The question of whether the tetanus vaccine elicits an antibody-dependent cellular cytotoxicity (ADCC) response is an intriguing one, as ADCC is typically associated with viral and certain bacterial infections, rather than toxin-mediated diseases like tetanus. The tetanus vaccine primarily induces the production of neutralizing antibodies against the tetanus toxin, which prevent it from binding to nerve cells and causing disease. While ADCC involves the recruitment of immune cells, such as natural killer (NK) cells, to eliminate infected cells coated with antibodies, the tetanus toxin does not infect cells in the traditional sense, making ADCC an unlikely mechanism of action for the vaccine. However, research into the broader immune responses triggered by the tetanus vaccine, including potential interactions with immune cells, continues to explore whether secondary mechanisms like ADCC could play a role in enhancing immunity or contributing to vaccine efficacy.
Explore related products






What You'll Learn
![]()
Mechanism of ADCC in Tetanus Vaccine
The tetanus vaccine primarily induces humoral immunity by generating neutralizing antibodies against tetanus toxin, but its interaction with antibody-dependent cellular cytotoxicity (ADCC) remains a nuanced topic. ADCC typically involves antibodies binding to pathogen-infected cells, recruiting immune effectors like natural killer (NK) cells, and eliminating the target. While tetanus toxin does not infect cells directly, recent studies suggest that anti-tetanus antibodies may indirectly engage ADCC mechanisms in specific contexts. For instance, if tetanus toxin binds to neuronal cells, these toxin-antibody complexes could theoretically trigger ADCC, though this pathway is not the vaccine’s primary mode of action.
To explore this mechanism, consider the vaccine’s composition: the tetanus toxoid (inactivated toxin) in formulations like Tdap (Tetanus, Diphtheria, Pertussis) or DT (Diphtheria, Tetanus) stimulates B cells to produce IgG antibodies. These antibodies neutralize free toxin in the bloodstream, preventing it from reaching neurons. However, if toxin binds to cell surfaces, IgG antibodies could bridge the toxin-cell complex to FcγRIIIa receptors on NK cells, initiating ADCC. This process would involve perforin and granzyme release, leading to target cell lysis. While this scenario is plausible, it is not the vaccine’s intended function, as systemic toxin neutralization remains the primary defense.
Clinically, the tetanus vaccine is administered as a 0.5 mL intramuscular dose, with booster recommendations every 10 years for adults. For children, the DTaP series (Diphtheria, Tetanus, Pertussis) is given at 2, 4, 6, and 15–18 months, followed by a booster at 4–6 years. While ADCC is not a focus in vaccine design, understanding its potential role highlights the complexity of immune responses. For instance, individuals with compromised humoral immunity might benefit from ADCC-enhancing therapies, though this remains speculative in tetanus vaccination.
A comparative analysis reveals that vaccines like influenza or COVID-19 mRNA vaccines explicitly leverage ADCC by targeting infected cells, whereas the tetanus vaccine’s efficacy relies on toxin neutralization. However, the indirect ADCC pathway could serve as a secondary defense, particularly in severe cases where toxin binds to tissues. Practical tips for healthcare providers include ensuring proper dosing and adhering to schedules, as consistent antibody levels are critical for both neutralization and any potential ADCC activity.
In conclusion, while the tetanus vaccine’s primary mechanism is toxin neutralization, its interaction with ADCC warrants further investigation. This dual-functionality underscores the immune system’s adaptability and provides a basis for future vaccine enhancements. For now, adherence to established protocols remains the cornerstone of tetanus prevention.
Mixing Vaccines: Benefits, Risks, and What Science Says
You may want to see also
Explore related products




![]()
Role of Antibodies in Tetanus Vaccine Response
The tetanus vaccine primarily elicits a humoral immune response, where antibodies play a critical role in neutralizing the toxin produced by *Clostridium tetani*. Unlike vaccines that rely on antibody-dependent cellular cytotoxicity (ADCC), the tetanus vaccine’s efficacy hinges on the production of antitoxin antibodies that directly bind and inactivate tetanospasmin, the potent neurotoxin responsible for tetanus symptoms. These antibodies circulate in the bloodstream, acting as a first line of defense to prevent toxin binding to nerve terminals, thereby halting disease progression.
