The question of whether vaccines are the same as antibodies is a common one, often arising from a misunderstanding of their roles in the immune system. Vaccines are biological preparations that stimulate the body’s immune response to a specific pathogen, such as a virus or bacterium, by introducing a harmless version or component of the pathogen. This process trains the immune system to recognize and combat the real pathogen if encountered in the future. Antibodies, on the other hand, are proteins produced by the immune system in response to the presence of foreign substances, known as antigens. While vaccines can induce the production of antibodies as part of the immune response, they are not the same; vaccines are a preventive tool that triggers immunity, whereas antibodies are a direct product of that immune response. Understanding this distinction is crucial for appreciating how vaccines work and their role in protecting against infectious diseases.
| Characteristics | Values |
|---|---|
| Definition | Vaccines are biological preparations that stimulate the immune system to produce antibodies and provide immunity against specific diseases. Antibodies are proteins produced by the immune system to neutralize pathogens. |
| Source | Vaccines are externally administered (e.g., injections). Antibodies are naturally produced by the body in response to vaccines, infections, or other immune stimuli. |
| Function | Vaccines prevent diseases by inducing immunity. Antibodies directly neutralize or mark pathogens for destruction. |
| Specificity | Vaccines target specific pathogens (e.g., COVID-19, flu). Antibodies are specific to the pathogen or antigen that triggered their production. |
| Duration | Vaccine-induced immunity can last months to years, depending on the vaccine. Antibody levels may decline over time, requiring booster shots. |
| Passive vs. Active Immunity | Vaccines provide active immunity by training the immune system. Antibodies can be part of passive immunity when transferred (e.g., monoclonal antibodies or maternal antibodies). |
| Production Time | Vaccines take time (days to weeks) to stimulate antibody production. Antibodies are produced naturally after vaccination or infection. |
| Types | Vaccines include live-attenuated, inactivated, mRNA, etc. Antibodies include IgG, IgM, IgA, etc., each with specific roles. |
| Role in Immunity | Vaccines are a preventive measure. Antibodies are a key component of the immune response. |
| Latest Data (2023) | mRNA vaccines (e.g., Pfizer, Moderna) induce robust antibody responses. Antibody levels wane over time, emphasizing the need for boosters. |
Explore related products






What You'll Learn
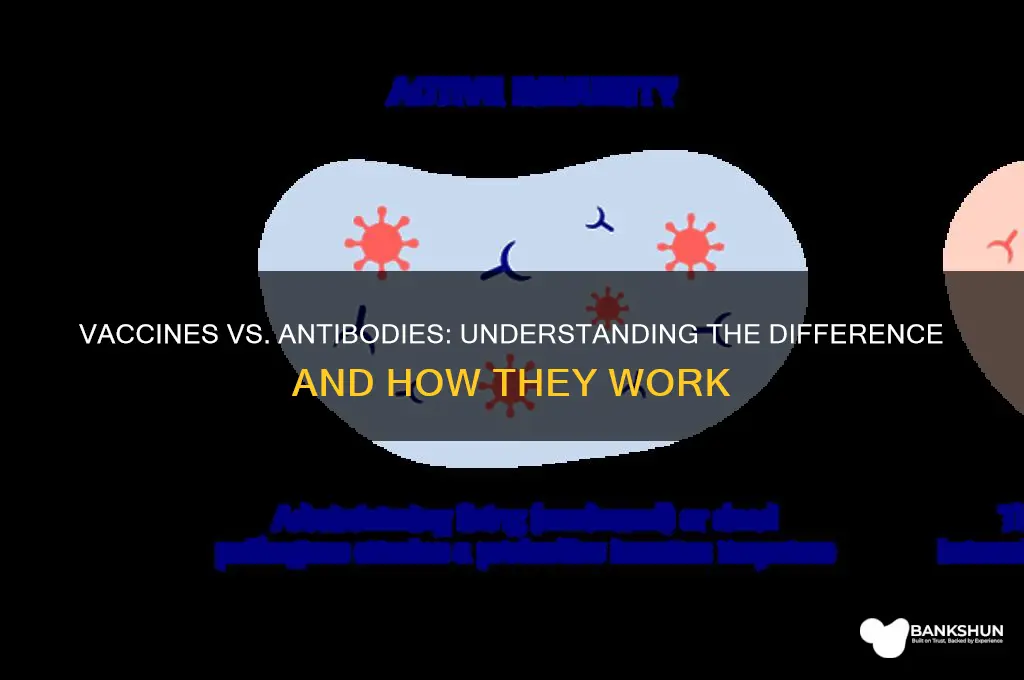
- Vaccines vs. Natural Immunity: Vaccines mimic infections to trigger antibody production without causing disease
- Passive Antibody Therapy: Direct antibody injection provides immediate but temporary protection, unlike vaccines
- Vaccine-Induced Antibodies: Vaccines stimulate the body to produce specific antibodies against pathogens
- Antibody Duration: Vaccine-generated antibodies may wane over time, requiring boosters
- Types of Antibodies: Vaccines primarily induce IgG antibodies, while infections may produce IgM first
![]()
Vaccines vs. Natural Immunity: Vaccines mimic infections to trigger antibody production without causing disease
