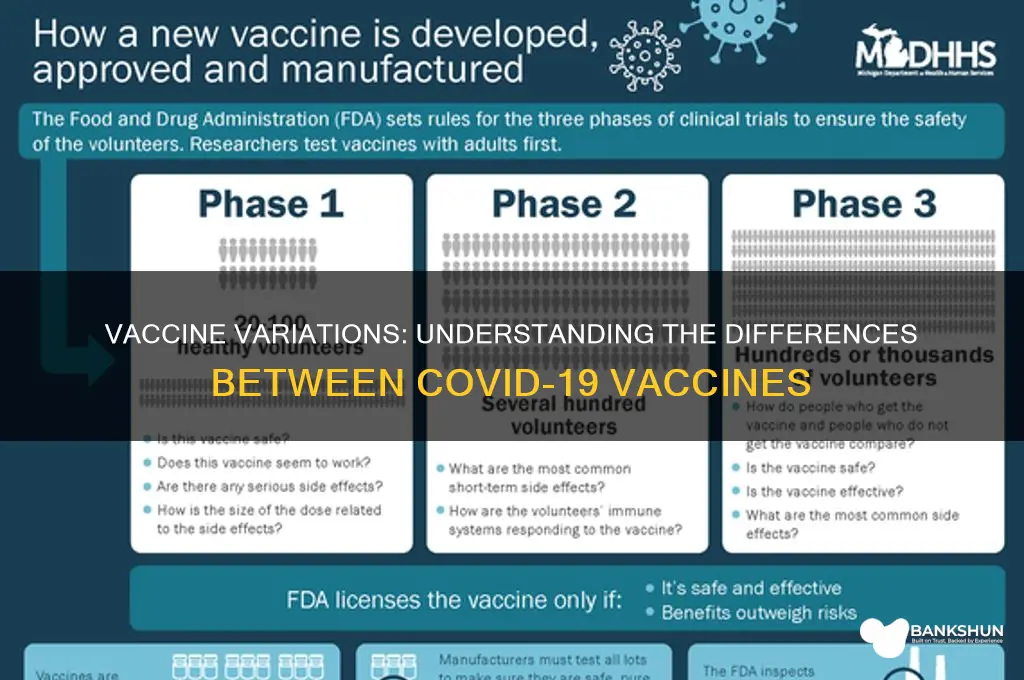
The question of whether there are differences between vaccines is a critical one, especially in the context of global health initiatives and immunization programs. Vaccines, while all designed to stimulate the immune system to protect against specific diseases, vary significantly in their composition, mechanisms of action, and efficacy. For instance, some vaccines, like mRNA vaccines (e.g., Pfizer-BioNTech and Moderna), use genetic material to instruct cells to produce a protein that triggers an immune response, whereas others, such as viral vector vaccines (e.g., AstraZeneca and Johnson & Johnson), employ a harmless virus to deliver genetic instructions. Additionally, traditional vaccines, like those for influenza or measles, often contain inactivated or weakened forms of the pathogen. These differences can influence factors such as storage requirements, dosing schedules, and side effect profiles, making it essential for healthcare providers and the public to understand the distinctions to ensure informed decision-making and optimal protection against diseases.
Explore related products






What You'll Learn
- Vaccine Types: mRNA, viral vector, protein subunit, and whole virus differences explained
- Efficacy Rates: Comparison of effectiveness against infection, severe illness, and hospitalization
- Side Effects: Common and rare side effects across different vaccine platforms
- Dosage & Schedule: Variations in number of doses and timing between vaccines
- Immunity Duration: How long protection lasts for each vaccine type
![]()
Vaccine Types: mRNA, viral vector, protein subunit, and whole virus differences explained
The COVID-19 pandemic spotlighted four primary vaccine technologies, each with distinct mechanisms and applications. Understanding these differences empowers informed decisions about vaccination. Let's dissect mRNA, viral vector, protein subunit, and whole virus vaccines.
MRNA Vaccines: The Instruction Manual
Imagine injecting your cells with a temporary recipe for a harmless viral protein fragment. That's the essence of mRNA vaccines like Pfizer-BioNTech and Moderna. These vaccines deliver genetic code (mRNA) encased in lipid nanoparticles. Cells use this code to produce the spike protein found on the virus's surface, triggering an immune response. This response includes antibody production and the activation of immune cells, preparing the body to recognize and combat the actual virus. Notably, mRNA doesn't alter your DNA. These vaccines boast high efficacy (around 95% initially) and require two doses, typically 3-4 weeks apart, for optimal protection.
