Ebola Virus Disease (EVD), a severe and often fatal illness caused by the Ebola virus, has sparked significant global concern due to its high mortality rate and potential for rapid spread. Historically, outbreaks have been particularly devastating in parts of Africa, prompting urgent efforts to develop preventive measures. One of the most critical questions in the fight against Ebola is whether there exists a vaccine to prevent the disease. Recent advancements in medical research have indeed led to the development and approval of vaccines, such as Ervebo (rVSV-ZEBOV), which has shown high efficacy in clinical trials and real-world settings. These breakthroughs offer hope for controlling future outbreaks and protecting vulnerable populations, though challenges remain in ensuring widespread access and distribution in affected regions.
| Characteristics | Values |
|---|---|
| Vaccine Availability | Yes, there are approved vaccines to prevent Ebola. |
| Approved Vaccines | Ervebo (rVSV-ZEBOV) and Zabdeno/Mvabea (Ad26.ZEBOV and MVA-BN-Filo). |
| Ervebo (rVSV-ZEBOV) | Approved by the FDA in 2019 and WHO prequalified in 2019. |
| Zabdeno/Mvabea | Approved by the European Commission in 2020. |
| Efficacy | Ervebo showed 100% efficacy in a ring vaccination trial in Guinea. |
| Target Population | Adults and children above 1 year of age. |
| Dosage | Ervebo: Single dose; Zabdeno/Mvabea: Two-dose regimen (prime-boost). |
| Storage Requirements | Ervebo: -60°C to -80°C; Zabdeno/Mvabea: Standard refrigeration (2-8°C). |
| Usage in Outbreaks | Widely used in recent Ebola outbreaks in Africa (e.g., DRC, 2018-2020). |
| Side Effects | Mild to moderate, including headache, fatigue, and muscle pain. |
| Global Access | Supported by Gavi, the Vaccine Alliance, for low-income countries. |
| Ongoing Research | Continued studies for long-term efficacy and pediatric use. |
Explore related products






What You'll Learn
![]()
Current Ebola vaccine availability
As of recent developments, the Ervebo vaccine, developed by Merck, has been a game-changer in the fight against Ebola. Approved by the U.S. Food and Drug Administration (FDA) in 2019 and prequalified by the World Health Organization (WHO) in 2019, it is the first and only vaccine licensed for preventing Ebola virus disease (EVD) caused by the Zaire ebolavirus species. This single-dose vaccine has been administered to over 350,000 individuals in various outbreak settings, demonstrating a high level of efficacy in protecting against this deadly disease.
From a practical standpoint, the Ervebo vaccine is typically given as a single 1-milliliter injection into the deltoid muscle of individuals aged 18 years and older. In outbreak situations, the WHO has also recommended a "ring vaccination" strategy, where contacts and contacts of contacts of confirmed Ebola cases are vaccinated to create a protective barrier around the infected individual. This approach has proven effective in limiting the spread of the virus, as evidenced by its successful implementation during the 2018-2020 Ebola outbreak in the Democratic Republic of Congo (DRC). It is essential to note that the vaccine should not be administered to individuals with a history of severe allergic reactions to any component of the vaccine.
A comparative analysis of Ebola vaccine development reveals that while Ervebo is currently the only licensed vaccine, other candidates are in various stages of clinical trials. For instance, the Johnson & Johnson (J&J) regimen, which consists of two doses administered 56 days apart, has shown promising results in phase 2 and 3 trials. This vaccine uses a non-replicating viral vector based on adenovirus serotype 26 (Ad26) to deliver genetic material encoding the Ebola glycoprotein. Although not yet licensed, the J&J vaccine has been used in a clinical trial setting during the 2018-2020 DRC outbreak, providing valuable data on its safety and efficacy. The availability of multiple vaccine options in the future could enhance global preparedness and response to Ebola outbreaks.
In terms of accessibility, the Ervebo vaccine has been made available through a global emergency stockpile, which was established in 2020 to ensure rapid response to Ebola outbreaks. This stockpile, managed by the International Coordinating Group (ICG) on Vaccine Provision, consists of 6,000 doses of the vaccine, which can be deployed within 24-72 hours of a request from a country experiencing an outbreak. To date, the stockpile has been utilized in several countries, including Guinea, the DRC, and Côte d'Ivoire, highlighting the importance of global collaboration in combating Ebola. Individuals traveling to or residing in Ebola-affected areas should consult with healthcare professionals or local health authorities to determine their eligibility for vaccination and receive guidance on preventive measures.
