The debate over whether vaccine-induced immunity is superior to natural immunity acquired through infection has gained significant attention, particularly in the context of the COVID-19 pandemic. While recovering from an infection can provide some level of protection against future illness, vaccines offer a safer and more controlled method of achieving immunity. Vaccines are designed to trigger a robust immune response without exposing individuals to the risks associated with the disease, such as severe symptoms, long-term complications, or death. Additionally, vaccine immunity often produces a more consistent and predictable immune memory, whereas natural infection can result in variable levels of protection depending on the severity of the illness. Public health experts emphasize that vaccination remains the most reliable way to build population-level immunity while minimizing harm, making it a cornerstone of disease prevention strategies.
Explore related products






What You'll Learn
![]()
Vaccine Safety vs. Infection Risks
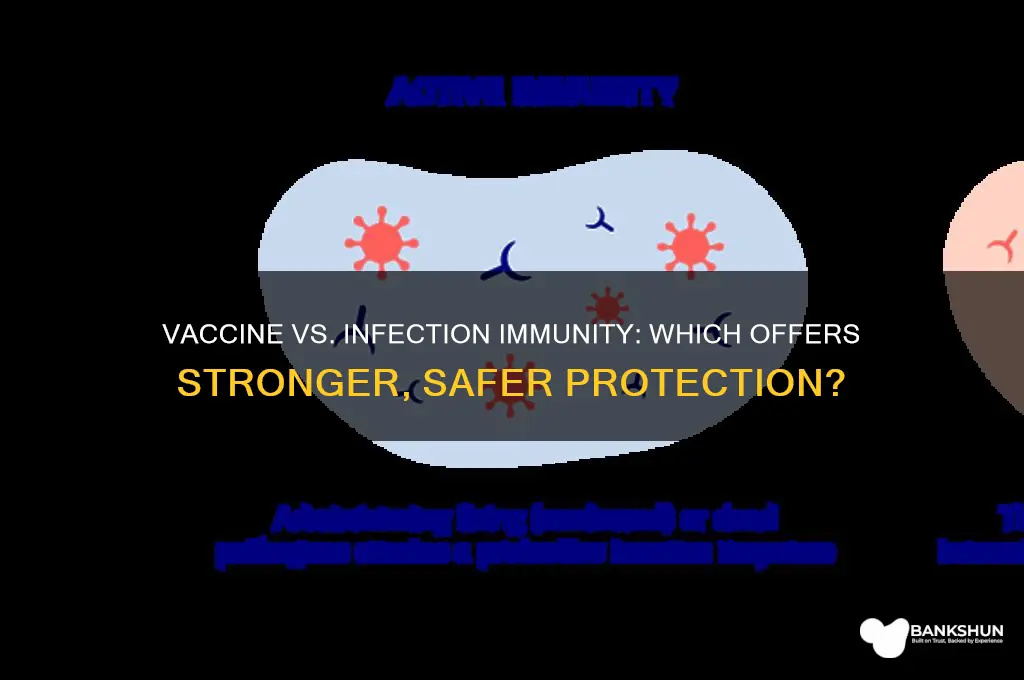
Vaccine-induced immunity offers a controlled, predictable response to pathogens, minimizing the risks associated with natural infection. Vaccines introduce a harmless version or component of the virus, triggering the immune system to produce antibodies and memory cells without causing disease. For instance, the COVID-19 mRNA vaccines deliver genetic instructions for cells to create a spike protein, prompting an immune reaction. This process bypasses the dangers of severe illness, hospitalization, or long-term complications like myocarditis or multisystem inflammatory syndrome, which can occur with natural infection. A single dose of an mRNA vaccine contains precisely measured micrograms of active ingredient, ensuring safety while eliciting a robust immune response.
Consider the measles virus, a highly contagious pathogen with a 1 in 500 risk of causing encephalitis in infected individuals. The measles vaccine, administered in two doses (typically at 12–15 months and 4–6 years), provides over 95% immunity without exposing recipients to the virus’s life-threatening complications. In contrast, natural infection not only endangers the individual but also poses a risk to unvaccinated populations, particularly infants too young to receive the vaccine. This example underscores the principle that vaccines confer immunity while eliminating the inherent risks of infection, such as organ damage, neurological sequelae, or death.
From a practical standpoint, vaccine safety protocols are rigorously tested through clinical trials involving tens of thousands of participants across diverse age groups, ensuring efficacy and identifying rare side effects. For example, the FDA’s approval process for COVID-19 vaccines included monitoring for adverse events like anaphylaxis (occurring in approximately 2–5 cases per million doses) and implementing safeguards such as 15–30 minute post-vaccination observation periods. In contrast, the risks of natural infection are unpredictable and often irreversible, with conditions like post-COVID syndrome affecting up to 30% of non-hospitalized individuals. To mitigate vaccine-related risks, individuals with severe allergies should consult allergists before vaccination and ensure access to epinephrine.
