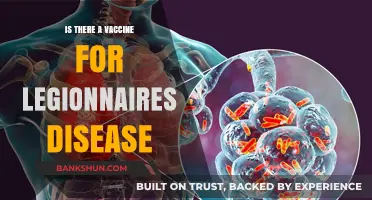
Japanese encephalitis (JE) is a potentially severe viral infection transmitted by mosquitoes, primarily in Asia and parts of the Western Pacific. It affects the brain and can lead to long-term neurological complications or even death. Given its significant health impact, the question of whether there is a vaccine for Japanese encephalitis is of great importance. Fortunately, several effective vaccines are available to prevent JE, offering protection to both travelers and residents in endemic regions. These vaccines are recommended for individuals at risk, particularly those living in or visiting areas with high transmission rates, and have played a crucial role in reducing the disease's prevalence.
Explore related products


$99 $109.99




What You'll Learn
- Vaccine Availability: Japanese encephalitis vaccines are available in many countries, including endemic regions
- Vaccine Types: Two main types exist: inactivated (IXIARO) and live-attenuated (SA14-14-2)
- Target Groups: Travelers, residents in endemic areas, and lab workers are recommended for vaccination
- Dosage Schedule: Typically a 2-dose series, with boosters every 1-3 years for high-risk groups
- Effectiveness: Provides up to 90% protection, significantly reducing the risk of severe disease
![]()
Vaccine Availability: Japanese encephalitis vaccines are available in many countries, including endemic regions
Japanese encephalitis (JE) vaccines are widely accessible across the globe, including in regions where the disease is endemic. This availability is a critical factor in preventing the spread of this potentially fatal virus, primarily transmitted through mosquito bites. Countries in Asia and the western Pacific, where JE is most prevalent, have integrated these vaccines into their national immunization programs, ensuring that at-risk populations, particularly children, are protected. For instance, in countries like India, Thailand, and South Korea, JE vaccines are routinely administered to infants and young children, typically in a two-dose schedule starting as early as 9 months of age. This proactive approach has significantly reduced the incidence of JE in these areas, highlighting the importance of vaccine accessibility in disease control.
For travelers visiting JE-endemic regions, obtaining the vaccine is a practical and often recommended precaution. The Centers for Disease Control and Prevention (CDC) advises that travelers to rural areas in Asia, especially during peak mosquito seasons, should consider vaccination. The vaccine, available under brand names such as IXIARO (in the U.S.) and JESPECT (in Europe), is administered in a two-dose series, with the second dose given 28 days after the first. A single booster dose may be required after 12–24 months for those at continued risk. It’s essential to plan ahead, as the vaccination process should ideally be completed at least a week before travel to ensure adequate immunity.
Despite the vaccine’s availability, challenges remain in ensuring equitable access, particularly in low-resource settings. Cost and distribution logistics can hinder widespread vaccination efforts, leaving vulnerable populations at risk. However, initiatives like the World Health Organization’s (WHO) support for vaccine introduction and Gavi, the Vaccine Alliance’s funding for low-income countries, have made significant strides in bridging these gaps. For example, in countries like Nepal and Cambodia, mass vaccination campaigns have been successful in reaching remote communities, demonstrating that with targeted efforts, vaccine availability can be maximized even in challenging environments.
Practical tips for individuals seeking JE vaccination include consulting a healthcare provider or travel clinic well in advance of travel to assess risk and schedule doses. It’s also important to be aware of potential side effects, which are generally mild and may include headache, muscle pain, or soreness at the injection site. While rare, severe allergic reactions can occur, so vaccination should be administered in a setting where medical care is readily available. By understanding the availability and logistics of JE vaccines, individuals and communities can take proactive steps to protect themselves from this preventable disease.
Citizens Bank App: Mobile Banking Features and Accessibility Explained
You may want to see also
Explore related products






![]()
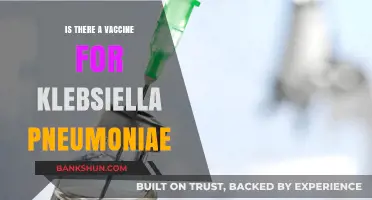
Vaccine Types: Two main types exist: inactivated (IXIARO) and live-attenuated (SA14-14-2)
Japanese encephalitis, a viral infection transmitted by mosquitoes, poses a significant health risk in many parts of Asia and the Pacific. Fortunately, vaccines are available to prevent this potentially severe disease. Two primary types of vaccines dominate the market: inactivated (IXIARO) and live-attenuated (SA14-14-2). Understanding their differences is crucial for informed decision-making, especially for travelers and residents in endemic areas.
