The question of whether there is a vaccine for a specific virus is a critical one, as vaccines are one of the most effective tools in preventing and controlling infectious diseases. Vaccines work by training the immune system to recognize and combat pathogens, either by introducing a weakened or inactivated form of the virus or by using a fragment of it. While there are vaccines available for many well-known viruses, such as influenza, measles, and COVID-19, not all viruses have corresponding vaccines. The development of a vaccine depends on various factors, including the virus's complexity, its mutation rate, and the urgency of public health needs. Ongoing research and advancements in biotechnology continue to expand the list of vaccine-preventable diseases, offering hope for protection against emerging and existing viral threats.
| Characteristics | Values |
|---|---|
| Existence of Vaccines for Viruses | Yes, vaccines exist for numerous viruses. |
| Examples of Viral Vaccines | Measles, Mumps, Rubella (MMR), Influenza, COVID-19, Hepatitis A & B, Human Papillomavirus (HPV), Polio, Varicella (Chickenpox), Rabies, Ebola, Rotavirus, Yellow Fever. |
| Mechanism of Action | Stimulates the immune system to recognize and combat specific viral pathogens. |
| Types of Viral Vaccines | Live-attenuated, Inactivated, Subunit/Protein, mRNA, Viral vector. |
| Effectiveness | Varies by vaccine; some provide lifelong immunity (e.g., MMR), while others require periodic boosters (e.g., Influenza). |
| Global Impact | Eradicated smallpox; significantly reduced morbidity and mortality for diseases like polio and measles. |
| Challenges | Developing vaccines for rapidly mutating viruses (e.g., HIV, Influenza) remains difficult. |
| Recent Developments | mRNA technology (e.g., Pfizer-BioNTech, Moderna COVID-19 vaccines) has revolutionized vaccine development. |
| Availability | Varies by region; access is limited in low-income countries due to cost and distribution challenges. |
| Safety | Generally safe; rare side effects include allergic reactions or mild symptoms (e.g., fever, soreness). |
| Research Focus | Ongoing efforts to develop vaccines for HIV, RSV, Zika, and other emerging viruses. |
Explore related products

$11.93 $21.99
![Vaccines: Are They Really Safe and Effective? [VACCINES UPDATED AND REVIS -OS]](https://m.media-amazon.com/images/I/41yjhcd2-dL._AC_UY218_.jpg)




What You'll Learn
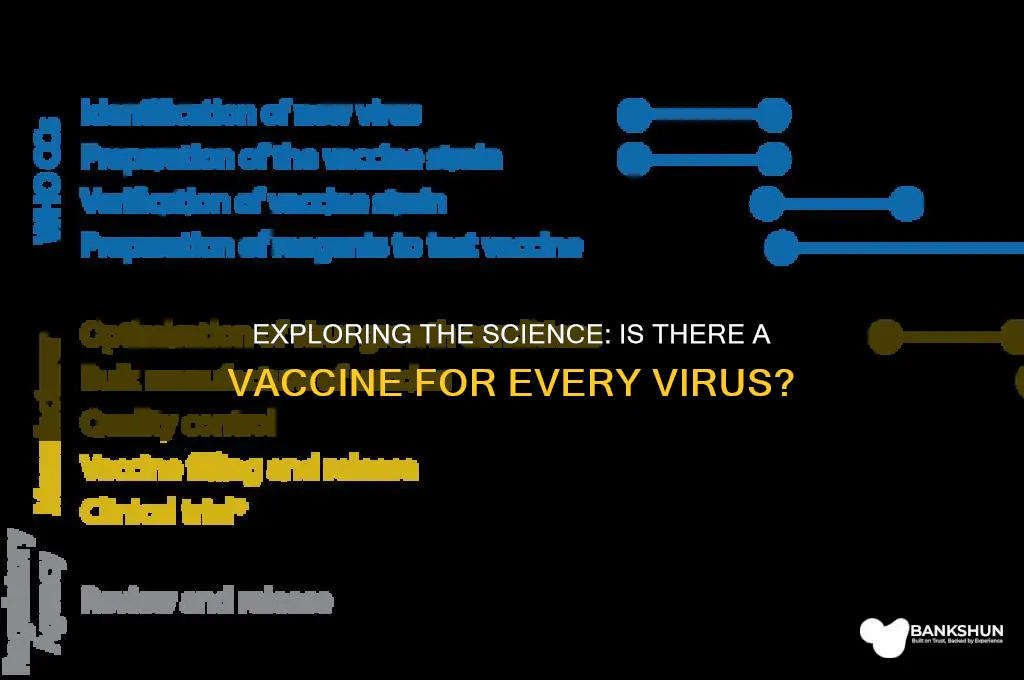
- Vaccine Development Process: Steps from virus identification to vaccine approval and distribution
- Vaccine Types: Live-attenuated, mRNA, viral vector, and protein subunit vaccines explained
- Efficacy and Safety: Clinical trials, effectiveness rates, and potential side effects of vaccines
- Global Access: Challenges in distributing vaccines equitably worldwide and affordability issues
- Vaccine Hesitancy: Causes, impacts, and strategies to address public skepticism about vaccines
![]()
Vaccine Development Process: Steps from virus identification to vaccine approval and distribution
