The question of whether schools should mandate vaccinations for children before entry is a contentious and multifaceted issue that intersects public health, individual rights, and educational policy. Proponents argue that vaccination requirements protect not only individual students but also the broader community by preventing the spread of preventable diseases, particularly in environments where children are in close proximity. They emphasize the success of vaccines in eradicating or controlling diseases like measles and polio, and view mandates as a necessary measure to maintain herd immunity. However, opponents raise concerns about parental autonomy, potential vaccine side effects, and the ethical implications of denying education to unvaccinated children. This debate highlights the need to balance collective well-being with personal freedoms, while also addressing misinformation and ensuring equitable access to vaccines. Ultimately, the decision requires careful consideration of scientific evidence, societal values, and the long-term impact on public health and education systems.
| Characteristics | Values |
|---|---|
| Public Health Protection | Vaccination reduces the spread of infectious diseases in school settings. |
| Herd Immunity | High vaccination rates protect vulnerable individuals who cannot be vaccinated. |
| Disease Prevention | Prevents outbreaks of vaccine-preventable diseases like measles, mumps, and whooping cough. |
| School Attendance | Vaccinated children are less likely to miss school due to preventable illnesses. |
| Cost-Effectiveness | Reduces healthcare costs associated with treating vaccine-preventable diseases. |
| Legal and Ethical Considerations | Balancing individual rights with community health may lead to legal debates. |
| Parental Choice | Some parents may oppose vaccination due to personal beliefs or concerns. |
| Vaccine Safety | Vaccines are rigorously tested and proven safe for the majority of children. |
| Global Health Standards | Many countries mandate vaccinations for school entry to align with global health goals. |
| Educational Impact | Healthy students contribute to a more stable and productive learning environment. |
| Policy Enforcement | Schools may face challenges in verifying vaccination status and enforcing policies. |
| Equity in Access | Ensuring all children, regardless of socioeconomic status, have access to vaccines. |
| Scientific Consensus | Overwhelming scientific evidence supports the benefits of childhood vaccination. |
| Community Trust | Building trust in vaccines and public health systems is crucial for compliance. |
| Potential Exemptions | Medical, religious, or philosophical exemptions may be allowed in some regions. |
Explore related products

$17.01 $16.95





What You'll Learn
- Vaccine Mandates vs. Parental Choice: Balancing public health with individual rights in school policies
- Herd Immunity Benefits: How vaccinated students protect vulnerable peers and communities
- Safety and Side Effects: Addressing concerns about vaccine risks for children
- Disease Outbreak Prevention: Reducing preventable illnesses in crowded school environments
- Equity in Access: Ensuring all children, regardless of background, receive necessary vaccinations
![]()
Vaccine Mandates vs. Parental Choice: Balancing public health with individual rights in school policies
The debate over vaccine mandates in schools pits the collective good against individual freedoms, a tension that has only intensified in recent years. On one side, public health advocates argue that requiring vaccinations before school entry protects vulnerable populations, prevents outbreaks, and maintains herd immunity. For instance, the measles vaccine, administered in two doses between 12 and 15 months and again between 4 and 6 years, has been a cornerstone of school entry requirements for decades, effectively eradicating the disease in many regions. Yet, opponents counter that such mandates infringe on parental rights, citing concerns over vaccine safety, religious beliefs, or personal autonomy. This clash raises a critical question: How can schools balance the undeniable benefits of vaccination with respect for individual choice?
Consider the practical implications of vaccine mandates. Schools serve as communal hubs, where children in close proximity can rapidly spread infectious diseases. A single unvaccinated child can become a vector, endangering classmates with compromised immune systems or those too young to receive certain vaccines. For example, the CDC recommends the Tdap vaccine (tetanus, diphtheria, and pertussis) for preteens around age 11 or 12, yet without mandates, coverage rates may fall below the 95% threshold needed for herd immunity. Mandates, therefore, act as a safeguard, ensuring that public spaces like schools remain safe for all. However, implementing such policies requires sensitivity to exceptions, such as medical exemptions for children with allergies to vaccine components like gelatin or egg proteins.
