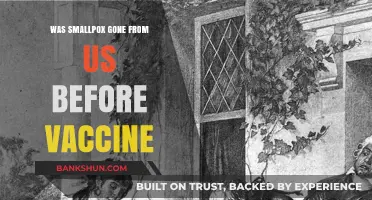
The polio vaccine, a groundbreaking medical achievement, was indeed administered in the form of a sugar cube during the mid-20th century. Developed by Dr. Albert Sabin, the oral polio vaccine (OPV) was a live but weakened version of the virus, delivered on a small, sugar-coated cube to make it more palatable, especially for children. This innovative method played a crucial role in the global effort to eradicate polio, as it was easy to distribute, required no needles, and encouraged widespread acceptance. The sugar cube vaccine became a symbol of hope and progress, contributing significantly to the dramatic decline in polio cases worldwide.
| Characteristics | Values |
|---|---|
| Vaccine Type | Oral Polio Vaccine (OPV) |
| Form | Sugar cube (sabin vaccine on a sugar cube) |
| Developer | Albert Sabin |
| Introduction Year | 1961 |
| Purpose | Mass vaccination campaigns to eradicate polio |
| Administration Method | Oral ingestion |
| Active Ingredient | Live attenuated poliovirus strains (Types 1, 2, and 3) |
| Storage | Required refrigeration until administration |
| Effectiveness | Highly effective in inducing immunity in the gut |
| Discontinuation | Largely phased out in favor of inactivated polio vaccine (IPV) due to rare vaccine-derived polio cases |
| Historical Impact | Played a crucial role in global polio eradication efforts |
| Current Use | Rarely used today; IPV is the preferred vaccine in most countries |
| Notable Campaigns | Widely used in the 1960s and 1970s, especially in developing countries |
| Side Effects | Generally safe; rare cases of vaccine-associated paralytic polio (VAPP) |
| Legacy | Symbol of successful public health initiatives in the 20th century |
Explore related products






What You'll Learn
![]()
Origins of the Sugar Cube Vaccine
The sugar cube vaccine, a symbol of hope in the fight against polio, emerged in the late 1950s as a revolutionary method to administer the oral polio vaccine (OPV). Developed by Dr. Albert Sabin, the OPV was a live, attenuated vaccine that could be easily delivered without the need for needles, making it ideal for mass immunization campaigns. The sugar cube, a familiar and palatable medium, became the vehicle of choice for this vaccine, transforming the way children received protection against a debilitating disease. This method was not only innovative but also culturally significant, as it turned a medical intervention into a simple, almost celebratory act.
To understand the origins of the sugar cube vaccine, one must consider the context of the polio epidemic. In the mid-20th century, polio was a feared disease, particularly among children, causing paralysis and even death. The development of the OPV was a breakthrough, but its success relied on widespread distribution. The sugar cube method was introduced in 1961 as part of the Sabin Vaccine Program, initially in the United States and later globally. Each sugar cube was impregnated with a measured dose of the vaccine—typically 0.1 mL—ensuring consistency and ease of administration. Parents were instructed to give the cube to their children, who would consume it like a treat, often without realizing it was medicine.
The choice of sugar cubes as the delivery mechanism was both practical and strategic. Sugar was inexpensive, widely available, and appealing to children, increasing compliance among young recipients. The cubes were also easy to transport and store, which was crucial for reaching remote or underserved communities. For example, during the 1962–1963 campaign in the United States, over 20 million children received the vaccine via sugar cubes in just two rounds of distribution. This method not only facilitated mass immunization but also helped normalize the vaccine, reducing fear and resistance among parents and children alike.
However, the sugar cube vaccine was not without its challenges. Ensuring the vaccine’s stability within the sugar cube required precise manufacturing techniques, as the live virus had to remain viable during storage and transportation. Additionally, the method was less suitable for infants under two years old, who were at higher risk of polio but often unable to safely consume the cube. In such cases, alternative methods, like drops, were used. Despite these limitations, the sugar cube vaccine played a pivotal role in the global eradication efforts, particularly in the Americas, where polio cases plummeted in the decades following its introduction.
In retrospect, the sugar cube vaccine represents a unique intersection of medical innovation and public health strategy. It exemplifies how creativity in delivery methods can overcome logistical and psychological barriers to vaccination. While the sugar cube is no longer the primary method for administering the OPV—liquid drops are now more common—its legacy endures as a testament to the power of simplicity in saving lives. For those interested in replicating the method for educational or historical purposes, it’s important to note that the original process involved soaking the cubes in a vaccine solution for a specific duration, ensuring even distribution of the virus. This detail underscores the meticulous planning behind what appeared to be a straightforward solution.