Consider the mechanism: upon vaccination, the toxoid (a non-toxic form of the toxin) stimulates B cells to differentiate into plasma cells, which secrete IgG antibodies. These antibodies are highly specific to tetanospasmin and provide long-term immunity. For instance, a standard tetanus toxoid vaccine (e.g., Td or Tdap) administered at a dose of 0.5 mL intramuscularly in adults induces protective antitoxin levels in over 95% of recipients within 2–4 weeks. Booster doses every 10 years maintain this immunity, ensuring rapid antibody response upon exposure to the toxin.
A comparative analysis highlights the contrast with ADCC-mediated vaccines, such as those targeting viral pathogens like HIV or certain cancers. In ADCC, antibodies tag infected cells for destruction by immune cells like natural killer (NK) cells. Tetanus, however, does not involve cellular infection; the toxin acts extracellularly, making direct neutralization by antibodies the most effective strategy. This distinction underscores why the tetanus vaccine’s design focuses on antitoxin production rather than ADCC activation.
Practical tips for optimizing antibody response include ensuring timely vaccination, especially for at-risk groups like children (who receive DTaP at 2, 4, 6, and 15–18 months) and older adults. Adverse reactions are rare but can include localized pain or swelling at the injection site. For individuals with uncertain vaccination histories, a single dose of Tdap followed by Td boosters is recommended. Understanding the antibody-centric mechanism of the tetanus vaccine not only clarifies its efficacy but also emphasizes the importance of adherence to vaccination schedules for sustained protection.
Mastering Citations: A Guide to Citing RCSB Protein Data Bank
You may want to see also
![]()
Tetanus Toxoid and ADCC Activation Pathways
The tetanus toxoid vaccine, a cornerstone of preventive medicine, primarily elicits a humoral immune response by generating neutralizing antibodies against tetanus toxin. However, emerging research suggests that antibody-dependent cellular cytotoxicity (ADCC) may play a secondary, yet significant role in its protective mechanism. ADCC is a process where antibodies bind to target cells and engage immune effector cells, such as natural killer (NK) cells, to eliminate pathogens. While not the primary mode of action for the tetanus vaccine, understanding its potential involvement in ADCC pathways could enhance our appreciation of its immunological breadth.
To explore this, consider the vaccine’s composition and administration. Tetanus toxoid is typically administered as part of the DTaP (diphtheria, tetanus, and acellular pertussis) vaccine for children under 7 years old, with booster doses (Tdap or Td) recommended every 10 years for adults. The vaccine contains inactivated tetanus toxin (toxoid), which stimulates B cells to produce antitoxin antibodies. These antibodies primarily neutralize circulating tetanus toxin, preventing it from binding to nerve endings and causing spasms. However, in vitro studies have shown that certain IgG subclasses produced in response to tetanus toxoid can engage Fcγ receptors on NK cells, potentially triggering ADCC. This suggests that while neutralization is the dominant mechanism, ADCC could contribute to clearing toxin-producing bacteria or toxin-affected cells.
A comparative analysis of ADCC in tetanus vaccination versus other vaccines, such as those for viral pathogens, highlights its unique role. Unlike vaccines targeting viruses like HIV or influenza, where ADCC is a critical component of protection due to the need to eliminate infected cells, tetanus toxoid’s primary target is a soluble toxin rather than an intracellular pathogen. Yet, the vaccine’s ability to induce IgG1 and IgG3 subclasses, which are potent ADCC mediators, indicates a latent capacity for this pathway. This duality underscores the vaccine’s robust design, which may offer additional layers of defense beyond toxin neutralization.
Practically, this insight could inform vaccine optimization strategies. For instance, adjuvants that enhance ADCC-inducing antibody production could be explored to bolster the vaccine’s efficacy, particularly in high-risk populations like the elderly or immunocompromised individuals. Additionally, understanding ADCC’s role could guide the development of combination vaccines that leverage both neutralization and cellular immunity. For healthcare providers, recognizing the vaccine’s potential ADCC activity reinforces the importance of adhering to recommended dosing schedules (e.g., 0.5 mL intramuscularly for adults) to ensure robust antibody production and maximize protective mechanisms.
In conclusion, while the tetanus toxoid vaccine’s primary function remains toxin neutralization, its interaction with ADCC pathways represents an intriguing secondary mechanism. This knowledge not only deepens our understanding of vaccine immunology but also opens avenues for innovation in vaccine design and administration. By appreciating the multifaceted nature of the immune response to tetanus toxoid, we can better harness its full protective potential.