From a parental perspective, the argument for choice often hinges on trust—or the lack thereof—in medical institutions and government bodies. Some parents fear over-vaccination or long-term side effects, despite extensive research affirming vaccine safety. Others view mandates as an overreach of authority, prioritizing their right to decide what’s best for their child. To address these concerns, schools and policymakers could adopt a hybrid approach: require vaccinations for entry but allow exemptions for valid medical or religious reasons. This model, used in states like California, strikes a balance by upholding public health while respecting individual circumstances. However, it also demands rigorous verification processes to prevent abuse of exemptions, as seen in communities where non-medical opt-out rates have fueled outbreaks.
A comparative analysis of global policies offers further insight. Countries like Australia employ a "No Jab, No Pay" policy, withholding child care benefits from parents who refuse vaccinations, while France mandates 11 vaccines for school entry. In contrast, the U.S. system is decentralized, with states setting their own requirements, leading to inconsistencies. For instance, Mississippi and West Virginia allow only medical exemptions, resulting in near-universal compliance, whereas states with lenient policies see higher rates of vaccine-preventable diseases. These examples suggest that while mandates are effective, their success depends on cultural acceptance, enforcement mechanisms, and public education campaigns. Schools can play a pivotal role by hosting workshops, providing multilingual resources, and partnering with healthcare providers to address parental hesitancy.
Ultimately, the vaccine mandate debate is not about absolute rights but about navigating trade-offs. Public health thrives on collective action, yet individual freedoms are a cornerstone of democratic societies. Schools must act as mediators, fostering dialogue and implementing policies that prioritize safety without alienating families. Practical steps include offering on-site vaccination clinics, ensuring transparency in exemption processes, and tailoring communication to address specific concerns. By combining rigor with empathy, schools can create environments where both community well-being and personal choice are valued, setting a precedent for how society tackles complex ethical dilemmas.
Is BMO Harris Bank Right for You? A Comprehensive Review
You may want to see also
Explore related products






![]()
Herd Immunity Benefits: How vaccinated students protect vulnerable peers and communities
Vaccinating students before school entry doesn’t just safeguard individual children—it creates a protective shield around the entire community. This concept, known as herd immunity, occurs when a high percentage of a population becomes immune to a disease, making its spread unlikely. In schools, where close contact is unavoidable, herd immunity acts as a firewall, preventing outbreaks that could harm vulnerable individuals who cannot be vaccinated due to medical conditions like immunodeficiency or severe allergies. For instance, measles requires 93–95% vaccination coverage to achieve herd immunity, a threshold that schools can help meet by enforcing vaccination policies.
Consider the practical steps schools can take to maximize this benefit. First, implement a mandatory vaccination policy for all eligible students, with exemptions granted only for legitimate medical reasons. Second, collaborate with local health departments to offer on-site vaccination clinics during enrollment periods, ensuring convenience for families. Third, educate parents about the communal impact of vaccination, emphasizing how their child’s immunization protects classmates with conditions like leukemia or asthma, who are at higher risk of complications from vaccine-preventable diseases. For example, a single dose of the MMR vaccine is 93% effective against measles, while two doses raise protection to 97%, significantly reducing the risk of classroom outbreaks.
Critics often argue that individual freedoms should outweigh communal benefits, but the data tell a different story. In 2019, a measles outbreak in a U.S. school with low vaccination rates resulted in 47 cases, including hospitalizations of immunocompromised students. Conversely, schools with strict vaccination policies, like those in Australia’s “No Jab, No Play” program, have seen a 95% vaccination rate among enrolled children, virtually eliminating outbreaks of diseases like pertussis and mumps. These examples illustrate that herd immunity isn’t just a theoretical concept—it’s a proven strategy that saves lives.