Viral Vector Vaccines: The Trojan Horse Approach
Think of these vaccines as a clever disguise. Viral vector vaccines like AstraZeneca and Johnson & Johnson use a harmless, modified virus (the vector) to deliver genetic instructions for the spike protein. This vector acts as a Trojan horse, entering cells and prompting them to produce the protein, eliciting an immune response. While slightly less efficacious than mRNA vaccines (around 67-90% depending on the study), they offer advantages like easier storage and a single-dose regimen for Johnson & Johnson. However, rare blood clotting events have been associated with some viral vector vaccines, leading to specific recommendations for certain age groups.
Protein Subunit Vaccines: The Targeted Sniper
This approach focuses on delivering only the most crucial viral component: the spike protein itself. Protein subunit vaccines like Novavax isolate and purify this protein, often combined with an adjuvant to enhance the immune response. This method is well-established, having been used in vaccines for HPV and hepatitis B. While requiring two doses, protein subunit vaccines are generally well-tolerated and suitable for individuals with certain allergies or preferences for non-genetic vaccine technologies.
Whole Virus Vaccines: The Classic Approach
This traditional method uses either weakened (attenuated) or inactivated (killed) versions of the entire virus. Examples include the Sinopharm and Sinovac vaccines. Attenuated vaccines, like the measles vaccine, introduce a live but weakened virus, prompting a robust immune response. Inactivated vaccines, like the polio vaccine, use a killed virus, often requiring multiple doses and adjuvants to boost immunity. While effective, whole virus vaccines can pose a slight risk of reversion to virulence in attenuated forms and may be less suitable for immunocompromised individuals.
Choosing the Right Vaccine:
The "best" vaccine depends on individual factors like age, health status, and availability. Consult your healthcare provider for personalized advice. Remember, all approved vaccines significantly reduce the risk of severe illness, hospitalization, and death from COVID-19. Getting vaccinated, regardless of the type, is a crucial step in protecting yourself and your community.
Mastering the Bank Rush Challenge: Tips for Quick Completion
You may want to see also
Explore related products






![]()
Efficacy Rates: Comparison of effectiveness against infection, severe illness, and hospitalization
The COVID-19 vaccines have demonstrated varying efficacy rates, which are critical in understanding their impact on infection, severe illness, and hospitalization. For instance, the Pfizer-BioNTech vaccine has shown an initial efficacy of around 95% against symptomatic infection in clinical trials, while the Moderna vaccine closely follows with 94.1%. In contrast, the Johnson & Johnson (J&J) vaccine, a single-dose option, reported a lower efficacy of approximately 66% in preventing moderate to severe COVID-19 globally, though it still provided strong protection against hospitalization and death. These differences highlight the importance of considering specific vaccine characteristics when evaluating their effectiveness.
Analyzing the vaccines’ performance against severe illness and hospitalization reveals a more consistent picture. All authorized vaccines have proven highly effective in preventing severe outcomes, regardless of initial efficacy against infection. For example, real-world data from the CDC showed that mRNA vaccines (Pfizer and Moderna) were over 90% effective in preventing hospitalization among fully vaccinated adults. The J&J vaccine, despite its lower efficacy against infection, still demonstrated 71% effectiveness against hospitalization in the U.S. This suggests that while breakthrough infections may occur, vaccines remain a robust shield against critical illness.
Practical considerations for maximizing vaccine efficacy include adhering to recommended dosages and schedules. For Pfizer and Moderna, a two-dose regimen with a 3- to 4-week interval is standard, while a booster dose significantly enhances protection, particularly against variants like Delta and Omicron. The J&J vaccine’s single-dose convenience is appealing, but studies indicate that a second dose or a booster with an mRNA vaccine can improve its efficacy. Age also plays a role: individuals over 65 or with comorbidities may experience slightly lower efficacy, emphasizing the need for timely boosters and additional precautions.
A comparative analysis of efficacy rates underscores the trade-offs between vaccine types. mRNA vaccines offer higher initial protection against infection but require multiple doses and storage at ultra-cold temperatures, which can pose logistical challenges. The J&J vaccine, while less effective against infection, provides a practical single-dose option with easier storage requirements. For populations in areas with limited healthcare access or vaccine hesitancy, the J&J vaccine may be a more viable choice despite its lower efficacy. Ultimately, the best vaccine is the one that is available and accepted by the individual.
In conclusion, while efficacy rates against infection vary among COVID-19 vaccines, their effectiveness in preventing severe illness and hospitalization remains consistently high. Understanding these nuances allows individuals and healthcare providers to make informed decisions based on personal health needs, accessibility, and community context. Regularly updating vaccination status with boosters and staying informed about emerging data are essential steps in maintaining robust protection against the virus.