Analytical Perspective:
The inactivated vaccine, IXIARO (approved in the U.S. and Europe), is derived from a purified, chemically inactivated virus. This formulation ensures it cannot replicate in the body, making it safer for individuals with weakened immune systems. Administered in a two-dose series, typically 28 days apart, it offers robust protection for adults and children over 2 months old. Studies show efficacy rates exceeding 90%, with a third dose recommended for long-term travelers or those at continued risk. In contrast, the live-attenuated vaccine, SA14-14-2 (widely used in China and other Asian countries), contains a weakened but live virus. While highly effective after a single dose, it is generally restricted to individuals aged 8 months to 60 years and may pose risks for immunocompromised individuals.
Instructive Approach:
For optimal protection, consider your age, health status, and travel plans when choosing a vaccine. IXIARO is ideal for young children, older adults, or those with compromised immunity due to its inactivated nature. The first dose should be administered at least 7 days before potential exposure, with the second dose following 28 days later. If time is limited, SA14-14-2 offers a single-dose convenience but is not suitable for everyone. Always consult a healthcare provider to determine the best option for your specific needs.
Comparative Insight:
While both vaccines are effective, their administration and eligibility criteria differ significantly. IXIARO’s inactivated formulation minimizes adverse reactions, typically limited to mild pain at the injection site. SA14-14-2, however, may cause transient fever or rash in some recipients due to its live virus component. Cost and availability also vary; IXIARO is more expensive and primarily accessible in Western countries, whereas SA14-14-2 is more affordable and widely distributed in endemic regions.
Practical Tips:
Regardless of the vaccine chosen, combine immunization with mosquito avoidance strategies for comprehensive protection. Wear long sleeves, use DEET-based repellents, and sleep under mosquito nets in high-risk areas. Keep vaccination records handy, especially when traveling, as proof of immunization may be required in certain regions. For those receiving IXIARO, schedule doses well in advance of travel to ensure full immunity. If opting for SA14-14-2, verify its suitability with a healthcare professional, particularly if you have underlying health conditions.
Takeaway:
Both inactivated (IXIARO) and live-attenuated (SA14-14-2) vaccines are effective tools against Japanese encephalitis, but their distinct characteristics cater to different populations and circumstances. By weighing factors like age, health, and travel plans, individuals can select the most appropriate vaccine and take proactive steps to safeguard their health in endemic areas.
Mastering Bank Valuation: Key Strategies for Accurate Financial Assessment
You may want to see also
Explore related products






![]()
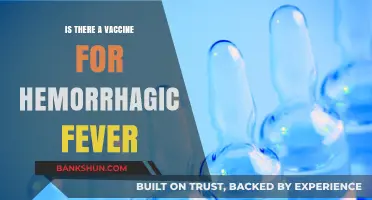
Target Groups: Travelers, residents in endemic areas, and lab workers are recommended for vaccination
Japanese encephalitis (JE) vaccination is not a one-size-fits-all recommendation. While the disease is rare, its severe neurological complications make targeted prevention crucial. Travelers venturing into endemic regions in Asia and the western Pacific face a heightened risk, particularly during peak mosquito seasons. Rural areas with rice paddies and pig farming—ideal breeding grounds for the Culex mosquitoes that transmit the virus—pose the greatest threat. For these travelers, a two-dose series of the Ixiaro vaccine, administered 28 days apart, is standard, with an accelerated 7-day schedule available for last-minute trips. Notably, the CDC advises vaccination for those spending a month or more in endemic zones, especially if travel includes rural areas or outdoor activities during evenings and nights.
Residents of endemic areas, particularly children, bear the brunt of JE’s impact. In countries like India, China, and Thailand, national immunization programs target infants and young children, typically starting at 9 months of age. The live-attenuated SA14-14-2 vaccine, widely used in these regions, requires a primary series of one to three doses, followed by boosters every 1–3 years. Despite its effectiveness, vaccine hesitancy and accessibility issues persist, leaving gaps in community protection. For adults in endemic regions, vaccination is often overlooked, yet outbreaks in older age groups highlight the need for broader coverage, especially in areas with declining herd immunity.
