The question of whether vaccines should be made using tumor cells is a highly debated and complex issue in the field of immunotherapy and cancer research. Proponents argue that tumor cell-based vaccines can harness the immune system's ability to recognize and attack cancer cells, potentially offering a targeted and personalized treatment approach. These vaccines, often derived from a patient's own tumor or engineered to express specific cancer antigens, aim to stimulate an immune response against malignant cells while minimizing harm to healthy tissue. However, critics raise concerns about safety, efficacy, and ethical implications, including the risk of unintended immune reactions, the challenge of ensuring consistent vaccine quality, and the potential for tumor cells to mutate or evade immune detection. As research advances, balancing the promise of innovative cancer treatments with rigorous scientific and ethical scrutiny remains crucial in determining the viability of tumor cell-based vaccines.
| Characteristics | Values |
|---|---|
| Purpose | Tumor cell-based vaccines aim to stimulate the immune system to recognize and attack cancer cells by using whole tumor cells or their components. |
| Types | Autologous (patient-specific) tumor cell vaccines, Allogeneic (donor-derived) tumor cell vaccines, Genetically modified tumor cell vaccines. |
| Advantages | High immunogenicity due to multiple tumor-associated antigens (TAAs), Potential for personalized medicine, Can induce both humoral and cellular immune responses. |
| Challenges | Risk of tumor cell contamination or mutation, Limited scalability for autologous vaccines, Variability in antigen expression, Potential for immune tolerance rather than activation. |
| Current Research | Clinical trials exploring combinations with immune checkpoint inhibitors, Genetic engineering to enhance immunogenicity, Use of tumor cell lysates or mRNA-based approaches. |
| Ethical Considerations | Concerns about using tumor cells from donors, Informed consent for autologous vaccines, Balancing risks and benefits in clinical trials. |
| Regulatory Status | Limited approvals; most are in preclinical or clinical trial phases. Notable examples include Provenge (sipuleucel-T) for prostate cancer, which uses autologous antigen-presenting cells. |
| Efficacy | Mixed results; some studies show improved survival and immune responses, while others report limited clinical benefit. Efficacy depends on tumor type, vaccine formulation, and patient immune status. |
| Safety Profile | Generally considered safe, with mild to moderate side effects (e.g., fever, fatigue, injection site reactions). Rare cases of autoimmune reactions or disease progression have been reported. |
| Future Directions | Integration with immunotherapy (e.g., CAR-T cells, checkpoint inhibitors), Development of off-the-shelf tumor cell vaccines, Advances in bioengineering to improve antigen presentation and delivery. |
| Public Perception | Mixed; some concerns about safety and efficacy, but growing acceptance as research progresses and successes are highlighted. |
| Cost Implications | High production costs, especially for autologous vaccines, may limit accessibility. Economies of scale could reduce costs for allogeneic or standardized approaches. |
| Scientific Consensus | Tumor cell-based vaccines show promise but require further optimization and standardization. Combination therapies are likely the key to maximizing their potential. |
Explore related products






What You'll Learn
![]()
Ethical concerns of using tumor cells in vaccines
The use of tumor cells in vaccine development raises profound ethical questions, particularly regarding informed consent and the origins of these cells. Historically, some cancer cell lines, like HeLa, were derived without the donor’s knowledge or permission, sparking decades-long debates about autonomy and exploitation. When tumor cells are sourced for vaccines, ensuring transparent consent from donors or their families becomes critical. For instance, if a vaccine candidate relies on a cell line extracted decades ago under questionable ethical standards, its use today could perpetuate historical injustices. Researchers must establish rigorous protocols to trace cell origins and secure explicit consent, even for anonymized or archived samples. Without this, the ethical foundation of the vaccine is compromised, regardless of its medical potential.
Another ethical concern lies in the potential for tumor cell-based vaccines to cause unintended harm, such as oncogenic risks or immune system dysregulation. While these vaccines aim to train the immune system to recognize and attack cancer cells, the introduction of tumor-derived material into the body carries theoretical risks. For example, if a vaccine contains whole tumor cells or fragments, there is a remote possibility of genetic material from these cells integrating into the recipient’s genome, potentially triggering malignancy. Regulatory bodies like the FDA require extensive preclinical and clinical testing to mitigate such risks, but the public’s perception of safety often lags behind scientific assurance. Communicating these risks transparently, without undermining trust in vaccination, is a delicate balance that developers and health authorities must navigate.