Vaccines and natural immunity both aim to protect the body from disease, but they achieve this goal through fundamentally different mechanisms. Natural immunity occurs when a person contracts a disease, recovers, and their immune system retains a memory of the pathogen, producing antibodies to fend off future infections. This process, however, comes with the risk of severe illness, long-term complications, or even death. Vaccines, on the other hand, mimic infections by introducing a harmless version or component of the pathogen—such as a weakened virus, inactivated virus, or specific protein—to trigger antibody production without causing the disease itself. For example, the mRNA COVID-19 vaccines deliver genetic instructions for cells to produce the SARS-CoV-2 spike protein, prompting the immune system to generate antibodies and memory cells, all without exposing the individual to the virus.
Consider the practical differences in antibody generation. Natural immunity relies on the body’s direct encounter with a pathogen, often requiring a full-blown infection. Vaccines, however, streamline this process by presenting the immune system with a controlled, safe stimulus. For instance, the influenza vaccine contains inactivated virus particles, while the HPV vaccine uses virus-like particles to elicit an immune response. This precision reduces the risk of complications while ensuring robust antibody production. Dosage is another critical factor: vaccines are administered in carefully calibrated amounts, such as the 0.5 mL intramuscular injection for the Pfizer-BioNTech COVID-19 vaccine, to maximize efficacy without overwhelming the immune system.
The comparative safety of vaccines versus natural immunity cannot be overstated. Contracting a disease naturally exposes individuals to unpredictable outcomes, particularly in vulnerable populations like the elderly, immunocompromised, or those with pre-existing conditions. For example, measles infection carries a 1 in 500 risk of encephalitis, a potentially fatal brain inflammation, whereas the measles vaccine (MMR) has a negligible risk profile. Vaccines also offer herd immunity benefits, protecting those who cannot be vaccinated due to medical reasons. Natural immunity, while effective for the recovered individual, does not contribute to community-wide protection in the same way.
A key takeaway is that vaccines provide a safer, more controlled pathway to immunity than natural infection. They are designed to educate the immune system without the dangers of disease, making them a cornerstone of public health. For instance, the tetanus vaccine uses a toxoid—an inactivated form of the toxin—to generate antibodies, eliminating the risk of tetanus while conferring long-term protection. Practical tips for maximizing vaccine efficacy include adhering to recommended schedules (e.g., the two-dose regimen for COVID-19 vaccines spaced 3–4 weeks apart) and staying informed about booster requirements, especially for diseases like pertussis or influenza, where immunity wanes over time.
In summary, while both vaccines and natural immunity result in antibody production, vaccines achieve this through a safer, more controlled process that mimics infection without causing disease. Their precision, safety, and ability to confer herd immunity make them an indispensable tool in preventing illness and saving lives. Understanding this distinction empowers individuals to make informed decisions about their health and underscores the importance of vaccination in modern medicine.
Bank Fraud: A Hidden Form of Class Discrimination?
