The question of whether vaccines alone are sufficient to end a pandemic is a critical and complex one, as it involves not only the efficacy of the vaccines themselves but also broader public health strategies, global distribution, and individual behaviors. While vaccines have proven to be a cornerstone in reducing severe illness, hospitalizations, and deaths, their ability to completely halt a pandemic depends on several factors, including vaccination rates, the emergence of new variants, and the equitable distribution of doses worldwide. High vaccination coverage can significantly slow the spread of the virus and reduce its impact, but achieving herd immunity remains challenging, especially in regions with limited access to vaccines or where hesitancy persists. Additionally, the virus’s ability to mutate and the potential waning of vaccine immunity over time underscore the need for complementary measures such as masking, testing, and continued research into booster shots and new treatments. Thus, while vaccines are a powerful tool, they are likely just one part of a multifaceted approach required to control and eventually end a pandemic.
Explore related products



$5.99 $12.99



What You'll Learn
![]()
Vaccine efficacy against variants
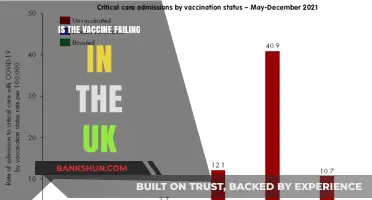
The emergence of SARS-CoV-2 variants has raised critical questions about vaccine efficacy. While initial vaccines demonstrated remarkable effectiveness against the original strain, their performance against variants like Delta and Omicron has varied. Studies show that two doses of mRNA vaccines (Pfizer-BioNTech, Moderna) provide approximately 60-70% protection against symptomatic infection from Omicron, compared to 95% against the original strain. This decline underscores the virus's ability to evade immune responses, even in vaccinated individuals.
Consider the role of booster doses in restoring efficacy. A third dose of mRNA vaccines significantly enhances protection, increasing neutralizing antibody levels by 20- to 30-fold. For instance, a booster shot raises efficacy against symptomatic Omicron infection to around 75%, according to data from the UK Health Security Agency. This highlights the importance of timely boosters, particularly for vulnerable populations such as those over 65 or immunocompromised. Practical advice: follow local health guidelines for booster eligibility, typically recommended 3-6 months after the second dose.
Comparing vaccine types reveals differences in variant protection. Viral vector vaccines (AstraZeneca, Johnson & Johnson) show lower efficacy against Omicron, with approximately 40-50% protection after two doses. However, heterologous boosting—combining different vaccine types—has shown promise. A study in *The Lancet* found that an mRNA booster following a viral vector prime restored efficacy to levels comparable to mRNA-only regimens. This strategy offers flexibility for regions with limited vaccine availability.
Despite reduced efficacy against infection, vaccines remain highly effective at preventing severe disease and hospitalization across variants. Data from South Africa during the Omicron wave showed that vaccinated individuals were 70-80% less likely to require hospitalization compared to the unvaccinated. This protection is attributed to memory cells and T-cell responses, which target conserved viral regions less prone to mutation. Key takeaway: vaccines are not a perfect shield against infection, but they are a critical barrier against severe outcomes.
Finally, ongoing research into variant-specific vaccines offers a path forward. Pfizer and Moderna have begun trials for Omicron-tailored boosters, expected to provide more durable and targeted immunity. Until these become available, layering non-pharmaceutical interventions—masking, ventilation, and testing—with vaccination remains essential. Practical tip: monitor public health updates for access to updated vaccines and adjust preventive measures accordingly. Vaccine efficacy against variants is a dynamic challenge, but with adaptive strategies, it remains a cornerstone of pandemic control.
Hepatitis A Vaccine for Adults: Essential or Optional Protection?
You may want to see also
Explore related products






![]()
Global vaccine distribution challenges
The COVID-19 pandemic has underscored a harsh reality: vaccines alone cannot end a global health crisis without equitable distribution. While wealthy nations hoard doses, administering boosters to healthy adults, low-income countries struggle to secure even a first dose for their most vulnerable populations. This disparity isn't just a moral failing; it's a strategic blunder. As long as the virus circulates unchecked in underserved regions, it mutates, creating new variants that threaten global progress.
Omicron's emergence, for instance, highlighted the consequences of vaccine inequality. South Africa, with its relatively robust healthcare system, identified the variant due to its genomic surveillance capabilities. However, the global response was marred by travel bans targeting African nations, rather than addressing the root cause: insufficient vaccine access. This reactive approach, fueled by vaccine nationalism, prolongs the pandemic and undermines collective immunity.
Consider the logistical hurdles. Many vaccines require ultra-cold storage, a challenge in regions with unreliable electricity or limited infrastructure. The Pfizer-BioNTech vaccine, for example, needs storage at -70°C, while Moderna's can be stored at -20°C. AstraZeneca's vaccine, stable at refrigerator temperatures, offered a solution, but hesitancy and supply chain issues hindered its distribution. Additionally, the complexity of multi-dose regimens, like the two-dose Pfizer and Moderna vaccines or the single-dose Johnson & Johnson vaccine, complicates administration, particularly in areas with limited healthcare workers.
Simplifying distribution requires innovative solutions. COVAX, a global initiative aimed at equitable vaccine access, has faced funding shortfalls and supply delays. Wealthy nations must fulfill their dose-sharing pledges and support technology transfers to enable local vaccine production in low-income countries. Furthermore, investing in cold chain infrastructure and training healthcare workers in remote areas is crucial.
Ultimately, overcoming global vaccine distribution challenges demands a shift from nationalistic hoarding to global solidarity. The pandemic has exposed the fragility of our interconnected world. Only through equitable vaccine access, coupled with robust public health measures, can we hope to control this pandemic and prevent future ones. This requires not just charity, but a recognition that global health security is a shared responsibility.
Understanding the Federal Reserve Bank's Organizational Structure and Functions
You may want to see also
Explore related products