Huntington Bank in Colorado: Availability and Branch Locations Explained
You may want to see also
Explore related products

$14.95





![]()
Side Effects: Common and rare side effects across different vaccine platforms
Vaccines, regardless of platform, share a common goal: to train the immune system to recognize and combat pathogens. Yet, the path to immunity varies, and so do the side effects. mRNA vaccines, like Pfizer-BioNTech and Moderna, introduce genetic material that prompts cells to produce a harmless piece of the virus, triggering an immune response. Viral vector vaccines, such as AstraZeneca and Johnson & Johnson, use a modified virus to deliver genetic instructions. Protein subunit vaccines, like Novavax, contain harmless pieces of the virus directly. Each platform interacts with the body differently, leading to distinct side effect profiles.
Common side effects across all platforms include pain or swelling at the injection site, fatigue, headache, and muscle pain. These symptoms typically appear within 24–48 hours of vaccination and resolve within a few days. For instance, mRNA vaccines often cause more pronounced systemic reactions, especially after the second dose, due to their potent immune stimulation. Viral vector vaccines, on the other hand, may cause flu-like symptoms, such as fever and chills, in some recipients. Protein subunit vaccines generally have milder side effects, possibly because they contain only specific viral components rather than genetic material.
Rare side effects, though uncommon, highlight the importance of platform-specific awareness. mRNA vaccines have been associated with rare cases of myocarditis (heart inflammation), particularly in young males after the second dose. This risk is estimated at around 1 in 5,000 to 1 in 20,000 doses. Viral vector vaccines carry a small risk of thrombosis with thrombocytopenia syndrome (TTS), a blood clotting disorder, occurring in approximately 1 in 100,000 recipients. Protein subunit vaccines, being newer to the market, have limited data but have shown no significant safety concerns in clinical trials.
Practical tips can help manage side effects effectively. For common symptoms, over-the-counter pain relievers like acetaminophen or ibuprofen can alleviate discomfort, but avoid taking them preemptively unless advised by a healthcare provider. Stay hydrated and rest to support recovery. If rare side effects are suspected—such as chest pain, persistent headaches, or unusual bruising—seek medical attention immediately. Monitoring symptoms and reporting them through vaccine safety programs contributes to ongoing research and improves public health outcomes.
In conclusion, while all vaccines aim to protect against disease, their side effect profiles differ based on their mechanisms. Understanding these differences empowers individuals to make informed decisions and manage reactions effectively. Whether it’s the robust immune response of mRNA vaccines, the rare clotting risks of viral vectors, or the mild reactions of protein subunits, each platform offers a unique balance of benefits and potential drawbacks. Knowledge of these specifics ensures a safer and more confident vaccination experience.
Master HDFC NetBanking: A Step-by-Step Guide for Beginners
You may want to see also
Explore related products






![]()
Dosage & Schedule: Variations in number of doses and timing between vaccines
One of the most noticeable differences between COVID-19 vaccines is the number of doses required for full immunization. For instance, the Pfizer-BioNTech and Moderna vaccines both mandate a two-dose regimen for individuals aged 12 and older, with a recommended interval of 3 to 4 weeks between doses. In contrast, the Johnson & Johnson (Janssen) vaccine offers a single-dose option, providing a streamlined approach for those seeking quicker protection. This variation in dosage is not arbitrary; it stems from differences in vaccine technology and the immune response they elicit.
The timing of these doses is equally critical. For the Pfizer-BioNTech vaccine, the second dose should be administered 21 days after the first, while Moderna’s second dose is given 28 days later. These intervals are optimized to maximize immune response without overburdening the body. For younger age groups, such as children aged 5 to 11, Pfizer-BioNTech reduces the dosage to 10 micrograms per shot (compared to 30 micrograms for older individuals) and maintains a 21-day interval. This tailored approach ensures safety and efficacy across different demographics.
Booster shots further complicate the dosage and schedule landscape. While all three vaccines now recommend boosters, the timing and eligibility vary. Pfizer-BioNTech and Moderna boosters are advised 5 months after the initial series for adults, with a third primary dose for immunocompromised individuals 28 days after the second shot. Johnson & Johnson’s booster is recommended 2 months after the single dose. These differences highlight the importance of consulting healthcare providers to determine the appropriate schedule based on individual health status and vaccine availability.