You may want to see also
Explore related products





![]()
Passive Antibody Therapy: Direct antibody injection provides immediate but temporary protection, unlike vaccines
Vaccines and antibodies are often conflated, yet they serve distinct roles in immunity. While vaccines stimulate the body to produce its own antibodies over weeks, passive antibody therapy offers a shortcut: direct injection of pre-formed antibodies for immediate protection. This method bypasses the immune system’s learning curve, making it particularly useful in emergencies, such as exposure to COVID-19 or rabies. However, this protection is fleeting, typically lasting weeks to months, as the injected antibodies degrade naturally. Vaccines, in contrast, confer long-term immunity by training the immune system to recognize and combat pathogens independently.
Consider a scenario where an unvaccinated individual is exposed to a high-risk virus. Passive antibody therapy, such as monoclonal antibody infusions, can be administered within a specific window—often 72 to 96 hours post-exposure—to neutralize the pathogen. For instance, COVID-19 monoclonal antibody treatments like casirivimab-imdevimab are given intravenously in doses ranging from 1,200 to 2,400 mg, depending on age and weight. This approach is especially critical for immunocompromised individuals who may not mount a robust response to vaccines. However, it’s not a replacement for vaccination; it’s a stopgap measure for immediate threats.
The mechanics of passive antibody therapy highlight its limitations. Unlike vaccines, which trigger memory B cells to produce antibodies on demand, injected antibodies do not confer lasting immunity. Once administered, they circulate in the bloodstream for a finite period, typically 3 to 6 weeks, before being cleared by the body. This makes it unsuitable for long-term prevention but ideal for acute situations, such as preventing severe illness in high-risk populations or treating toxin-mediated diseases like botulism. For example, rabies immune globulin is given alongside the rabies vaccine to provide instant protection while the vaccine takes effect.
Practical considerations underscore the niche role of passive antibody therapy. It’s resource-intensive, requiring precise timing, refrigeration, and healthcare access for administration. Vaccines, on the other hand, are cost-effective, scalable, and self-sustaining once administered. For instance, a single dose of the measles vaccine costs pennies and provides lifelong immunity, whereas antibody treatments for the same disease would be prohibitively expensive and short-lived. This disparity highlights why vaccines remain the cornerstone of public health, while passive therapy is reserved for targeted, urgent interventions.
In summary, passive antibody therapy and vaccines are not interchangeable but complementary tools. The former provides rapid, temporary protection in critical situations, while the latter builds enduring immunity through immune education. Understanding this distinction is key to deploying each strategy effectively, whether in individual treatment plans or public health campaigns. For those seeking immediate defense, passive therapy can be a lifesaver; for long-term resilience, vaccination remains unmatched.
Step-by-Step Guide to Updating Bank KYC in EPFO Easily
You may want to see also
Explore related products






![]()
Vaccine-Induced Antibodies: Vaccines stimulate the body to produce specific antibodies against pathogens
Vaccines are not antibodies, but they are the body's instructors for creating them. When a vaccine is administered, it introduces a harmless piece of a pathogen, such as a protein or a weakened virus, to the immune system. This triggers a response where B cells, a type of white blood cell, begin to produce antibodies specifically designed to recognize and neutralize the pathogen. For instance, the COVID-19 mRNA vaccines deliver genetic material that instructs cells to produce the spike protein of the SARS-CoV-2 virus, prompting the immune system to generate antibodies against it. This process mimics a natural infection but without the risk of severe disease, ensuring the body is prepared for future encounters with the actual pathogen.
The production of vaccine-induced antibodies is a highly specific and tailored process. Unlike natural infections, which expose the body to the entire pathogen, vaccines often target key components, ensuring a focused immune response. For example, the tetanus vaccine contains a toxoid—an inactivated form of the toxin produced by the bacterium *Clostridium tetani*. After receiving the recommended three-dose primary series (typically given at 2, 4, and 6 months of age, with boosters every 10 years), the body maintains a pool of memory B cells ready to rapidly produce antibodies if exposed to the toxin. This specificity is why vaccines are so effective at preventing diseases like tetanus, diphtheria, and pertussis, even though these pathogens are still present in the environment.