The ethical implications extend to equity and access, particularly when tumor cell-based vaccines are developed for rare or geographically concentrated cancers. For instance, a vaccine targeting a cancer prevalent in low-income regions might be priced beyond the reach of those populations due to high development costs. This raises questions about the prioritization of profit over global health equity. Developers could explore mechanisms like tiered pricing or technology transfer agreements to ensure accessibility, but such solutions require international cooperation and ethical commitment. Without addressing these disparities, the use of tumor cells in vaccines risks exacerbating existing inequalities in healthcare.
Finally, the psychological and societal impact of using tumor cells in vaccines cannot be overlooked. For some, the idea of injecting material derived from cancer cells—even if thoroughly processed and safe—may evoke fear or discomfort. This perception could fuel misinformation campaigns, undermining public confidence in vaccines broadly. Proactive engagement with communities, including clear explanations of the science and safety measures, is essential. For example, educational campaigns could highlight how tumor cells are inactivated or engineered to eliminate their harmful potential, framing the vaccine as a tool of hope rather than a source of risk. Ethical vaccine development, in this context, requires not just scientific rigor but also empathy and effective communication.
Creative Guide to Crafting an Engaging Banking School Project
You may want to see also
Explore related products


$457.44 $549.99




![]()
Potential risks of tumor cell-based vaccines
Tumor cell-based vaccines, while promising in cancer immunotherapy, carry inherent risks that demand careful consideration. One primary concern is the potential for these vaccines to induce autoimmune reactions. Tumor cells often express antigens that are also present on healthy tissues, albeit at lower levels. When the immune system is primed to target these antigens, it may mistakenly attack normal cells, leading to autoimmune disorders. For instance, a vaccine targeting MUC1, a glycoprotein overexpressed in breast cancer, could theoretically trigger autoimmune responses in mucosal tissues, causing conditions like dry mouth or gastrointestinal inflammation. Patients with pre-existing autoimmune diseases, such as rheumatoid arthritis or lupus, may be at heightened risk and should be excluded from clinical trials unless closely monitored.
Another critical risk lies in the possibility of tumor cell mutation or contamination during vaccine production. Tumor cells used in vaccines are often irradiated or chemically treated to prevent their growth, but incomplete inactivation could allow residual cells to proliferate post-administration. This scenario, though rare, could theoretically lead to secondary tumor formation at the injection site or elsewhere. Additionally, contamination with pathogens or other tumor cell lines during manufacturing poses a significant hazard. Stringent quality control measures, including genomic sequencing and sterility testing, are essential to mitigate these risks. Regulatory bodies like the FDA require multiple rounds of testing, but even these protocols are not foolproof, as evidenced by historical cases of vaccine contamination.
The immunogenicity of tumor cell-based vaccines can also be unpredictable, particularly in older adults or immunocompromised individuals. Elderly patients, who constitute a significant portion of cancer patients, often exhibit immunosenescence, a decline in immune function that reduces vaccine efficacy. For example, a dose of 1x10^6 irradiated tumor cells, effective in younger patients, might fail to elicit a robust immune response in those over 65. Similarly, patients undergoing chemotherapy or radiation therapy may have suppressed immune systems, rendering the vaccine ineffective or even harmful. Tailoring vaccine dosages or combining them with immunomodulatory agents could address these challenges, but such strategies require extensive clinical validation.
Finally, the psychological and ethical implications of tumor cell-based vaccines cannot be overlooked. Patients may experience anxiety or reluctance upon learning that the vaccine contains tumor cells, even if they are inactivated. Clear, transparent communication about the vaccine’s composition, risks, and benefits is crucial to alleviate concerns. Ethically, the use of tumor cells derived from patients or cell lines raises questions about consent and ownership. For instance, the HeLa cell line, derived without consent, remains a contentious example. Ensuring informed consent and respecting donor autonomy are non-negotiable principles in the development and deployment of such vaccines.
In summary, while tumor cell-based vaccines hold immense potential, their risks—ranging from autoimmune reactions to contamination and unpredictable immunogenicity—require meticulous management. Practical steps, such as rigorous quality control, personalized dosing, and ethical oversight, can help navigate these challenges. However, ongoing research and transparent communication remain vital to ensuring these vaccines are both safe and effective.