Despite the progress made in Ebola vaccine development, challenges remain in ensuring widespread availability and accessibility, particularly in low-resource settings. Cold chain requirements, which necessitate storage and transportation of the vaccine at temperatures between -60°C and -80°C, pose significant logistical hurdles. Moreover, the high cost of production and distribution can limit access for vulnerable populations. To address these challenges, ongoing research is focused on developing thermostable vaccine formulations and exploring alternative delivery methods, such as oral or intranasal administration. By overcoming these barriers, we can move closer to a world where Ebola vaccines are readily available to those who need them most, ultimately contributing to the global goal of eliminating Ebola as a public health threat.
Step-by-Step Guide to Investing in Yes Bank's IPO Successfully
You may want to see also
Explore related products






![]()
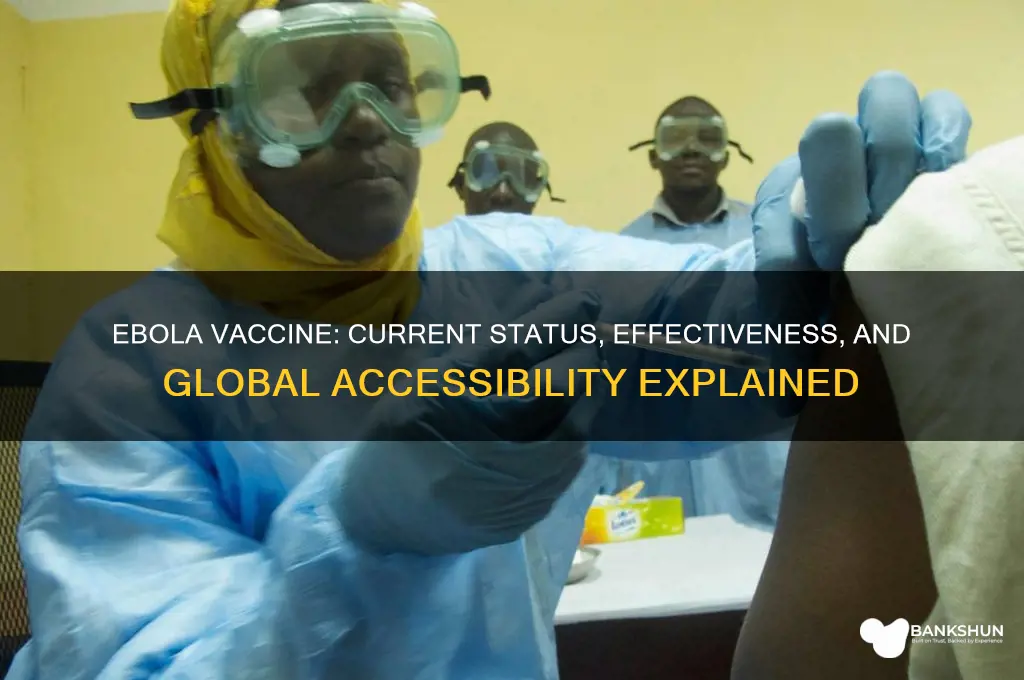
Effectiveness of approved Ebola vaccines
As of recent developments, several Ebola vaccines have been approved or are in advanced stages of development, marking a significant milestone in the fight against this deadly virus. Among these, the rVSV-ZEBOV vaccine, also known as Ervebo, stands out as the first to receive regulatory approval. Its effectiveness has been demonstrated in clinical trials, particularly in the 2014-2016 West African outbreak, where it showed approximately 97.5% efficacy in preventing Ebola virus disease when administered in a single dose. This vaccine is recommended for individuals aged 18 years and older, including those at high risk of exposure, such as healthcare workers and frontline responders in outbreak areas.
The administration of the rVSV-ZEBOV vaccine involves a single intramuscular injection, typically in the deltoid muscle. It is crucial to follow the manufacturer’s guidelines for storage and handling, as the vaccine requires refrigeration at 2–8°C. In emergency situations, the vaccine can be used under a "ring vaccination" strategy, where contacts and contacts of contacts of confirmed Ebola cases are vaccinated to create a protective barrier around the outbreak. This approach has proven effective in limiting the spread of the virus during recent outbreaks in the Democratic Republic of Congo.
Another notable vaccine, the Ad26.ZEBOV and MVA-BN-Filo regimen, is a two-dose vaccine that has shown promising results in Phase 2 and 3 trials. The first dose, Ad26.ZEBOV, is administered followed by a booster dose of MVA-BN-Filo 56 days later. This regimen has demonstrated robust immune responses and is being considered for broader use, particularly in regions where a two-dose approach may be more feasible. Its effectiveness is still under evaluation, but preliminary data suggest it could provide durable protection against multiple Ebola virus species.
Comparatively, the rVSV-ZEBOV vaccine’s single-dose regimen offers practical advantages in outbreak settings, where rapid deployment is critical. However, its long-term immunity is still being studied, and booster doses may be necessary. In contrast, the two-dose Ad26.ZEBOV and MVA-BN-Filo regimen may offer more sustained immunity but requires careful planning to ensure recipients return for the second dose. Both vaccines highlight the importance of tailoring vaccination strategies to the specific needs of affected communities.