One critical aspect of vaccine-induced antibodies is their longevity and the concept of immunological memory. After the initial immune response, some B cells transform into long-lived memory cells that "remember" the pathogen. This memory allows the immune system to mount a faster and stronger response upon re-exposure, often preventing infection altogether. For example, the measles vaccine, typically given in two doses (the first at 12–15 months and the second at 4–6 years), provides lifelong immunity for 95% of recipients. This is because the vaccine induces high levels of neutralizing antibodies and robust memory B cells, ensuring protection even decades after vaccination.
However, not all vaccine-induced antibodies are created equal. The efficacy of antibody production depends on factors like age, underlying health conditions, and the type of vaccine. For instance, older adults may produce fewer antibodies in response to vaccines due to age-related immune decline, a phenomenon known as immunosenescence. To address this, some vaccines, like the shingles vaccine (Shingrix), require higher antigen doses or adjuvants to boost the immune response. Similarly, individuals with compromised immune systems, such as those undergoing chemotherapy, may require additional doses or alternative vaccination schedules to achieve adequate antibody levels.
Practical tips for maximizing vaccine-induced antibody production include staying hydrated, getting adequate sleep, and maintaining a healthy diet rich in nutrients like vitamin D and zinc, which support immune function. Avoiding stress and excessive alcohol consumption can also enhance vaccine efficacy. For travelers, ensuring vaccinations are up to date and receiving destination-specific vaccines (e.g., yellow fever or typhoid) well in advance of travel allows sufficient time for antibody production. Understanding how vaccines stimulate antibody production not only highlights their uniqueness compared to natural antibodies but also underscores their role as a cornerstone of preventive medicine.
Does US Bank Offer Trust Services? Exploring Their Department Options
You may want to see also
Explore related products






![]()
Antibody Duration: Vaccine-generated antibodies may wane over time, requiring boosters
Vaccines and antibodies are not the same, though they are closely linked in the body's defense system. Vaccines are biological preparations that stimulate the immune system to recognize and combat pathogens, often by introducing a weakened or inactivated form of the virus or bacteria. Antibodies, on the other hand, are proteins produced by the immune system in response to these pathogens, acting as the body's frontline soldiers against infection. While vaccines trigger the production of antibodies, they are not antibodies themselves. This distinction is crucial for understanding why vaccine-generated antibodies may wane over time, necessitating booster shots.
The duration of antibody protection varies depending on the vaccine and individual factors such as age, immune health, and exposure to the pathogen. For instance, the measles vaccine typically confers lifelong immunity, while the influenza vaccine requires annual administration due to the virus's rapid mutation. COVID-19 vaccines, such as Pfizer-BioNTech and Moderna, have shown a decline in antibody levels 6 to 8 months after the initial series, particularly in older adults and immunocompromised individuals. This decline does not mean the immune system is defenseless; memory cells retain the ability to mount a rapid response if exposed to the virus. However, waning antibodies increase the risk of breakthrough infections, especially with highly transmissible variants.
Booster doses are designed to reinvigorate the immune response by reintroducing the vaccine antigen. For COVID-19, studies show that a booster dose significantly increases antibody levels, reducing the risk of severe illness and hospitalization. The CDC recommends a booster shot 5 months after the initial Pfizer or Moderna series for individuals aged 12 and older, and 2 months after the Johnson & Johnson vaccine for all eligible adults. Timing is critical, as administering the booster too early may limit its effectiveness, while delaying it increases vulnerability during periods of high community transmission.
Practical considerations for maintaining antibody levels include staying informed about vaccine recommendations, particularly for those at higher risk. For example, individuals over 65 or with underlying health conditions may benefit from additional boosters. Tracking vaccination dates and setting reminders can ensure timely administration. Additionally, lifestyle factors such as adequate sleep, a balanced diet, and regular exercise support overall immune function, complementing the protection provided by vaccines. While boosters are essential for sustaining antibody levels, they are part of a broader strategy for long-term immunity.
In conclusion, vaccine-generated antibodies are a dynamic component of the immune system, subject to natural decline over time. Boosters serve as a critical tool to replenish these antibodies, particularly for vaccines with shorter durations of protection. Understanding this process empowers individuals to make informed decisions about their health, balancing scientific guidance with personal circumstances. As research continues to evolve, staying updated on vaccine efficacy and booster schedules remains key to maximizing protection against infectious diseases.