Kickstart Your Banking Career: Post-12th Preparation Guide for Success
You may want to see also
Explore related products






![]()
Scientific feasibility of tumor cell vaccines
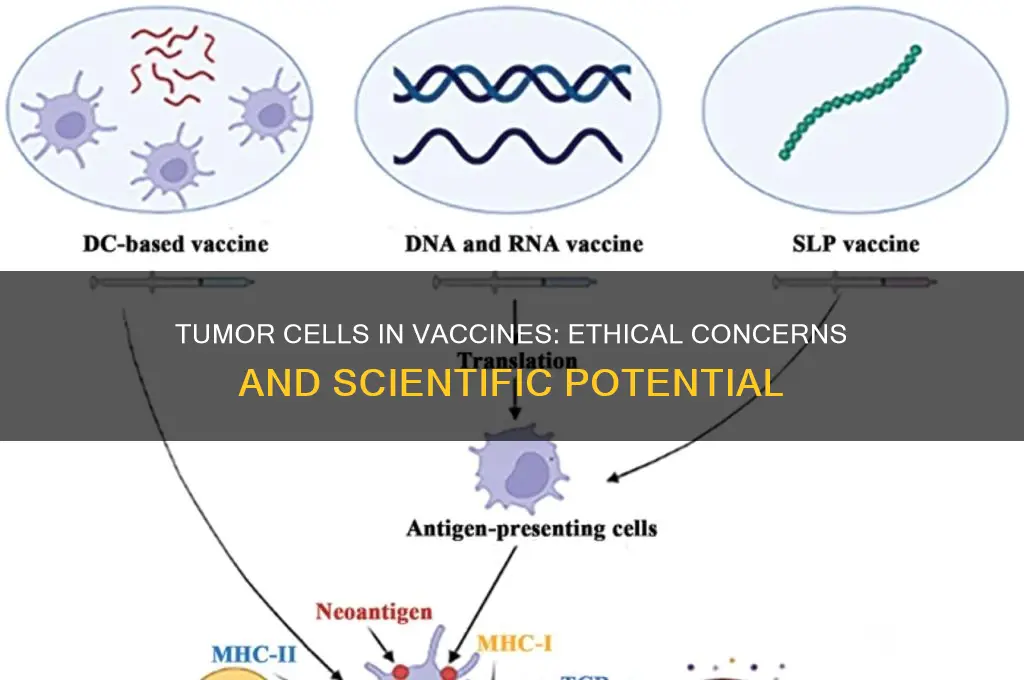
Tumor cell vaccines represent a promising frontier in cancer immunotherapy, leveraging the body’s immune system to target and destroy cancer cells. The scientific feasibility of these vaccines hinges on their ability to elicit a robust, specific immune response against tumor-associated antigens (TAAs). Unlike traditional vaccines that prevent infectious diseases, tumor cell vaccines aim to treat existing cancers by reprogramming the immune system to recognize and attack malignant cells. This approach requires precise engineering of vaccine components to ensure efficacy and safety, as tumor cells often evade immune detection through mechanisms like antigen downregulation or immunosuppression.
One critical challenge in developing tumor cell vaccines is identifying and isolating suitable antigens that are uniquely expressed by cancer cells. Advances in genomics and proteomics have enabled the discovery of neoantigens—mutated proteins specific to an individual’s tumor—which serve as ideal targets. For instance, personalized neoantigen vaccines, such as those developed by BioNTech and Moderna, use mRNA technology to encode multiple neoantigens, stimulating a tailored immune response. Clinical trials have demonstrated encouraging results, with some patients achieving durable remission in cancers like melanoma. However, scalability remains a hurdle, as individualized vaccines require extensive tumor sequencing and synthesis, limiting accessibility.
The manufacturing process for tumor cell vaccines also demands stringent quality control to ensure safety and consistency. Irradiated or chemically treated tumor cells are often used to prevent vaccine-induced tumor growth while preserving antigenicity. Adjuvants, such as Toll-like receptor agonists or cytokines, are frequently incorporated to enhance immunogenicity. For example, the vaccine OncoVax uses autologous tumor cells combined with the adjuvant dinitrophenyl (DNP) to amplify immune activation. Dosage optimization is critical; preclinical studies suggest that doses ranging from 10^6 to 10^7 cells per injection can balance efficacy and adverse effects, though this varies by cancer type and patient immune status.