Laboratory workers handling the Japanese encephalitis virus face a unique occupational hazard. Accidental exposure through needle sticks or aerosolized virus in research settings can lead to infection, even without mosquito transmission. For these individuals, vaccination is not just recommended—it’s essential. The CDC’s Advisory Committee on Immunization Practices (ACIP) mandates that lab personnel receive the inactivated vaccine series, regardless of travel history or endemic residence. This group also requires regular serological testing to ensure immunity, as workplace exposure risks are ongoing.
Comparing these target groups reveals a spectrum of risk and prevention strategies. Travelers rely on pre-trip vaccinations and mosquito avoidance, while residents in endemic areas depend on sustained public health initiatives. Lab workers, meanwhile, benefit from occupational health protocols tailored to their specific risks. Across all groups, the vaccines’ safety profiles are well-established, with mild side effects like pain at the injection site or low-grade fever. However, cost and accessibility remain barriers, particularly for travelers in non-endemic countries, where the vaccine is often not covered by standard insurance plans.
In practice, tailoring vaccination strategies to these groups requires collaboration between healthcare providers, public health agencies, and employers. For travelers, clinics should emphasize the importance of timely vaccination and provide region-specific risk assessments. Endemic countries must prioritize vaccine distribution to rural areas and address misinformation to boost uptake. Lab facilities should integrate vaccination into mandatory safety training and provide resources for post-exposure management. By focusing on these distinct populations, global efforts to combat Japanese encephalitis can maximize protection where it’s needed most.
Is 'Branch' Capitalized When Referring to a Bank? Grammar Guide
You may want to see also
Explore related products






![]()
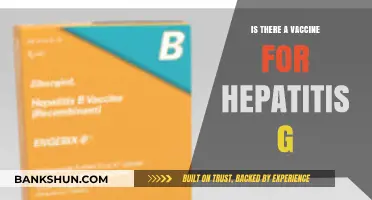
Dosage Schedule: Typically a 2-dose series, with boosters every 1-3 years for high-risk groups
Japanese encephalitis (JE) vaccination follows a precise dosage schedule to ensure optimal protection, particularly for those at heightened risk. The primary series consists of two doses, typically administered 28 days apart. This initial regimen is crucial for building a robust immune response against the virus. For adults and children over the age of 2 months, the standard dose is 0.5 mL per injection, delivered intramuscularly into the deltoid muscle for adults and the anterolateral thigh for young children. Adhering to this schedule is essential, as it maximizes the vaccine’s efficacy in preventing severe disease.
Booster doses play a critical role in maintaining long-term immunity, especially for individuals in high-risk groups. These include travelers to endemic areas, laboratory workers handling the virus, and residents of regions with frequent JE outbreaks. Boosters are recommended every 1 to 3 years, depending on ongoing exposure risk and the specific vaccine used. For example, the Ixiaro vaccine, commonly used in the U.S. and Europe, requires a booster after 12 to 18 months for continued protection. Practical tips for high-risk individuals include scheduling boosters well in advance of travel and keeping a vaccination record to track due dates.
Age-specific considerations are vital when planning the JE vaccination schedule. Children under 2 months are not eligible for the vaccine, while those aged 2 months to 3 years may require a reduced dose or an adjusted schedule. For older children and adolescents, the standard adult regimen applies. Pregnant or breastfeeding women should consult a healthcare provider, as the vaccine is generally avoided unless the risk of infection is high. Tailoring the dosage schedule to age and health status ensures both safety and effectiveness.
Comparing the JE vaccination schedule to other travel vaccines highlights its unique requirements. Unlike vaccines such as hepatitis A, which may offer protection for decades, JE immunity wanes more rapidly, necessitating frequent boosters. This underscores the importance of staying informed about local disease activity and personal risk factors. For instance, a traveler visiting rural areas during peak mosquito season may need a booster sooner than someone staying in urban centers. Understanding these nuances empowers individuals to make informed decisions about their vaccination needs.