To sustain herd immunity, schools must also address vaccine hesitancy through transparent communication. Provide parents with clear, evidence-based information about vaccine safety and efficacy, dispelling myths like the debunked link between the MMR vaccine and autism. Offer multilingual resources and engage trusted community leaders to bridge cultural or linguistic gaps. Finally, monitor vaccination rates annually and intervene in areas of low compliance with targeted outreach. By treating herd immunity as a shared responsibility, schools can transform themselves from potential hotspots into bastions of public health, protecting not just students but the broader community.
Mastering Bank Strategies: Defeating Valkyrie Caera in Competitive Play
You may want to see also
Explore related products






![]()
Safety and Side Effects: Addressing concerns about vaccine risks for children
Vaccine safety is a cornerstone of public health, yet concerns about side effects persist, especially among parents considering school entry requirements. Understanding the rigorous testing and monitoring vaccines undergo can alleviate fears. Before approval, vaccines are tested in clinical trials involving thousands of participants, with specific studies focusing on pediatric populations. For instance, the MMR vaccine, commonly required for school entry, has been administered to millions of children worldwide since its introduction in 1971, with extensive data confirming its safety profile. Post-approval, surveillance systems like the Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD) continuously monitor for rare or unexpected side effects, ensuring ongoing safety.
Common side effects of childhood vaccines, such as soreness at the injection site, mild fever, or fussiness, are typically mild and short-lived. For example, the DTaP vaccine, which protects against diphtheria, tetanus, and pertussis, may cause fever in up to 1 in 4 children, but these symptoms usually resolve within 48 hours. Severe reactions are exceedingly rare; anaphylaxis, a severe allergic reaction, occurs in approximately 1 in a million doses. Parents should be reassured that healthcare providers are trained to manage such events, and schools often have protocols in place to respond to medical emergencies. Practical tips include administering acetaminophen or ibuprofen for fever or discomfort, as recommended by the CDC, and keeping children hydrated post-vaccination.
Comparing vaccine risks to the dangers of preventable diseases highlights the importance of immunization. For example, measles, a highly contagious virus, can lead to pneumonia, encephalitis, and even death, particularly in young children. In contrast, the MMR vaccine’s side effects are minimal, with less than 1 in a million doses resulting in serious complications. Similarly, the risks of polio, which can cause paralysis, far outweigh the rare side effects of the inactivated polio vaccine (IPV). This comparative perspective underscores the critical role vaccines play in protecting children and communities, especially in school settings where diseases can spread rapidly.
Addressing parental concerns requires clear, empathetic communication. Healthcare providers and school administrators should emphasize that vaccines are not one-size-fits-all; dosages and schedules are tailored to age groups, such as the hepatitis B vaccine given at birth, followed by additional doses at 1–2 months and 6–18 months. For older children entering school, booster shots ensure continued immunity. Parents should be encouraged to ask questions and seek information from reliable sources, such as the CDC or WHO, rather than unverified online claims. By fostering trust and providing accurate, actionable information, we can mitigate fears and promote informed decision-making.
Ultimately, the benefits of vaccination in preventing serious diseases and protecting public health far outweigh the minimal risks. Schools requiring vaccinations before entry not only safeguard individual students but also contribute to herd immunity, protecting vulnerable populations who cannot be vaccinated. While side effects are a valid concern, they are rare, manageable, and far less dangerous than the diseases they prevent. By focusing on evidence-based information and practical strategies, parents and educators can work together to ensure a safe and healthy learning environment for all children.
Activating iSafe ICICI Bank: A Step-by-Step Guide for Secure Access
You may want to see also
Explore related products






![]()
Disease Outbreak Prevention: Reducing preventable illnesses in crowded school environments
Schools, with their dense populations and close contact, are fertile grounds for disease transmission. A single unvaccinated child can introduce a preventable illness like measles or whooping cough, triggering an outbreak that endangers not only classmates but also vulnerable individuals in the wider community. This risk is not hypothetical; recent outbreaks in schools across the globe highlight the real-world consequences of vaccine hesitancy.