A comparative analysis reveals that while both vaccination and natural infection can lead to immunity, the latter is a dangerous gamble. For example, chickenpox infection confers lifelong immunity but carries risks of bacterial skin infections, pneumonia, or, in rare cases, encephalitis. The varicella vaccine, administered in two doses (first dose at 12–15 months, second at 4–6 years), provides comparable immunity with a significantly lower adverse event profile. Parents should weigh the 1 in 1,000 risk of severe complications from chickenpox against the 1 in 1,000,000 risk of serious vaccine reactions, opting for the safer route.
Ultimately, the choice between vaccine-induced and infection-induced immunity is not one of equivalence but of risk management. Vaccines are a tool to harness the immune system’s power without subjecting individuals to the unpredictability of disease. For maximum protection, adhere to recommended vaccine schedules, report adverse reactions via systems like VAERS, and stay informed about booster requirements. By prioritizing vaccine safety over infection risks, individuals safeguard not only their health but also contribute to community immunity, protecting vulnerable populations from preventable diseases.
Mastering Relationship Banking: Strategies to Enhance Client Connections and Success
You may want to see also
Explore related products






![]()
Duration of Immunity Comparison
Vaccine-induced immunity and infection-induced immunity differ significantly in their duration, a critical factor in long-term protection against diseases. Vaccines are designed to provide a robust and consistent immune response, often with a predictable timeline. For instance, the mRNA COVID-19 vaccines (Pfizer-BioNTech and Moderna) have been shown to offer strong protection for at least 6 months after the second dose, with booster shots recommended to extend this duration. In contrast, immunity from a natural COVID-19 infection varies widely, with studies indicating that protection can wane after 3 to 6 months, depending on the severity of the initial infection and individual immune responses.
To illustrate, consider the influenza virus. Annual flu vaccines are necessary because the virus mutates rapidly, and vaccine-induced immunity typically lasts only about 6 to 8 months. However, natural infection with influenza may provide longer-lasting immunity to the specific strain encountered, but this does not protect against new variants. This highlights a key trade-off: while infection-induced immunity can be strain-specific and variable, vaccine immunity is standardized and can be updated to target emerging variants.
From a practical standpoint, maintaining immunity through vaccination is more controllable and safer. For example, the tetanus vaccine provides protection for about 10 years, and booster shots are recommended every decade. In contrast, relying on natural infection for tetanus immunity is not only dangerous but also unpredictable, as the severity of the disease can vary widely. Vaccines offer a structured approach to immunity, allowing healthcare providers to schedule boosters and monitor antibody levels, ensuring consistent protection.
A comparative analysis reveals that vaccine immunity often surpasses infection immunity in terms of reliability and safety. Vaccines are rigorously tested to ensure they provide a durable immune response without the risks associated with natural infection, such as severe illness or long-term complications. For instance, measles infection confers lifelong immunity, but it also carries a risk of serious complications like encephalitis. The measles vaccine, on the other hand, provides similarly long-lasting immunity with minimal side effects, making it the safer choice.
In conclusion, while infection-induced immunity can be potent, its duration is often unpredictable and varies by individual and pathogen. Vaccine immunity, though sometimes requiring boosters, offers a safer, more standardized, and controllable approach to long-term protection. For optimal health outcomes, vaccination remains the preferred method for achieving and maintaining immunity, especially for diseases with severe consequences or high variability in natural infection outcomes.
Steps to Become a Reserve Bank Officer: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Variant Protection Differences
Vaccine-induced immunity and infection-induced immunity differ significantly in their ability to protect against emerging variants, a critical factor in the ongoing battle against rapidly evolving pathogens like SARS-CoV-2. While natural infection exposes the immune system to the entire virus, vaccines typically target specific antigens, such as the spike protein. This difference in exposure can lead to variations in the breadth and durability of immune responses, particularly when new variants arise with mutations in these key regions. For instance, the Omicron variant’s extensive spike protein mutations reduced the neutralizing antibody efficacy of both vaccinated and naturally infected individuals, but vaccinated individuals generally retained higher levels of cross-reactive T-cell immunity, which is crucial for preventing severe disease.