Practical considerations also play a role in navigating these variations. For example, individuals who received the Johnson & Johnson vaccine initially may opt for a Pfizer or Moderna booster, as studies suggest this heterologous approach can enhance immunity. Conversely, those who started with an mRNA vaccine (Pfizer or Moderna) should stick to the same type for boosters unless contraindicated. Keeping track of vaccination dates and staying informed about updated guidelines is essential, especially as new variants emerge and recommendations evolve.
In summary, the dosage and schedule of COVID-19 vaccines are not one-size-fits-all. From single-dose convenience to multi-dose regimens, each vaccine’s design reflects its unique mechanism and target population. Understanding these differences empowers individuals to make informed decisions, ensuring timely and effective protection against the virus. Always consult healthcare professionals for personalized advice tailored to your specific needs.
The Federal Reserve: Government Entity or Independent Actor?
You may want to see also
Explore related products






![]()
Immunity Duration: How long protection lasts for each vaccine type
The duration of immunity provided by vaccines varies significantly depending on the type of vaccine, the pathogen it targets, and individual factors such as age and immune system health. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna, which have been widely used against COVID-19, offer robust protection for approximately 6 to 8 months after the initial two-dose series. However, this protection wanes over time, necessitating booster shots to maintain immunity. Studies show that a booster dose can restore efficacy to over 90% against severe disease and hospitalization. In contrast, viral vector vaccines like Johnson & Johnson provide a slightly shorter initial immunity period, typically around 5 to 6 months, but a single booster dose can significantly extend this protection.
Analyzing vaccine types further, inactivated or protein-based vaccines, such as those used for hepatitis B or the Novavax COVID-19 vaccine, often require multiple doses to build long-lasting immunity. For example, the hepatitis B vaccine series involves three doses over 6 months, providing protection that can last over 20 years in most individuals. Similarly, the Novavax COVID-19 vaccine, which uses a protein subunit approach, has shown durable immunity for at least 6 months post-vaccination, with ongoing studies to determine its long-term efficacy. These vaccines typically rely on traditional methods of inducing immune memory, which can result in more predictable and prolonged protection compared to newer technologies.
For live-attenuated vaccines, such as those for measles, mumps, and rubella (MMR), a single dose can provide lifelong immunity in 95% of recipients. However, a second dose is recommended to ensure protection in the remaining 5%. This high level of durability is due to the vaccine’s ability to mimic natural infection, stimulating a robust and long-lasting immune response. In contrast, vaccines targeting rapidly mutating viruses, like influenza, require annual updates and administrations because the virus evolves, reducing the effectiveness of previous immunity. This highlights the challenge of achieving long-term protection against certain pathogens.
Practical considerations for maintaining immunity include adhering to recommended booster schedules and staying informed about updated vaccine formulations. For example, individuals over 65 or those with compromised immune systems may require additional doses or more frequent boosters to sustain adequate protection. Additionally, combining different vaccine types (e.g., receiving an mRNA booster after a viral vector vaccine) has shown promising results in enhancing immunity, a strategy known as heterologous boosting. Always consult healthcare providers for personalized advice, as individual health conditions can influence vaccine effectiveness and duration.
In summary, the longevity of vaccine-induced immunity is not one-size-fits-all. It depends on the vaccine’s mechanism, the pathogen’s characteristics, and the individual’s immune response. While some vaccines offer decades of protection, others require regular boosters to remain effective. Understanding these differences empowers individuals to make informed decisions about their health and stay protected against preventable diseases.
The Risky Reality of Robbing a Bank: Is It Worth It?
You may want to see also
Frequently asked questions
Yes, while both Pfizer and Moderna are mRNA vaccines with high efficacy, they differ in storage requirements, dosing intervals, and minor variations in side effects. Pfizer requires ultra-cold storage initially, while Moderna can be stored at standard freezer temperatures.
The Johnson & Johnson vaccine is a viral vector vaccine, requiring only one dose, while Pfizer is an mRNA vaccine requiring two doses. J&J has a lower efficacy rate compared to Pfizer but offers easier distribution due to its single-dose regimen.
Yes, side effects vary by vaccine type. mRNA vaccines (Pfizer, Moderna) often cause more frequent and stronger reactions (e.g., fatigue, fever) after the second dose, while viral vector vaccines (J&J) may cause milder reactions but have rare risks like blood clots.
Yes, effectiveness against variants varies. mRNA vaccines (Pfizer, Moderna) generally show higher efficacy against variants like Delta and Omicron compared to viral vector vaccines (J&J, AstraZeneca), though all provide strong protection against severe illness and hospitalization.