![]()
Public trust and hesitancy issues
Public trust in vaccines has historically been a cornerstone of pandemic control, yet hesitancy remains a persistent barrier. During the COVID-19 pandemic, for instance, vaccine rollout was hindered in many regions by skepticism fueled by misinformation, political polarization, and a lack of transparent communication. A 2021 study published in *Nature Medicine* found that countries with higher vaccine hesitancy rates saw slower declines in infection rates, even when vaccines were widely available. This highlights a critical truth: the efficacy of vaccines in ending a pandemic depends not just on their scientific design but on the public’s willingness to accept them. Without trust, even the most effective vaccine becomes a tool left unused.
Building trust requires more than scientific data; it demands empathy and tailored communication strategies. For example, addressing hesitancy among pregnant individuals or parents of young children (ages 5–11, a group often skeptical of new vaccines) involves acknowledging their specific concerns about safety and long-term effects. Providing clear, accessible information about clinical trial results, such as the Pfizer vaccine’s 91% efficacy in children aged 5–11, can alleviate fears. Equally important is involving trusted community leaders—religious figures, healthcare workers, or local influencers—to deliver messages in culturally sensitive ways. A one-size-fits-all approach fails; trust is built through personalized, respectful dialogue.
Misinformation spreads faster than any virus, and combating it is essential to fostering trust. During the COVID-19 pandemic, false claims about vaccines causing infertility or altering DNA proliferated on social media, particularly among younger age groups (18–35). Platforms like Facebook and Twitter eventually implemented fact-checking tools, but the damage was already done in many cases. To counter this, public health campaigns must preemptively address common myths with evidence-based responses. For instance, explaining that mRNA vaccines (like Moderna and Pfizer) do not interact with human DNA and degrade quickly after vaccination can dispel unfounded fears. Proactive, transparent communication is the antidote to misinformation.
Finally, hesitancy is often rooted in systemic failures, not individual ignorance. Communities with historical reasons to distrust medical institutions, such as African American populations in the U.S., require acknowledgment of past injustices like the Tuskegee Syphilis Study. Rebuilding trust in these groups involves not just education but actions that demonstrate respect and equity. For example, ensuring vaccine distribution sites are accessible in underserved neighborhoods and involving community members in decision-making processes can signal a commitment to fairness. Trust is not earned through words alone but through consistent, equitable actions that address the root causes of skepticism.
Generate UPI PIN for ICICI Bank: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Booster shots necessity and timing
The effectiveness of initial COVID-19 vaccines in preventing severe illness and death has been well-documented, but their ability to curb transmission and provide long-term immunity remains a critical question. As new variants emerge and antibody levels wane over time, booster shots have become a central topic in pandemic management. The necessity and timing of these boosters hinge on several factors, including individual health status, vaccine type, and the evolving nature of the virus. For instance, studies show that mRNA vaccine efficacy against symptomatic infection drops from around 95% to 50-60% six months after the second dose, underscoring the need for additional protection.
From a practical standpoint, determining the optimal timing for booster shots requires balancing scientific data with real-world logistics. Health authorities, such as the CDC and WHO, recommend boosters for vulnerable populations—including those over 65, immunocompromised individuals, and frontline workers—starting six months after their initial series. For younger, healthier adults, the timeline may extend to eight months or more, depending on local transmission rates and variant prevalence. Pfizer-BioNTech and Moderna boosters are typically administered at half the dose of the primary series (25 micrograms and 50 micrograms, respectively), while Johnson & Johnson recipients receive a full dose as their booster.
A comparative analysis of booster campaigns across countries reveals varying strategies based on resource availability and population needs. Israel, an early adopter of boosters, saw a significant reduction in severe cases among older adults within weeks of administering third doses. In contrast, some low-income nations struggle to distribute even first doses, highlighting global inequities in vaccine access. This disparity raises ethical questions about prioritizing boosters in wealthy countries while others lack basic protection. Still, for regions with high vaccination rates, boosters serve as a critical tool to maintain immunity and prevent healthcare system overload.
Persuasively, the argument for boosters extends beyond individual protection to their role in ending the pandemic. By reducing viral transmission and the likelihood of new variants, widespread booster uptake could accelerate a return to normalcy. However, this requires clear communication from health officials to address hesitancy and misinformation. Practical tips for individuals include scheduling boosters during off-peak hours to avoid crowds, staying hydrated before vaccination, and planning for potential side effects, such as fatigue or mild fever, which typically resolve within 48 hours.
In conclusion, booster shots are not a luxury but a necessity in the ongoing fight against COVID-19. Their timing must be tailored to individual and community needs, guided by data and equity considerations. As the pandemic evolves, staying informed and proactive about booster recommendations remains essential for both personal and public health.
Is Fever Normal After 4-Month Vaccines? What Parents Should Know
You may want to see also
Explore related products