In conclusion, the effectiveness of approved Ebola vaccines is a testament to scientific innovation and global collaboration. While rVSV-ZEBOV remains the primary tool in current outbreak responses, ongoing research into multi-dose regimens like Ad26.ZEBOV and MVA-BN-Filo expands the arsenal against Ebola. Practical considerations, such as dosage schedules, storage requirements, and community acceptance, play a crucial role in maximizing the impact of these vaccines. As these tools continue to evolve, they offer hope for controlling and eventually eradicating Ebola virus disease.
Exploring Barclays Bank's Extensive Branch Network Across Europe
You may want to see also
Explore related products






![]()
Side effects of Ebola vaccines
Ebola vaccines, such as Ervebo (rVSV-ZEBOV) and Zabdeno/Mvabea (Ad26.ZEBOV and MVA-BN-Filo), have been developed to combat the deadly virus, but like any medical intervention, they come with potential side effects. Understanding these side effects is crucial for informed decision-making, especially in regions where Ebola outbreaks are a persistent threat. Clinical trials and real-world use have provided valuable insights into what recipients might experience after vaccination.
Common Side Effects: What to Expect
Most side effects of Ebola vaccines are mild to moderate and resolve within a few days. These include pain, swelling, or redness at the injection site, similar to reactions from routine vaccinations. Systemic symptoms like fever, fatigue, headache, and muscle pain are also frequently reported. For instance, in trials of Ervebo, approximately 50% of recipients experienced headache, and around 30% reported fatigue. These reactions typically occur within 24 hours of vaccination and can be managed with over-the-counter pain relievers, such as acetaminophen, following healthcare provider guidance. It’s important to stay hydrated and rest if these symptoms arise.
Less Common but Notable Reactions
While rare, some individuals may experience more severe or unusual side effects. Arthralgia (joint pain) and transient rashes have been documented in a small percentage of vaccine recipients. In extremely rare cases, allergic reactions, including anaphylaxis, can occur, though this is uncommon. Healthcare providers administering the vaccine are trained to monitor for such reactions and have protocols in place to manage them promptly. Individuals with a history of severe allergies should inform their healthcare provider before receiving the vaccine.
Special Considerations for Specific Populations
Certain groups require careful evaluation before vaccination. Pregnant and breastfeeding individuals were initially excluded from clinical trials, but ongoing studies are assessing safety in these populations. Current recommendations suggest that the benefits of vaccination may outweigh the risks in high-risk settings, but consultation with a healthcare provider is essential. Similarly, immunocompromised individuals may have a reduced immune response to the vaccine, and their healthcare provider should weigh the risks and benefits. For children, Ervebo is approved for use in individuals aged 18 and older, while Zabdeno/Mvabea is authorized for those aged 1 year and older, with dosage adjustments based on age.
Practical Tips for Managing Side Effects
To minimize discomfort, apply a cool, damp cloth to the injection site if swelling or pain occurs. Avoid strenuous activity for 24 hours post-vaccination to reduce the risk of exacerbating side effects. Keep a record of any symptoms and their duration, especially if they persist beyond 72 hours or worsen. If severe symptoms like difficulty breathing, swelling of the face, or persistent high fever occur, seek medical attention immediately. Finally, stay informed about local health guidelines, as recommendations may evolve based on new research or outbreak dynamics.
In summary, while Ebola vaccines are a critical tool in preventing the spread of this deadly virus, being aware of potential side effects ensures preparedness and promotes trust in vaccination efforts. Most reactions are manageable, but vigilance and proactive communication with healthcare providers are key to a safe vaccination experience.
Historic Bank Heists: Have Robbers Ever Truly Escaped Justice?
You may want to see also
Explore related products






![]()
Global distribution of Ebola vaccines
Ebola vaccines have been developed and deployed in recent outbreaks, but their global distribution remains a complex challenge. The rVSV-ZEBOV vaccine, approved by the FDA in 2019, has been a game-changer in controlling outbreaks, particularly in the Democratic Republic of Congo (DRC). However, ensuring equitable access to these vaccines across affected and at-risk regions involves navigating logistical, financial, and political hurdles. For instance, the vaccine requires storage at -60°C to -80°C, a significant barrier in low-resource settings with limited cold chain infrastructure.
Analyzing distribution strategies reveals a reliance on ring vaccination, where contacts of confirmed cases and their contacts are prioritized. This method proved effective in the 2018-2020 DRC outbreak, reducing case counts by 97.5%. However, this approach assumes robust surveillance systems, which are often lacking in remote or conflict-affected areas. Additionally, the vaccine’s two-dose regimen (Ervebo, administered 8 weeks apart) complicates adherence, particularly in populations with high mobility or limited healthcare access. Single-dose alternatives, such as the Ad26.ZEBOV and MVA-BN-Filo regimen, are under trial but not yet widely available.