Comparatively, tumor cell vaccines offer advantages over other immunotherapies like checkpoint inhibitors or CAR-T cell therapy, particularly in terms of specificity and reduced toxicity. However, their success depends on overcoming immune tolerance mechanisms that protect tumor cells from destruction. Combination therapies, such as pairing tumor cell vaccines with PD-1/PD-L1 inhibitors, have shown synergistic effects in preclinical models, enhancing T-cell infiltration and tumor regression. For instance, a phase II trial combining a whole-cell melanoma vaccine with pembrolizumab demonstrated improved overall survival rates compared to monotherapy.
In conclusion, the scientific feasibility of tumor cell vaccines is supported by technological advancements in antigen identification, vaccine engineering, and immunomodulation. While challenges remain, particularly in personalization and manufacturing, ongoing research continues to refine their design and application. Practical considerations, such as patient selection (e.g., prioritizing those with resected tumors or high mutational burden) and monitoring for immune-related adverse events, are essential for maximizing therapeutic benefit. As the field evolves, tumor cell vaccines hold significant potential to transform cancer treatment, offering a targeted, durable approach to combating malignancy.
Paying Your Mortgage at Alpine Bank: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Immunogenicity of vaccines made with tumor cells
Tumor cells, by their very nature, are masters of evasion, slipping past the immune system’s radar to proliferate unchecked. Yet, paradoxically, they hold a unique potential as vaccine components. When harnessed correctly, tumor cells can become potent immunogens, training the immune system to recognize and attack cancerous cells. The key lies in their antigenic profile—tumor cells express unique proteins, or neoantigens, that distinguish them from healthy cells. These neoantigens serve as red flags, signaling the immune system to mount a targeted response. However, the immunogenicity of tumor cell-based vaccines hinges on several critical factors, including the type of tumor cells used, the method of delivery, and the individual’s immune status.
To unlock the immunogenic potential of tumor cell vaccines, researchers often employ strategies to enhance their visibility to the immune system. One common approach is irradiation, which renders tumor cells non-viable while preserving their antigenic integrity. Irradiated tumor cells can then be combined with adjuvants, such as Toll-like receptor agonists or cytokines, to amplify the immune response. For instance, granulocyte-macrophage colony-stimulating factor (GM-CSF) has been widely used in clinical trials, demonstrating its ability to recruit and activate antigen-presenting cells. Dosage is critical here—a typical regimen might involve administering 1–2 million irradiated tumor cells per dose, combined with 125–250 micrograms of GM-CSF, delivered intradermally or subcutaneously every 1–2 weeks for 3–6 cycles.
A comparative analysis of tumor cell vaccines reveals their strengths and limitations. Unlike whole-cell vaccines, which may induce tolerance rather than immunity, genetically modified tumor cell vaccines offer greater control over immunogenicity. For example, tumor cells engineered to express costimulatory molecules like CD80 or 4-1BBL enhance T-cell activation, improving vaccine efficacy. However, this approach requires sophisticated genetic engineering techniques and raises concerns about safety and scalability. In contrast, autologous tumor cell vaccines, derived from a patient’s own tumor, offer a personalized approach but are labor-intensive and may not capture the full spectrum of neoantigens. Allogeneic tumor cell vaccines, sourced from a different individual, are more practical but risk reduced immunogenicity due to major histocompatibility complex (MHC) mismatches.
Practical considerations for implementing tumor cell vaccines include patient selection and monitoring. These vaccines are most effective in patients with minimal residual disease, as a lower tumor burden allows the immune system to act more efficiently. Additionally, combining tumor cell vaccines with checkpoint inhibitors, such as anti-PD-1 or anti-CTLA-4 antibodies, can overcome immune suppression in the tumor microenvironment. For instance, a phase II trial combining autologous tumor cell vaccines with ipilimumab (an anti-CTLA-4 antibody) in metastatic melanoma patients demonstrated a 20% objective response rate, compared to 10% with ipilimumab alone. Monitoring immune responses post-vaccination, through assays like enzyme-linked immunospot (ELISPOT) or tetramer staining, is essential to assess vaccine efficacy and tailor subsequent treatments.