Consider the practical implications for individuals aged 65 and older, who are at higher risk of severe outcomes from COVID-19. A booster dose of an mRNA vaccine (e.g., 30 µg of Pfizer-BioNTech or Moderna) significantly enhances neutralizing antibody titers against variants like Delta and Omicron, providing a more robust defense compared to relying solely on immunity from a prior infection. Studies show that hybrid immunity—a combination of vaccination and natural infection—offers the most comprehensive protection, but this is not a recommended strategy due to the risks associated with infection. Instead, staying up-to-date with recommended vaccine doses is the safest way to maintain variant protection, especially as new formulations targeting specific variants become available.
From a comparative perspective, infection-induced immunity often wanes more rapidly against variants due to its reliance on a narrower range of antibodies. Vaccines, on the other hand, are designed to elicit a more focused and potent response, which can be adapted to target new variants through updated formulations. For example, bivalent mRNA vaccines, which include components of both the original virus and the Omicron variant, have demonstrated improved neutralizing activity against Omicron subvariants compared to monovalent vaccines. This adaptability gives vaccines a distinct advantage in the context of variant protection, as they can be rapidly modified to address evolving threats.
To maximize variant protection, individuals should follow a few key steps: first, complete the primary vaccine series as recommended by health authorities (typically two doses of an mRNA vaccine or one dose of Johnson & Johnson followed by an mRNA booster). Second, receive all recommended booster doses, especially if you are in a high-risk age group or have underlying health conditions. Third, monitor public health updates for new vaccine formulations targeting emerging variants and get vaccinated as soon as eligible. Caution should be exercised against relying on natural infection for immunity, as this approach carries significant risks, including long-term health complications and the potential for transmitting the virus to others.
In conclusion, while both vaccine-induced and infection-induced immunity offer protection against COVID-19, vaccines provide a more reliable and adaptable defense against variants. Their ability to be updated and their role in stimulating a broad immune response make them a superior choice for long-term protection. By staying informed and proactive about vaccination, individuals can significantly reduce their risk of severe disease and contribute to broader public health efforts to control the pandemic.
Understanding BBI: Decoding the Banking Term and Its Significance
You may want to see also
Explore related products






![]()
Herd Immunity Impact Analysis
Vaccine-induced immunity and infection-induced immunity both contribute to herd immunity, but their impacts differ significantly in terms of safety, efficacy, and societal burden. Herd immunity, the indirect protection that occurs when a large portion of a community becomes immune to a disease, is a critical public health goal. Vaccines offer a controlled, safer route to achieving this threshold, while natural infection carries inherent risks and unpredictable outcomes. Analyzing the impact of each approach reveals why vaccines are the preferred method for building herd immunity.
Consider the measles vaccine, which provides over 95% immunity after two doses, typically administered at 12–15 months and 4–6 years of age. This high efficacy rate means that in a fully vaccinated population, the virus struggles to find susceptible hosts, effectively halting transmission. In contrast, achieving herd immunity through natural infection would require approximately 90–95% of the population to contract measles. Given its complications—including pneumonia, encephalitis, and a 1–2% hospitalization rate in children—this approach would result in unnecessary morbidity and mortality. For example, a single measles outbreak in an unvaccinated community could lead to hundreds of cases, dozens of hospitalizations, and potential fatalities, particularly among vulnerable groups like infants and immunocompromised individuals.
Instructively, the COVID-19 pandemic provides a real-world comparison. Countries relying on vaccination campaigns, such as Israel and Singapore, achieved rapid declines in cases and hospitalizations by prioritizing high-risk groups (e.g., elderly and immunocompromised individuals) and maintaining consistent booster schedules. Conversely, regions allowing natural infection to spread uncontrolled, like parts of Brazil and India, faced overwhelmed healthcare systems, long-term complications (e.g., "long COVID"), and higher death rates. Vaccines not only reduce individual risk but also minimize the societal costs of lockdowns, economic disruption, and healthcare strain.
Persuasively, the economic argument for vaccine-driven herd immunity is compelling. A study by the Johns Hopkins Bloomberg School of Public Health estimated that every $1 spent on childhood immunizations yields $44 in economic benefits, primarily by preventing costly treatments and lost productivity. Natural infection, on the other hand, incurs direct medical expenses and indirect costs like absenteeism and reduced workforce capacity. For instance, a single case of measles can cost up to $10,000 in treatment, while a COVID-19 hospitalization averages $20,000. Scaling these costs to population levels underscores the financial wisdom of investing in vaccination programs.
Comparatively, the durability of immunity also favors vaccines in certain contexts. While natural infection with diseases like chickenpox confers lifelong immunity, others, such as COVID-19 or influenza, result in waning immunity over time. Vaccines, however, can be engineered to target specific viral components (e.g., spike proteins in mRNA vaccines) and updated to address emerging variants. For example, annual flu vaccines are reformulated based on circulating strains, offering tailored protection that natural infection cannot match. This adaptability ensures sustained herd immunity even as pathogens evolve.