Disputing Bank Charges: A Step-by-Step Guide to Calling Your Bank
You may want to see also
![]()
Immune Cell Involvement in Tetanus Vaccine ADCC
The tetanus vaccine, a cornerstone of preventive medicine, primarily elicits a humoral immune response, generating neutralizing antibodies against tetanus toxin. However, emerging research suggests that antibody-dependent cellular cytotoxicity (ADCC) may also play a role in its protective mechanism. ADCC involves the binding of antibodies to target cells, which are then recognized and eliminated by immune effector cells such as natural killer (NK) cells, macrophages, and neutrophils. While the tetanus vaccine’s efficacy is traditionally attributed to toxin neutralization, understanding its potential to induce ADCC could reveal additional layers of immune protection.
To explore this, consider the vaccine’s composition: it contains tetanus toxoid, an inactivated form of the toxin, which stimulates B cells to produce antitoxin antibodies. These antibodies are critical for neutralizing free tetanus toxin in the bloodstream. However, if these antibodies also engage Fc receptors on immune cells, they could trigger ADCC, enhancing the clearance of toxin-producing bacteria or toxin-affected cells. For instance, NK cells, which express FcγRIIIa, could be activated upon antibody binding, leading to the release of cytotoxic granules and targeted cell lysis. This mechanism, though not the primary focus of tetanus vaccination, could provide secondary defense against systemic toxin spread.
Practical implications of this involve optimizing vaccine formulations to enhance ADCC. Adjuvants like aluminum salts, commonly used in tetanus vaccines, primarily boost antibody production but could be paired with newer adjuvants like CpG oligonucleotides to stimulate NK cell activity. Additionally, dosing strategies, such as the standard 0.5 mL intramuscular injection for adults and children over 7 years, could be refined to maximize both antibody titers and ADCC potential. For example, a booster dose every 10 years maintains protective antibody levels, but future research could assess whether these doses also sustain ADCC-competent antibodies.
A comparative analysis with other vaccines, such as those for pertussis or influenza, highlights the uniqueness of tetanus vaccination. Unlike pertussis, where ADCC is directly targeted against bacterial cells, tetanus toxin’s extracellular nature limits ADCC to toxin-bound antibodies and immune cell interactions. This distinction underscores the need for tailored research to confirm ADCC’s role in tetanus immunity. For instance, in vitro studies could assess NK cell activation in the presence of tetanus toxin-antibody complexes, while animal models could evaluate ADCC’s contribution to survival post-toxin exposure.
In conclusion, while the tetanus vaccine’s primary action remains toxin neutralization, its potential to engage ADCC mechanisms warrants investigation. This could not only deepen our understanding of vaccine-induced immunity but also inform the design of next-generation vaccines with enhanced protective capabilities. Clinicians and researchers alike should consider ADCC as a complementary pathway, particularly in vulnerable populations like the elderly or immunocompromised, where maximizing immune responses is critical. By integrating ADCC into the vaccine’s immunological profile, we may unlock new strategies to combat tetanus more effectively.
Hostage Situations in Bank Robberies: Frequency and Trends Explored
You may want to see also
![]()
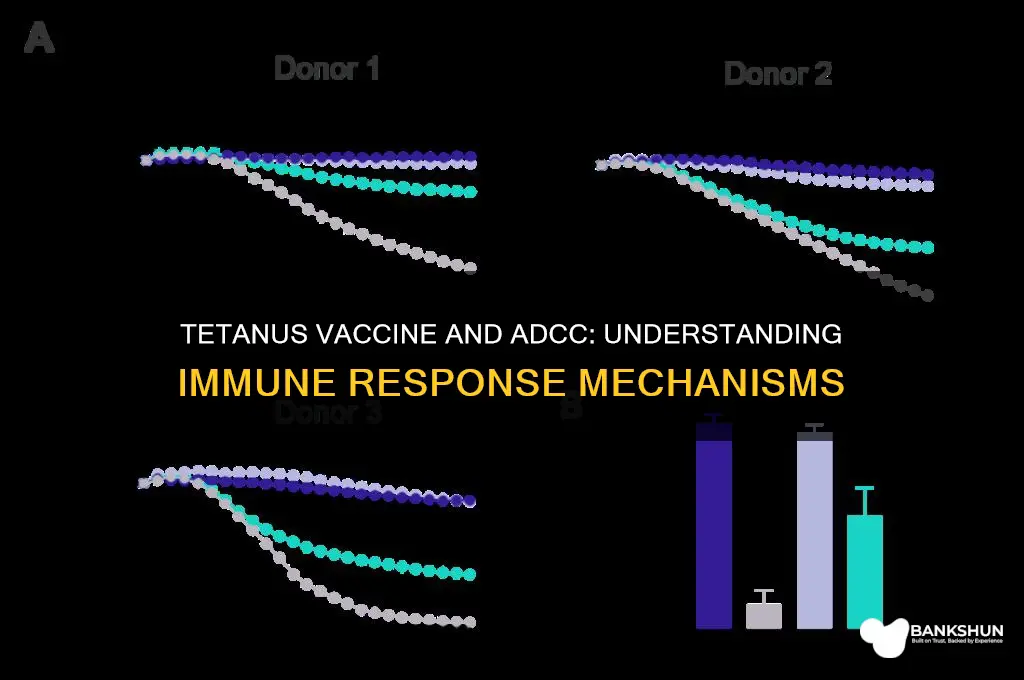
Clinical Evidence of ADCC in Tetanus Vaccination
