirus transmission in the gut.
The choice depends on your location and public health recommendations. In most countries, IPV is the standard, but OPV may be used in specific campaigns or regions. Consult your healthcare provider for guidance.