Viruses, by their very nature, are elusive targets for medical intervention. Unlike bacteria, which can often be combated with antibiotics, viruses infiltrate host cells, making them difficult to attack without harming the host. This fundamental challenge underscores the complexity of vaccine development, a process that demands precision, patience, and rigorous scientific scrutiny.
From the moment a new virus is identified, the race to develop a vaccine begins. This journey, often spanning years, involves multiple stages, each critical to ensuring the safety and efficacy of the final product. The process begins with virus identification and characterization, where scientists isolate the virus, sequence its genome, and study its behavior in the human body. This foundational step is crucial for understanding how the virus causes disease and identifying potential targets for vaccine development.
Once the virus is characterized, researchers move to preclinical development, where potential vaccine candidates are designed and tested in laboratory settings. This phase often involves animal models to assess the vaccine’s safety and immunogenicity—its ability to provoke an immune response. For instance, mRNA vaccines, like those developed for COVID-19, were tested in mice and non-human primates before advancing to human trials. Dosage levels are carefully calibrated during this stage, typically starting with microgram quantities (e.g., 30 µg for the Pfizer-BioNTech COVID-19 vaccine) to balance efficacy and side effects.
The next step is clinical trials, a three-phase process that evaluates the vaccine in humans. Phase 1 trials focus on safety and dosage, involving a small group of healthy volunteers (20–100 participants). Phase 2 expands to several hundred subjects, assessing immunogenicity and refining dosage protocols. Phase 3 trials, the largest and most critical, involve thousands to tens of thousands of participants across diverse populations to confirm efficacy and monitor rare side effects. For example, the Moderna COVID-19 vaccine’s Phase 3 trial included 30,000 participants, with a two-dose regimen administered 28 days apart.
Following successful clinical trials, the vaccine undergoes regulatory review and approval. In the United States, the FDA scrutinizes all trial data to ensure the vaccine meets safety, quality, and efficacy standards. Emergency Use Authorization (EUA) can expedite this process during public health crises, as seen with COVID-19 vaccines. However, full approval requires additional long-term data, typically collected over months or years.
Finally, manufacturing and distribution begin, a logistical feat that involves scaling production, ensuring cold-chain storage (e.g., -70°C for Pfizer’s vaccine), and equitable global distribution. Practical tips for distribution include prioritizing high-risk groups (e.g., healthcare workers, the elderly) and leveraging local health systems to administer doses efficiently.
Each step in this process is a testament to human ingenuity and collaboration, transforming scientific discovery into life-saving vaccines. While the journey is long and fraught with challenges, it remains our most powerful tool in the fight against viral diseases.