From a persuasive standpoint, global health organizations must prioritize pre-positioning vaccines in at-risk countries to enable rapid response. The World Health Organization’s (WHO) Ebola vaccine stockpile, established in 2021, is a step forward but remains underfunded and insufficient for large-scale outbreaks. Wealthier nations and pharmaceutical companies should commit to dose-sharing agreements and technology transfers to local manufacturers, ensuring sustainable production in endemic regions. For example, the Serum Institute of India’s partnership to produce rVSV-ZEBOV at a lower cost could serve as a model.
Comparatively, the COVID-19 vaccine rollout highlights lessons for Ebola distribution. While COVAX aimed for global equity, wealthier nations hoarded doses, leaving low-income countries underserved. Ebola vaccines must avoid this pitfall by implementing fair allocation frameworks from the outset. Practical tips for local health workers include community engagement to address vaccine hesitancy, using solar-powered cold chain solutions, and training staff in ultra-cold storage management. For instance, in the DRC, motorcycle-mounted refrigerators were used to transport vaccines to remote villages.
In conclusion, the global distribution of Ebola vaccines demands a multifaceted approach—combining innovative logistics, equitable policies, and local capacity-building. Without addressing these challenges, even the most effective vaccines will fail to reach those who need them most. The next outbreak is not a question of "if" but "when," making proactive, collaborative action imperative.
Spotting Fake Vaccine Passports: Essential Tips to Verify Authenticity
You may want to see also
Explore related products






![]()
Ongoing research for new Ebola vaccines
Ebola virus disease (EVD) remains a significant public health threat, particularly in regions where outbreaks occur. While the Ervebo vaccine has been a breakthrough, ongoing research is critical to developing more effective, accessible, and versatile vaccines. Scientists are exploring innovative approaches to improve vaccine efficacy, reduce dosage requirements, and extend protection to broader populations, including children and immunocompromised individuals.
One promising avenue is the development of single-dose vaccines. Current regimens often require multiple doses, which can be logistically challenging in outbreak settings. Researchers are testing formulations that elicit robust immunity with just one injection, such as the Ad26.ZEBOV and MVA-BN-Filo combination, which has shown efficacy in clinical trials. Another strategy involves adjuvants—substances added to vaccines to enhance immune response. For instance, the GSK vaccine candidate uses an AS01B adjuvant, enabling lower antigen doses while maintaining effectiveness. These advancements could simplify distribution and increase uptake in resource-limited areas.
Beyond dosage optimization, researchers are investigating vaccines targeting multiple Ebola strains. The Zaire ebolavirus is the most common cause of outbreaks, but other strains like Sudan ebolavirus also pose threats. Broad-spectrum vaccines, such as those using virus-like particles (VLPs) or nanoparticle technologies, aim to protect against several variants simultaneously. This approach could provide long-term immunity and reduce the need for strain-specific vaccines during outbreaks.
Pediatric populations are another focus of ongoing research. Children under 18 were excluded from early Ebola vaccine trials, leaving a gap in protection for this vulnerable group. Recent studies, such as the PREVAC trial, are evaluating the safety and immunogenicity of vaccines in children as young as 1 year old. Preliminary results suggest that lower doses may be sufficient for younger age groups, minimizing side effects while ensuring adequate immunity.
Finally, researchers are addressing the challenge of vaccine stability in tropical climates. Traditional vaccines often require cold chain storage, which is impractical in many Ebola-affected regions. Thermostable formulations, such as lyophilized (freeze-dried) vaccines, are being developed to withstand higher temperatures without losing potency. This innovation could revolutionize vaccine delivery, making it more feasible to reach remote and underserved communities.
In summary, ongoing research for new Ebola vaccines is multifaceted, targeting single-dose regimens, broad-spectrum protection, pediatric applications, and improved stability. These advancements hold the potential to transform Ebola prevention, making vaccines more accessible, effective, and adaptable to the needs of diverse populations. As science progresses, the goal of eradicating Ebola outbreaks moves closer to reality.
Step-by-Step Guide to Deactivating Your SBI Internet Banking ID
You may want to see also
Frequently asked questions
Yes, there is a vaccine called Ervebo (rVSV-ZEBOV) that has been approved for use against the Zaire ebolavirus species, which is the most common cause of Ebola outbreaks.
The Ervebo vaccine has shown high efficacy, with studies indicating it is approximately 97.5% effective in preventing Ebola virus disease when used in a ring vaccination strategy during outbreaks.
The Ebola vaccine is primarily recommended for individuals at high risk of exposure, including healthcare workers, laboratory staff, and those in close contact with infected individuals during outbreaks. It is also used in a ring vaccination strategy to protect communities in affected areas.