Descriptively, the ethical dimension of herd immunity strategies cannot be overlooked. Relying on natural infection disproportionately harms marginalized communities with limited access to healthcare, higher comorbidity rates, and greater exposure risks. Vaccines, when equitably distributed, provide a shield for these populations, reducing disparities in disease burden. Practical tips for maximizing herd immunity include adhering to recommended vaccine schedules, promoting booster doses for waning immunity, and addressing vaccine hesitancy through education and accessible clinics. By prioritizing vaccination, societies can achieve herd immunity with minimal harm, ensuring protection for all.
Chain Bank Season Dates: When Does It Run and Key Deadlines
You may want to see also
Explore related products






![]()
Side Effects and Long-Term Effects
Vaccine side effects are immediate, measurable, and often mild—think soreness at the injection site, fatigue, or a low-grade fever. These reactions, typically lasting 1–3 days, signal the immune system’s activation, not danger. For instance, the Pfizer-BioNTech and Moderna COVID-19 vaccines, administered in two doses 3–4 weeks apart, commonly cause arm pain in 70–80% of recipients and systemic symptoms like headache or chills in 50–60% after the second dose. In contrast, infection-induced immunity often comes with unpredictable and severe acute symptoms, such as high fever, respiratory distress, or organ damage, as seen in 20% of symptomatic COVID-19 cases. The trade-off is clear: vaccines offer controlled, short-term discomfort for long-term protection, while infections risk immediate, life-threatening complications.
Long-term effects of vaccines are rare and well-studied, with decades of data supporting their safety. For example, the HPV vaccine, administered in a 2- or 3-dose series depending on age, has been monitored in over 130 million recipients since 2006, with no significant long-term risks identified beyond occasional fainting post-injection. Conversely, infection-induced immunity can lead to persistent, debilitating conditions. Post-COVID syndrome, affecting 10–30% of survivors, includes fatigue, cognitive dysfunction, and cardiovascular issues lasting months or years. Similarly, measles, a vaccine-preventable disease, can cause subacute sclerosing panencephalitis (SSPE), a fatal brain disorder, in 1 in 10,000 cases. Vaccines minimize these risks by bypassing the disease’s most dangerous phases.
Consider the age-specific risks: children under 5, who receive vaccines like MMR and DTaP in multiple doses starting at 2 months, face higher infection risks due to underdeveloped immune systems. Vaccines protect them without exposing them to potential complications like pneumonia (from measles) or brain damage (from pertussis). For older adults, the COVID-19 vaccine’s side effects, though slightly more pronounced due to age-related immune changes, are far preferable to the 80% hospitalization rate among unvaccinated seniors infected with the virus. Tailoring vaccine schedules and dosages to age groups maximizes safety while ensuring robust immunity.
Practical tip: Monitor side effects post-vaccination using symptom trackers like the CDC’s V-safe app, which helps distinguish normal reactions from rare adverse events. For infections, long-term monitoring is essential; survivors of severe diseases like COVID-19 or chickenpox should undergo regular check-ups to detect complications early. While vaccines occasionally cause severe reactions (e.g., anaphylaxis in 1.3 per million mRNA vaccine doses), these are treatable with prompt medical intervention. Infections, however, leave no room for such control, making prevention through vaccination the safer choice.
The takeaway is straightforward: vaccine side effects are a small, manageable price for immunity without the gamble of infection consequences. While both routes trigger immune memory, vaccines decouple protection from the dangers of disease progression. Choosing vaccination isn’t just about avoiding short-term discomfort—it’s about eliminating the long-term uncertainties infections carry. As with any medical decision, weigh the evidence: vaccines offer predictable, studied outcomes, while infections bring chaos and risk. The choice is yours, but the data favors the needle over the nightmare.
Step-by-Step Guide to Filling HDFC Bank's Form A2 Easily
You may want to see also
Frequently asked questions
Vaccine immunity is generally considered safer and more controlled than infection immunity, as vaccines provide protection without the risks of severe illness or long-term complications associated with natural infection.
The duration of immunity varies, but vaccines often provide consistent and predictable protection, while immunity from natural infection can be less reliable and may wane over time.
Vaccines, especially updated or booster doses, are designed to target variants and provide broad protection, whereas natural infection may not offer robust defense against new strains.
Yes, relying on infection immunity carries significant risks, including severe illness, hospitalization, long COVID, and potential death, whereas vaccines are a safer way to build immunity.