In conclusion, the JE vaccine’s dosage schedule is a carefully designed regimen that balances initial immunity with long-term protection. By following the 2-dose series and adhering to booster recommendations, high-risk individuals can significantly reduce their risk of contracting this potentially fatal disease. Practical planning, age-specific adjustments, and awareness of regional risks are key to maximizing the vaccine’s benefits. Whether for travel, occupation, or residence in endemic areas, staying current with the JE vaccination schedule is a critical step in safeguarding health.
Vaccine Passports and HIPAA: Privacy Concerns Explored
You may want to see also
Explore related products






![]()
Effectiveness: Provides up to 90% protection, significantly reducing the risk of severe disease
Japanese encephalitis (JE) is a viral infection transmitted by mosquitoes, primarily in Asia and parts of the Western Pacific. While the disease is rare, its potential for severe neurological complications makes prevention critical. The JE vaccine stands out as a highly effective tool in this effort, offering up to 90% protection against the virus. This level of efficacy significantly reduces the risk of severe disease, including encephalitis, which can lead to long-term disability or death. For travelers and residents in endemic areas, this vaccine is a cornerstone of public health strategy, providing a reliable shield against a potentially devastating illness.
Analyzing the vaccine’s effectiveness, the 90% protection rate is particularly impressive when compared to other travel-related vaccines. For instance, the influenza vaccine typically ranges between 40-60% effectiveness depending on the season. The JE vaccine’s high efficacy is attributed to its robust immunogenicity, often achieved after a two-dose series for most formulations. The Ixiaro and Imojev vaccines, commonly used globally, are administered in two doses spaced 28 days apart, with studies showing seroprotection in over 90% of recipients. For those with limited time before travel, an accelerated schedule (0 and 7 days) is available, though it may offer slightly lower protection. This flexibility ensures that individuals can still benefit from substantial immunity even under urgent circumstances.
From a practical standpoint, understanding who should receive the JE vaccine is crucial. It is recommended for travelers spending a month or more in endemic areas, particularly rural or agricultural regions where mosquito exposure is higher. Expatriates, missionaries, and military personnel are also advised to get vaccinated. Age-specific guidelines vary: Ixiaro is approved for individuals aged 2 months and older, while Imojev is licensed for those 18 years and above. Pregnant women and those with severe allergies to vaccine components should consult a healthcare provider before vaccination. Notably, the vaccine’s high effectiveness means that even in areas with high JE transmission, the risk of contracting the disease post-vaccination is minimal.
Persuasively, the JE vaccine’s 90% protection rate should alleviate concerns about the disease’s severity. Encephalitis, the most feared complication, occurs in less than 1% of JE infections but carries a fatality rate of 20-30% and long-term disability in 30-50% of survivors. By significantly reducing the likelihood of severe disease, the vaccine not only protects individuals but also contributes to herd immunity in endemic communities. Its effectiveness is further bolstered by its safety profile, with mild side effects such as pain at the injection site or headache reported in less than 10% of recipients. This balance of high efficacy and low risk makes it a compelling choice for anyone at risk of exposure.
In conclusion, the JE vaccine’s up-to-90% protection rate is a testament to its role as a vital preventive measure. Its ability to significantly reduce the risk of severe disease underscores its importance for travelers and residents in endemic areas alike. By adhering to recommended dosages and schedules, individuals can maximize their immunity and minimize their vulnerability to this dangerous virus. Whether planning a trip to rural Asia or residing in a high-risk zone, the JE vaccine offers peace of mind backed by robust scientific evidence. Its effectiveness is not just a statistic—it’s a lifeline against a preventable threat.
Overdraft Fees: Banks' Right or Wrong?
You may want to see also
Frequently asked questions
Yes, there are vaccines available to prevent Japanese encephalitis, a viral infection transmitted by infected mosquitoes.
The vaccine is recommended for travelers visiting endemic areas in Asia and the Western Pacific for extended periods, as well as for residents of those regions.
The number of doses varies by vaccine type, but typically a primary series of 2–3 doses is given, followed by boosters every 1–3 years for continued protection.
Common side effects include mild pain at the injection site, headache, muscle pain, and fatigue. Serious side effects are rare.
Yes, the vaccine is approved for use in children as young as 2 months old, depending on the specific vaccine formulation.