TurboTax Bank Account Setup: A Step-by-Step Guide for Easy Filing
You may want to see also
Explore related products






![]()
Vaccine Types: Live-attenuated, mRNA, viral vector, and protein subunit vaccines explained
Vaccines are not one-size-fits-all. Each type harnesses a distinct mechanism to train the immune system, offering protection against viruses with varying levels of efficacy and safety profiles. Understanding these differences is crucial for informed decision-making, especially as new vaccine technologies emerge.
Live-attenuated vaccines, like the measles, mumps, and rubella (MMR) vaccine, use a weakened form of the virus, incapable of causing severe disease but still potent enough to trigger a robust immune response. This approach mimics natural infection, often providing lifelong immunity after a single dose. However, individuals with compromised immune systems should avoid these vaccines due to the theoretical risk of the virus reverting to its virulent form.
MRNA vaccines, exemplified by the Pfizer-BioNTech and Moderna COVID-19 vaccines, represent a revolutionary approach. They deliver genetic instructions to our cells, prompting them to produce a harmless piece of the virus, typically a protein found on its surface. This protein stimulates the immune system to generate antibodies and immune cells, preparing it for a real encounter with the virus. mRNA vaccines are highly effective, often requiring two doses spaced several weeks apart, and offer a safer alternative for immunocompromised individuals compared to live-attenuated vaccines.
Viral vector vaccines, such as the Johnson & Johnson COVID-19 vaccine, utilize a harmless virus (the vector) to deliver genetic material encoding a viral protein into our cells. This protein triggers an immune response similar to mRNA vaccines. While slightly less effective than mRNA vaccines in some cases, they offer the advantage of a single-dose regimen and can be stored at standard refrigerator temperatures, making them more accessible in resource-limited settings.
Protein subunit vaccines, like the Novavax COVID-19 vaccine, take a more direct approach. They contain only a specific piece of the virus, usually a protein, that is known to elicit a strong immune response. This purified protein is often combined with an adjuvant, a substance that enhances the immune response. Protein subunit vaccines are generally very safe, even for those with compromised immune systems, but may require multiple doses to achieve optimal protection.
Wells Fargo's Missteps: Uncovering the Bank's Ethical and Legal Failures
You may want to see also
Explore related products






![]()
Efficacy and Safety: Clinical trials, effectiveness rates, and potential side effects of vaccines
Vaccines undergo rigorous clinical trials to ensure they meet stringent efficacy and safety standards before approval. These trials typically progress through three phases, each designed to evaluate different aspects of the vaccine. Phase 1 focuses on safety, testing the vaccine on a small group of healthy volunteers to identify potential side effects and determine dosage levels. Phase 2 expands the study to include several hundred participants, assessing the vaccine’s immunogenicity (its ability to provoke an immune response) and further refining safety data. Phase 3 involves thousands of participants and aims to confirm the vaccine’s effectiveness in preventing disease, while continuing to monitor safety in a larger, more diverse population. For example, the Pfizer-BioNTech COVID-19 vaccine’s Phase 3 trial included over 43,000 participants, demonstrating 95% efficacy in preventing symptomatic infection.
Effectiveness rates are a critical measure of a vaccine’s performance in real-world settings. These rates indicate the percentage of vaccinated individuals who are protected from the disease. For instance, the measles vaccine boasts an effectiveness rate of 97% after two doses, making it one of the most successful vaccines in history. However, effectiveness can vary based on factors like age, underlying health conditions, and the virus’s ability to mutate. Booster doses are often recommended to maintain immunity, as seen with the annual flu vaccine, which typically has an effectiveness rate of 40–60% due to the virus’s rapid evolution. Understanding these rates helps individuals and healthcare providers make informed decisions about vaccination.