![]()
Role of masks and restrictions post-vaccination
Vaccines have proven to be a cornerstone in the fight against the pandemic, significantly reducing severe illness, hospitalizations, and deaths. However, the question remains: are they enough to stop the pandemic entirely? The emergence of variants and the uneven global distribution of vaccines highlight the need for complementary measures. Masks and restrictions, though often debated, continue to play a critical role even in post-vaccination scenarios. Their importance lies in addressing the gaps left by vaccines, such as breakthrough infections and the protection of vulnerable populations.
Consider the analytical perspective: while vaccines provide robust immunity, no vaccine is 100% effective. For instance, the Pfizer-BioNTech vaccine has an efficacy rate of approximately 95% against severe disease but offers slightly lower protection against infection, especially with variants like Delta and Omicron. Masks, particularly high-quality options like N95 or KN95 respirators, act as a physical barrier, reducing the transmission of respiratory droplets. In crowded or poorly ventilated spaces, masks can cut the risk of infection by up to 80%, according to studies from the CDC. Restrictions, such as capacity limits and social distancing, further minimize exposure by reducing contact between individuals. Together, these measures create a layered defense that vaccines alone cannot achieve.
From an instructive standpoint, implementing masks and restrictions post-vaccination requires clear guidelines. For example, individuals should wear masks in indoor public settings, especially in areas with high community transmission or low vaccination rates. Employers can enforce mask mandates in workplaces, while schools may require masks for students under 12, who are not yet eligible for certain vaccines. Restrictions should be tailored to local conditions: temporary closures of high-risk venues, such as nightclubs, may be necessary during outbreaks. Public health officials must communicate these measures effectively, emphasizing their role in protecting both the vaccinated and unvaccinated.
Persuasively, the continued use of masks and restrictions is not about fear but about responsibility. Vaccinated individuals can still carry and transmit the virus, particularly in the absence of symptoms. By wearing masks and adhering to restrictions, people contribute to herd immunity and protect those who cannot be vaccinated due to medical reasons or age. For instance, immunocompromised individuals, who make up 2-3% of the population, often mount a weaker response to vaccines and rely on community measures for safety. This collective effort is essential to prevent overwhelming healthcare systems and allowing economies to recover sustainably.
Comparatively, countries that have lifted masks and restrictions prematurely have faced resurgences in cases. For example, the UK’s "Freedom Day" in July 2021 led to a spike in infections, despite high vaccination rates. In contrast, Singapore maintained strict measures even with a 92% vaccination rate, resulting in lower transmission and fewer hospitalizations. This comparison underscores the importance of a cautious approach, where masks and restrictions are phased out gradually, based on data rather than deadlines.
In conclusion, while vaccines are a powerful tool, they are not enough to stop the pandemic on their own. Masks and restrictions serve as vital complements, addressing the limitations of vaccines and protecting vulnerable populations. By adopting a layered strategy, societies can maximize their defense against the virus and move toward a safer, more stable future. Practical steps, such as wearing high-quality masks in high-risk settings and tailoring restrictions to local conditions, ensure that these measures remain effective and sustainable. The role of masks and restrictions post-vaccination is clear: they are essential components of a comprehensive pandemic response.
Understanding Bank Cheque Validity: How Long Are They Good For?
You may want to see also
Frequently asked questions
No, the vaccine alone is not enough to stop the pandemic. While vaccines are highly effective at reducing severe illness, hospitalizations, and deaths, they are one of many tools needed. Additional measures like masking, testing, contact tracing, and global vaccine equity are crucial to control the spread and prevent new variants.
Yes, vaccinated individuals can still contract and spread the virus, especially with highly transmissible variants. While vaccines significantly reduce transmission, they are not 100% effective in preventing it. This means that widespread vaccination must be combined with other public health measures to minimize spread and protect vulnerable populations.
Global vaccination is essential because as long as the virus circulates in unvaccinated populations, it can mutate into new variants that may evade vaccines or cause more severe illness. Ensuring equitable access to vaccines worldwide is critical to reducing the virus's spread globally and ultimately ending the pandemic for everyone.