Fishers Stores: US Banks Accessibility and Availability
You may want to see also
Explore related products






![]()
Types of Antibodies: Vaccines primarily induce IgG antibodies, while infections may produce IgM first
Vaccines and natural infections both trigger the body’s immune response, but they do so in distinct ways, particularly in the types of antibodies they produce. Vaccines are designed to mimic an infection without causing illness, priming the immune system to recognize and combat a pathogen. In contrast, natural infections expose the body to the actual pathogen, often leading to a more immediate and varied immune reaction. Central to this difference is the type of antibodies generated: vaccines primarily induce IgG antibodies, while infections often produce IgM antibodies first. Understanding this distinction is key to appreciating how vaccines protect us and how our bodies respond to threats.
IgM antibodies are the first line of defense during a natural infection. They are large, pentameric molecules that appear early in the immune response, typically within days of exposure to a pathogen. Their primary role is to bind to antigens and activate the complement system, a cascade of immune responses that help neutralize pathogens. However, IgM antibodies are short-lived and less specific compared to IgG. For instance, during a viral infection like COVID-19, IgM antibodies are often detectable within the first week of symptoms, serving as an early marker of infection. In contrast, vaccines bypass this initial IgM response, focusing instead on generating high-affinity IgG antibodies, which are more durable and effective at neutralizing pathogens.
IgG antibodies, the primary focus of vaccination, are smaller, more versatile, and longer-lasting than IgM. They circulate in the bloodstream and tissues, providing sustained protection against reinfection. Vaccines achieve this by presenting a harmless piece of the pathogen (such as a protein or mRNA) to the immune system, prompting B cells to produce IgG antibodies tailored to that specific threat. For example, the COVID-19 mRNA vaccines induce IgG antibodies that target the virus’s spike protein, preventing it from entering cells. This process takes time—typically several weeks—but results in a robust and memory-based immune response. Booster doses further enhance IgG levels, ensuring prolonged immunity.
The timing and dosage of vaccines are critical to maximizing IgG production. Most vaccines require multiple doses spaced weeks or months apart to allow the immune system to mature its response. For instance, the Pfizer-BioNTech COVID-19 vaccine is administered in two doses, 3–4 weeks apart, with a booster recommended 6 months later. This staggered approach mimics the natural immune response, gradually increasing IgG levels and creating long-term memory cells. In contrast, natural infections often overwhelm the body with a high viral load, leading to rapid IgM production but also potential tissue damage. Vaccines, by delivering a controlled antigen dose, avoid this risk while achieving the same protective goal.
Practically, understanding the difference between IgM and IgG antibodies can guide medical decisions. For example, IgM tests are often used to diagnose acute infections, while IgG tests assess long-term immunity, such as after vaccination or recovery. Parents should ensure their children receive vaccines on schedule to build robust IgG immunity, especially for diseases like measles or whooping cough. Adults, particularly those over 65 or immunocompromised, should stay current with boosters to maintain IgG levels. By recognizing how vaccines and infections differ in antibody production, individuals can make informed choices to protect their health and that of their communities.
Does GoBank Charge for Insufficient Funds? Fees Explained
You may want to see also
Frequently asked questions
No, the vaccine is not the same as antibodies. A vaccine is a biological preparation that stimulates your immune system to produce antibodies, while antibodies are proteins produced by the immune system to fight off specific pathogens.
No, a vaccine does not directly give you antibodies. Instead, it teaches your immune system how to recognize and respond to a pathogen, prompting your body to produce its own antibodies over time.
Antibodies produced after vaccination are similar to natural antibodies but may differ in quantity and specificity. Vaccines often target key parts of a pathogen, leading to a focused immune response, whereas natural infection can trigger a broader antibody response.
Not always. The duration of antibody protection from vaccines varies depending on the vaccine and individual immune response. Some vaccines require boosters to maintain immunity, while natural infection may provide longer-lasting antibodies, though this is not guaranteed and can vary by pathogen.