European Bank Transfers: Understanding Processing Times and Delays
You may want to see also
Explore related products






![]()
Sabin Oral Polio Vaccine (OPV) Development
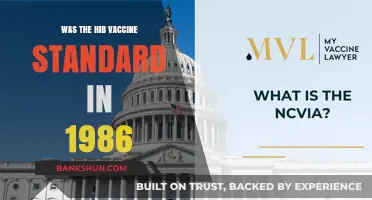
The Sabin Oral Polio Vaccine (OPV) revolutionized polio eradication efforts by offering a simple, needle-free solution that could be administered to children as young as 6 weeks old. Developed by Dr. Albert Sabin in the late 1950s, OPV was a live-attenuated vaccine delivered on a sugar cube, making it both palatable and easy to distribute. This method was particularly effective in mass vaccination campaigns, as it required no medical expertise to administer and eliminated the need for sterile needles or syringes. The sugar cube not only masked the vaccine’s taste but also made the experience less intimidating for children, increasing compliance in global immunization drives.
From a logistical standpoint, the OPV’s sugar cube delivery system was a game-changer. Each cube contained approximately 0.1 mL of the vaccine, a precise dose that ensured efficacy while minimizing waste. The vaccine’s stability at room temperature for short periods further facilitated its use in remote or resource-limited areas. However, administering OPV required careful handling: the sugar cube had to be fully saturated with the vaccine and consumed within minutes to maintain potency. Health workers were trained to ensure the cube dissolved completely in the child’s mouth, as spitting or incomplete ingestion could reduce effectiveness.
Comparatively, OPV’s oral route offered distinct advantages over the earlier inactivated polio vaccine (IPV), which required injection. While IPV provided individual protection, OPV induced both humoral and intestinal immunity, reducing viral shedding and transmission in communities. This dual benefit made OPV the preferred choice for global eradication efforts, particularly in regions with high polio prevalence. However, the live nature of OPV carried a rare risk of vaccine-associated paralytic polio (VAPP), occurring in approximately 1 in 2.7 million doses. This risk, though minimal, led to the eventual shift back to IPV in many countries once polio incidence declined.
For parents and caregivers, administering OPV was straightforward but required adherence to specific guidelines. Children typically received a series of 3–4 doses, starting at 6–8 weeks of age, with intervals of 4–8 weeks between doses. The vaccine could be given regardless of feeding status, making it convenient for busy families. However, it was crucial to avoid giving OPV with hot foods or liquids, as heat could inactivate the virus. Additionally, children with immunodeficiencies or those living with HIV were advised to receive IPV instead, due to the risk of VAPP.
In conclusion, the Sabin OPV’s sugar cube delivery was a masterstroke in public health innovation, combining simplicity, accessibility, and effectiveness. Its development marked a turning point in the fight against polio, enabling mass immunization campaigns that drastically reduced global incidence. While the sugar cube method is no longer widely used due to advancements in vaccine delivery, its legacy endures as a testament to the power of creative solutions in tackling infectious diseases. Understanding OPV’s history and mechanics offers valuable insights for future vaccine development, particularly in low-resource settings.
Easy Steps to Save Your Vaccine Receipt on Your Phone
You may want to see also
Explore related products






![]()
Mass Immunization Campaigns in the 1960s
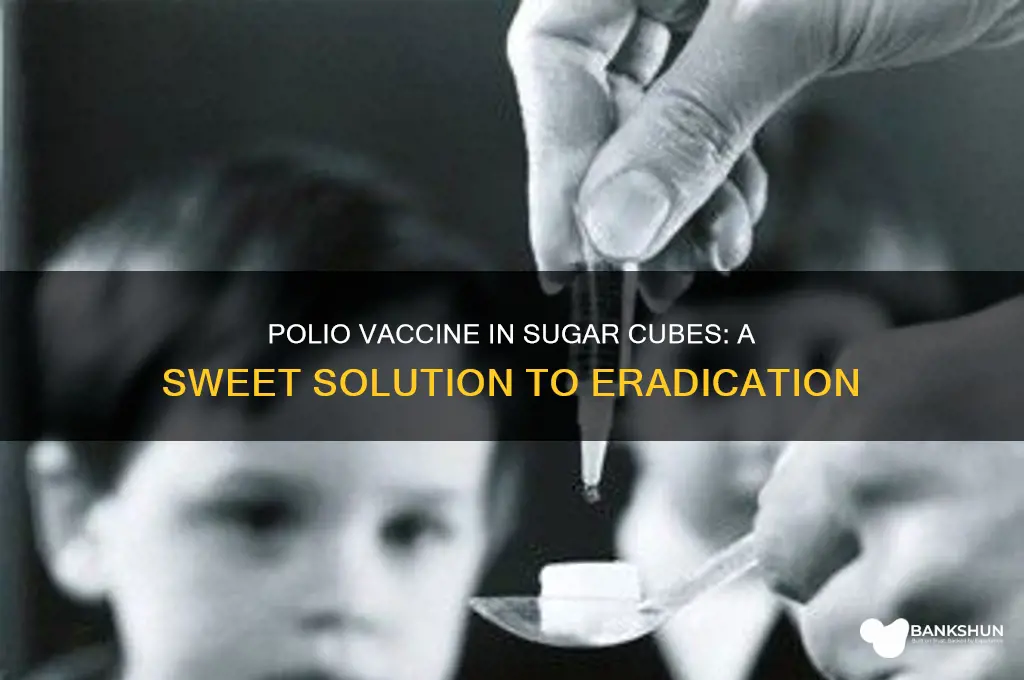
The 1960s marked a pivotal era in public health with the widespread rollout of mass immunization campaigns against polio, a disease that had terrorized families worldwide. Central to this effort was the oral polio vaccine (OPV), delivered in a form both ingenious and accessible: a sugar cube. Developed by Dr. Albert Sabin, the OPV was a live-attenuated vaccine that could be administered orally, making it ideal for large-scale campaigns. The sugar cube, impregnated with the vaccine, not only masked the taste but also simplified distribution, especially in areas with limited medical infrastructure. This innovation turned vaccination into a communal event, often held in schools, clinics, and public squares, where children lined up to receive their dose of protection.