While vaccines are generally safe, potential side effects are an important consideration. Common side effects include soreness at the injection site, mild fever, fatigue, and headaches, which usually resolve within a few days. For example, the Moderna COVID-19 vaccine may cause more pronounced side effects after the second dose, such as muscle pain and chills, but these are typically short-lived and manageable with over-the-counter pain relievers. Rare but serious side effects, such as anaphylaxis, occur in approximately 1 in 500,000 to 1 million doses and are why individuals are monitored for 15–30 minutes after vaccination. Transparency about these risks builds public trust and ensures that individuals can weigh the benefits against potential drawbacks.
Practical tips can enhance the vaccination experience and minimize discomfort. Scheduling vaccinations during a time when you can rest afterward is advisable, especially for vaccines known to cause fatigue. Staying hydrated and wearing loose clothing can also improve comfort. For children, distractions like toys or stories during the injection can reduce anxiety. It’s crucial to follow dosage instructions carefully; for instance, the HPV vaccine is administered in two or three doses depending on the recipient’s age, with intervals of 6–12 months between doses. Adhering to these guidelines maximizes the vaccine’s efficacy and ensures optimal protection.
Ultimately, the balance between efficacy and safety is a cornerstone of vaccine development and administration. Clinical trials provide robust evidence of a vaccine’s ability to prevent disease while identifying potential risks. Effectiveness rates offer real-world context, guiding expectations and informing public health strategies. By understanding side effects and following practical advice, individuals can approach vaccination with confidence. Vaccines remain one of the most powerful tools in modern medicine, and their careful evaluation ensures they protect without compromising safety.
Exploring Florida's Banking Landscape: Regions Bank's Presence Across the State
You may want to see also
Explore related products






![]()
Global Access: Challenges in distributing vaccines equitably worldwide and affordability issues
The COVID-19 pandemic starkly highlighted the inequities in global vaccine distribution. While wealthy nations secured billions of doses, low-income countries struggled to access even a fraction. For instance, as of late 2021, over 80% of COVID-19 vaccines had gone to high- and upper-middle-income countries, leaving many African nations with vaccination rates below 10%. This disparity isn’t unique to COVID-19; it’s a recurring pattern in global health crises. The question isn’t just about whether vaccines exist, but who can access them and at what cost.
One of the primary challenges in equitable distribution is logistics. Vaccines like Pfizer’s mRNA COVID-19 vaccine require ultra-cold storage at -70°C, a standard impossible to meet in many low-resource settings. Even vaccines with less stringent requirements, such as AstraZeneca’s, face hurdles in transportation and storage. For example, a single dose of the AstraZeneca vaccine must be administered within 6 hours of opening the vial, demanding precise coordination in remote areas. Without robust infrastructure, even available vaccines remain out of reach for millions.
Affordability compounds these logistical challenges. While initiatives like COVAX aimed to provide vaccines to low-income countries, they faced funding shortfalls and supply chain disruptions. Wealthy nations often outbid global initiatives, securing doses at higher prices. For instance, the cost of a single dose of the Moderna vaccine was approximately $15–$25 in the U.S., compared to $7 per dose through COVAX. For countries with limited healthcare budgets, these price differences are insurmountable, leaving populations vulnerable to outbreaks.
Intellectual property rights further exacerbate inequities. Pharmaceutical companies hold patents on vaccine technologies, restricting production to a handful of manufacturers. This monopoly limits supply and drives up costs. The World Trade Organization’s proposal to waive vaccine patents faced resistance from wealthy nations, delaying potential solutions. Without a shift in global policies, low-income countries will continue to rely on donations and limited production capacities, perpetuating cycles of inaccessibility.
To address these challenges, a multi-faceted approach is essential. First, invest in local manufacturing capabilities in low-income regions to reduce dependency on imports. Second, streamline regulatory approvals for vaccines produced in non-traditional markets. Third, establish fair pricing mechanisms that prioritize global health over profit. Finally, strengthen global partnerships to ensure equitable distribution during future pandemics. Without these steps, the promise of vaccines will remain a distant reality for billions, undermining global health security.