In conclusion, the immunogenicity of tumor cell vaccines is a double-edged sword—while tumor cells inherently express neoantigens, their ability to evade immunity must be countered through strategic enhancements. From irradiation and adjuvant use to genetic engineering and combination therapies, each approach offers unique advantages and challenges. For clinicians and researchers, the key lies in balancing immunogenicity with practicality, ensuring that these vaccines not only stimulate robust immune responses but also remain accessible and safe for patients. As the field advances, tumor cell vaccines hold promise as a cornerstone of personalized cancer immunotherapy, turning the tables on cancer’s most cunning weapon.
Deactivating IOB Mobile Banking: A Step-by-Step Guide to Securely Disable Access
You may want to see also
Explore related products






![]()
Regulatory challenges for tumor cell-based vaccines
Tumor cell-based vaccines represent a promising frontier in cancer immunotherapy, leveraging the body’s immune system to target and destroy cancer cells. However, their development and approval face unique regulatory challenges that differ significantly from traditional vaccines. One of the primary hurdles is the inherent variability of tumor cells, which can mutate rapidly and differ widely between patients, even within the same cancer type. This biological complexity necessitates rigorous characterization and standardization of the vaccine product, a task that is both scientifically demanding and time-consuming.
Regulatory agencies, such as the FDA and EMA, require extensive preclinical and clinical data to ensure safety and efficacy. For tumor cell-based vaccines, this includes demonstrating the consistency of the manufacturing process, which often involves culturing autologous or allogeneic tumor cells. Unlike traditional vaccines, which use well-defined antigens, tumor cell-based vaccines must account for the heterogeneity of cancer cells. This requires advanced analytical techniques to confirm the presence of relevant tumor-associated antigens and the absence of contaminants. For instance, ensuring that the vaccine contains a minimum of 1x10^6 viable cells per dose while maintaining sterility is a critical manufacturing challenge.
Another regulatory challenge lies in defining appropriate clinical endpoints for trials. Traditional vaccines often measure antibody titers or infection rates, but tumor cell-based vaccines aim to induce a complex immune response that may not be easily quantifiable. Regulators must accept surrogate endpoints, such as overall survival or progression-free survival, which require larger and longer trials. For example, a Phase III trial for a melanoma vaccine might need to enroll hundreds of patients over several years to demonstrate a statistically significant improvement in survival rates.
Furthermore, the personalized nature of some tumor cell-based vaccines complicates regulatory approval. Autologous vaccines, tailored to an individual patient’s tumor, raise questions about scalability and cost-effectiveness. Regulators must balance the potential benefits of personalized medicine with the need for standardized, reproducible therapies. In contrast, allogeneic vaccines, derived from a donor tumor, offer greater scalability but require careful matching to minimize immune rejection. This duality demands flexible regulatory frameworks that can accommodate both approaches.
Finally, post-market surveillance poses additional challenges. Unlike traditional vaccines, which are administered to healthy individuals, tumor cell-based vaccines are given to patients with compromised immune systems. Monitoring for adverse events, such as autoimmune reactions or disease progression, requires robust pharmacovigilance systems. For instance, patients receiving a vaccine for pancreatic cancer should be closely monitored for signs of pancreatitis or systemic inflammation, with clear guidelines for dose interruption or discontinuation.
In summary, the regulatory landscape for tumor cell-based vaccines is fraught with complexities stemming from their biological variability, manufacturing challenges, clinical trial design, and post-market surveillance. Addressing these issues requires collaboration between researchers, manufacturers, and regulators to develop innovative solutions that ensure safety, efficacy, and accessibility for patients in need.
Is Your Bank Responsible for Poor IRA Investment Guidance?
You may want to see also
Frequently asked questions
Vaccines made with tumor cells, known as cancer vaccines, are being researched to treat or prevent certain cancers. While they show promise in personalized medicine, they are not yet widely used due to challenges like variability in tumor cells and immune response. Current vaccines are rigorously tested for safety and efficacy.
Vaccines using tumor cells are designed to target specific cancer antigens and are generally considered safe when used under clinical supervision. However, like any medical treatment, they may have side effects, and their safety depends on the specific formulation and individual health conditions.
There is no evidence that vaccines made with tumor cells cause cancer. These vaccines are engineered to stimulate the immune system to recognize and attack cancer cells, not to introduce new cancerous cells. Strict regulatory standards ensure their safety before clinical use.