Consider the 2019 measles outbreak in a New York school district, where a single case led to over 100 infections, primarily among unvaccinated children. This scenario underscores the concept of herd immunity, where a high vaccination rate (typically 93-95% for measles) creates a protective barrier, preventing diseases from spreading even to those who cannot be vaccinated due to medical reasons. Schools, by mandating vaccinations before entry, can significantly bolster this herd immunity, effectively shielding their student bodies and the surrounding community.
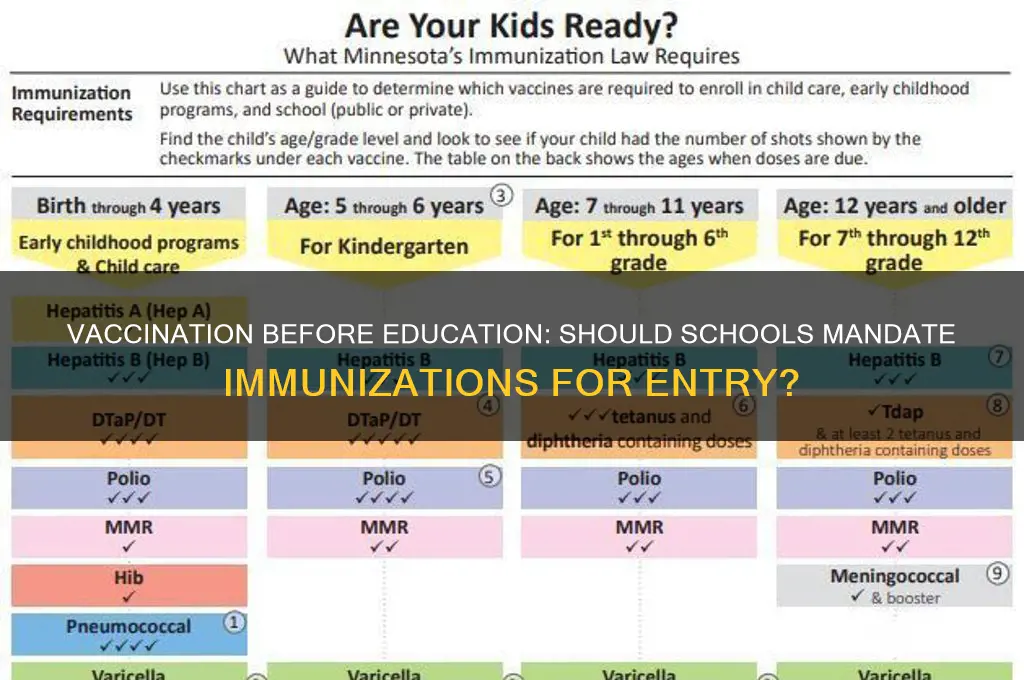
Implementing a school entry vaccination requirement involves a multi-step process. Firstly, schools must clearly communicate the required vaccinations, including specific doses and age-appropriate schedules. For instance, the MMR (measles, mumps, rubella) vaccine typically requires two doses, the first administered at 12-15 months and the second at 4-6 years. Schools should provide resources and partner with healthcare providers to ensure families have access to vaccinations, addressing potential barriers like cost or transportation.
While some argue that vaccination mandates infringe on personal freedom, the public health benefits outweigh these concerns. Schools have a responsibility to provide a safe learning environment, and preventing outbreaks of preventable diseases is a crucial aspect of this duty. Exemptions for medical reasons should be accommodated, but non-medical exemptions should be strictly limited to prevent erosion of herd immunity.
By prioritizing disease outbreak prevention through vaccination mandates, schools can create healthier learning environments, protect vulnerable populations, and contribute to the overall well-being of their communities. This proactive approach not only safeguards individual students but also strengthens the public health fabric, ensuring a safer future for all.