The tetanus vaccine, primarily composed of tetanus toxoid (TT), has been a cornerstone of public health for decades, effectively preventing the severe neurological effects of tetanus infection. However, its mechanism of action extends beyond neutralizing toxins. Emerging clinical evidence suggests that the tetanus vaccine may elicit antibody-dependent cellular cytotoxicity (ADCC), a process where antibodies tag infected cells for destruction by immune cells like natural killer (NK) cells. This phenomenon could enhance the vaccine’s protective efficacy by targeting toxin-producing *Clostridium tetani* bacteria or toxin-affected cells more comprehensively.
One key study investigated the ADCC response in individuals vaccinated with TT, particularly focusing on IgG antibodies produced post-vaccination. Researchers observed that these antibodies not only neutralized tetanus toxin but also bound to Fcγ receptors on NK cells, triggering their cytotoxic activity. This dual functionality highlights a potential secondary mechanism of protection, especially in scenarios where toxin neutralization alone might be insufficient. For instance, in cases of deep puncture wounds or surgical sites, where bacterial load could be high, ADCC may play a critical role in eliminating toxin-producing bacteria before they cause systemic harm.
Clinically, this evidence has practical implications for vaccination protocols. The standard TT dose (0.5 mL intramuscularly) in adults and children over 7 years old is known to induce robust antibody responses, but optimizing ADCC activity may require adjuvanted formulations or booster schedules. For example, pregnant women receiving tetanus-diphtheria-pertussis (Tdap) vaccines could benefit from enhanced ADCC responses to protect both mother and neonate, as maternal antibodies transfer across the placenta and provide passive immunity. Similarly, travelers to high-risk areas might require accelerated booster doses to maximize both neutralizing and ADCC-mediated immunity.
A comparative analysis of ADCC activity in vaccinated populations versus natural infection survivors further supports this hypothesis. Survivors of tetanus often exhibit higher levels of IgG antibodies with ADCC capabilities, suggesting that vaccination could mimic this protective profile. However, unlike natural infection, vaccination avoids the risks of tetanus-induced muscle spasms, respiratory failure, or death. This makes the ADCC-inducing potential of the tetanus vaccine a safer, yet equally effective, strategy for long-term immunity.
In conclusion, while the tetanus vaccine’s primary role remains toxin neutralization, its ability to induce ADCC provides an additional layer of defense. Clinicians and public health officials should consider this evidence when designing vaccination campaigns, particularly in high-risk populations. Future research should focus on quantifying ADCC responses across different age groups and vaccine formulations to refine dosing and scheduling, ensuring optimal protection against this preventable disease.
Bankruptcy: What Happens When Banks Fail?
You may want to see also
Frequently asked questions
No, the tetanus vaccine primarily stimulates the production of neutralizing antibodies against the tetanus toxin, not ADCC. ADCC is typically associated with vaccines targeting pathogens like viruses or certain bacteria, not toxins.
The tetanus vaccine does not elicit an ADCC-like response. Its mechanism focuses on generating antitoxins to neutralize the tetanus toxin, rather than activating immune cells for cytotoxicity.
No, ADCC is not a component of the immune response to the tetanus vaccine. The vaccine’s effectiveness relies on humoral immunity, specifically the production of antibodies to block the toxin.
The tetanus vaccine does not interact with ADCC pathways. It targets the toxin directly through antibodies, not through cell-mediated cytotoxicity mechanisms like ADCC.
Yes, vaccines like those for influenza, HIV, and certain bacterial infections are being studied for their potential to induce ADCC. However, the tetanus vaccine operates through a different immunological pathway.