When Do Banks Process Payments?
You may want to see also
Explore related products






![]()
Vaccine Hesitancy: Causes, impacts, and strategies to address public skepticism about vaccines
Vaccine hesitancy, defined by the World Health Organization as the delay in acceptance or refusal of vaccines despite availability, has become a critical public health challenge. While vaccines have eradicated diseases like smallpox and controlled others such as polio, measles outbreaks in recent years highlight the consequences of declining vaccination rates. For instance, the measles vaccine is 97% effective with two doses, yet in 2019, the U.S. reported its highest number of cases in decades, largely among unvaccinated populations. This trend underscores the urgency of understanding why skepticism persists and how to address it effectively.
The roots of vaccine hesitancy are multifaceted, often stemming from misinformation, historical mistrust, and individual risk perception. Social media platforms amplify false claims, such as the debunked link between the MMR vaccine and autism, which persists in public consciousness. Additionally, marginalized communities may harbor justified skepticism due to past medical exploitation, like the Tuskegee Syphilis Study. Psychological factors also play a role; some individuals overestimate their immunity or underestimate disease severity, leading to complacency. For example, during the COVID-19 pandemic, surveys revealed that 20-30% of respondents in various countries expressed reluctance to receive a vaccine, citing concerns about side effects or rushed development.
The impacts of vaccine hesitancy extend beyond individual health, threatening herd immunity and increasing healthcare costs. When vaccination rates drop below 95%, as seen in some U.S. communities, diseases like measles can spread rapidly, endangering immunocompromised individuals who cannot receive vaccines. Economically, outbreaks strain healthcare systems; the 2019 measles outbreak cost the U.S. an estimated $200 million in treatment and containment efforts. Globally, hesitancy hinders efforts to eradicate diseases like polio, where just a handful of cases in under-vaccinated regions can reignite outbreaks.
Addressing vaccine hesitancy requires tailored strategies that build trust and counter misinformation. Healthcare providers play a pivotal role; a 2020 study found that 70% of hesitant individuals were more likely to vaccinate after discussions with trusted doctors. Public health campaigns should focus on clear, evidence-based messaging, avoiding jargon and addressing specific concerns. For instance, emphasizing that COVID-19 vaccines underwent rigorous testing, with over 70,000 participants in clinical trials, can alleviate fears of rushed development. Community-based initiatives, such as town halls or partnerships with local leaders, can bridge cultural and historical gaps, particularly in marginalized populations.
Ultimately, combating vaccine hesitancy demands a collaborative approach that respects individual concerns while prioritizing collective well-being. Policymakers must invest in health literacy programs and regulate misinformation on digital platforms. Schools can integrate vaccine education into curricula, fostering informed decision-making from a young age. By combining empathy, evidence, and engagement, societies can rebuild trust in vaccines and safeguard public health for generations to come.
Banks as White Spaces: Unlocking Untapped Potential in Financial Services
You may want to see also
Frequently asked questions
No, there is not a vaccine for every virus. Vaccines are developed based on the specific characteristics of a virus, its impact on human health, and the feasibility of creating an effective and safe vaccine.
Developing a vaccine typically takes several years, but in emergencies like the COVID-19 pandemic, this process can be expedited to 12–18 months with accelerated research, funding, and regulatory approvals.
Vaccines are generally designed to target specific strains or variants of a virus. While they may offer some protection against related variants, effectiveness can decrease if the virus mutates significantly.
Vaccines primarily reduce the severity of illness, hospitalization, and death, but they may not always prevent infection entirely. Some vaccinated individuals can still get infected, especially with highly transmissible variants.
Viruses are highly diverse, and their structures and behaviors vary widely. A universal vaccine would need to target common mechanisms across all viruses, which is extremely challenging due to their complexity and rapid mutation rates.