Donating Cash to Food Banks: A Step-by-Step Guide to Giving Back
You may want to see also
Explore related products






![]()
Equity in Access: Ensuring all children, regardless of background, receive necessary vaccinations
Vaccination rates among children often mirror socioeconomic disparities, with lower-income families facing barriers like cost, transportation, and lack of nearby healthcare providers. In the U.S., for instance, children in households below the federal poverty level are 20% less likely to receive all recommended vaccines by age 2 compared to their higher-income peers. This gap persists globally; in low-income countries, only 60% of infants receive basic immunizations, compared to 85% in high-income nations. Schools, as universal access points, can bridge this divide by requiring vaccinations for entry, but only if paired with equitable support systems.
Step 1: Identify Barriers to Access
Begin by mapping the obstacles families face. Financial constraints top the list, as vaccines themselves are often free in public programs, but associated costs (transportation, missed work wages) deter participation. Geographic isolation compounds this—rural families in Australia, for example, travel an average of 50 km to reach the nearest immunization clinic. Language and cultural barriers further exclude immigrant or non-English-speaking families, who may mistrust medical systems or lack awareness of vaccine schedules. Schools must collaborate with health departments to address these specific hurdles through targeted interventions.
Step 2: Implement School-Based Clinics and Mobile Units
On-site vaccination clinics during enrollment periods streamline access. In California, school-based health centers administered 40% of adolescent Tdap boosters in low-income districts after partnering with local clinics. Mobile units, like those used in Brazil’s *Caravana da Vacinação*, bring vaccines directly to underserved neighborhoods, achieving a 90% coverage rate among previously unreachable populations. Pair these efforts with multilingual staff and culturally sensitive communication to build trust. For instance, Somali communities in Minnesota saw a 15% increase in MMR uptake after health workers engaged community leaders to dispel myths.
Step 3: Leverage Technology and Incentives
Digital tools can overcome logistical barriers. SMS reminders, used in Kenya’s Afya Mama program, increased timely vaccination by 27%. Online portals for scheduling appointments or verifying immunization records reduce paperwork burdens. Incentives, such as small gifts (backpacks, school supplies) or waivers for school fees upon vaccination completion, have proven effective in pilot programs in India and South Africa. However, caution against punitive measures like denying enrollment, which disproportionately penalize vulnerable children and may violate ethical guidelines.
Caution: Avoid One-Size-Fits-All Solutions
Equity requires tailoring strategies to local contexts. Urban schools might prioritize after-school vaccination drives, while rural areas benefit more from weekend mobile clinics. Religious exemptions, though controversial, necessitate dialogue rather than coercion—in the Netherlands, engagement with Orthodox Jewish communities led to a 30% increase in uptake after addressing specific concerns. Always ensure policies comply with legal frameworks; for instance, the U.S.’s Individuals with Disabilities Education Act mandates accommodations for medically fragile students.
Requiring vaccinations for school entry is a powerful tool, but its success hinges on dismantling access barriers. By combining structural support (free clinics, transportation vouchers) with community engagement (trusted messengers, culturally tailored education), schools can ensure immunization becomes a right, not a privilege. The goal is not just compliance, but a generation protected from preventable diseases—regardless of zip code, income, or identity.
What Debt Collectors Does US Bank Use for Credit Card Accounts?
You may want to see also
Frequently asked questions
Many schools and health authorities require or strongly recommend vaccinations before entry to protect students and staff from preventable diseases, promote herd immunity, and ensure a safe learning environment.
Common vaccines required for school entry include measles, mumps, rubella (MMR), polio, diphtheria, tetanus, pertussis (DTaP), chickenpox, and hepatitis B, though requirements vary by region and school district.
Some regions allow exemptions for medical, religious, or philosophical reasons, but these exemptions are becoming more restricted due to public health concerns and outbreaks of vaccine-preventable diseases.
Yes, unvaccinated children are at higher risk of contracting and spreading vaccine-preventable diseases, which can lead to serious health complications or even death.
While some argue it infringes on parental rights, school vaccination requirements are generally upheld as a legitimate public health measure to protect the broader community, especially vulnerable individuals who cannot be vaccinated.