To understand the impact of these campaigns, consider the logistics involved. The vaccine required no needles, refrigeration, or highly trained personnel, making it a game-changer for global health. Each sugar cube contained approximately 1 million plaque-forming units of the vaccine, a precise dosage that ensured efficacy while minimizing risks. Parents were instructed to ensure their children, typically aged 2 to 5, consumed the entire cube without chewing, as this could reduce the vaccine’s effectiveness. The simplicity of this method allowed for rapid immunization, with millions vaccinated in a matter of weeks. For instance, the United States saw over 20 million children immunized in a single year, drastically reducing polio cases from thousands annually to mere dozens by the decade’s end.
However, the success of these campaigns was not without challenges. Public trust was critical, and health officials employed creative strategies to encourage participation. Posters, radio broadcasts, and community leaders were enlisted to dispel myths and emphasize the vaccine’s safety. In some regions, the sugar cube became a symbol of hope, with children proudly showing off their participation badges or stickers. Yet, logistical hurdles persisted, particularly in rural or conflict-affected areas. Ensuring the vaccine’s viability during transport and storage, even without refrigeration, required meticulous planning. The use of portable coolers and timed distribution schedules became standard practices to maintain the vaccine’s potency.
Comparatively, the sugar cube method stood in stark contrast to the earlier inactivated polio vaccine (IPV), which required injection and was more resource-intensive. While IPV remained in use, particularly in wealthier nations, OPV’s oral delivery democratized access to immunization. This shift exemplified a broader trend in public health: adapting medical solutions to meet the needs of diverse populations. The sugar cube campaigns demonstrated that effective health interventions need not be complex—they must be practical, scalable, and culturally sensitive.
In retrospect, the mass immunization campaigns of the 1960s were a triumph of innovation and collaboration. They not only eradicated polio as a public health threat in many countries but also set a precedent for future vaccination drives, such as those against measles and COVID-19. The sugar cube, a humble vehicle for the polio vaccine, remains a powerful reminder of how simplicity and creativity can transform global health outcomes. For those planning or participating in immunization efforts today, the lessons are clear: prioritize accessibility, build trust, and tailor solutions to the communities they serve.
High-Risk Businesses: Identifying Industries Banks Approach with Caution
You may want to see also
Explore related products






![]()
Effectiveness and Public Acceptance of Sugar Cube Vaccine
The sugar cube delivery method for the polio vaccine, pioneered in the 1960s, was a masterclass in public health innovation. This simple, palatable approach addressed a critical challenge: administering a live, attenuated vaccine (Sabin vaccine) orally. The sugar cube acted as both a stabilizer for the vaccine and a vehicle for easy, painless delivery, particularly appealing to children. This method played a pivotal role in the global eradication efforts, contributing to a dramatic decline in polio cases worldwide.
A single sugar cube, typically containing 0.1 mL of the vaccine solution, provided a sufficient dose for immunity. The recommended age for vaccination was 6 weeks and older, with a series of doses administered over several months. This approach not only ensured widespread coverage but also fostered public trust, as the sugar cube made the vaccination process less intimidating.
However, the sugar cube's success wasn't solely due to its sweetness. Its effectiveness relied on a combination of factors. The Sabin vaccine's oral administration stimulated mucosal immunity, providing a robust defense against the poliovirus. The sugar cube's absorbency ensured the vaccine remained viable during storage and transportation, even in areas with limited refrigeration. This made it ideal for mass vaccination campaigns, reaching remote populations where traditional injection methods were impractical.
Moreover, the sugar cube's familiarity and accessibility played a crucial role in public acceptance. Unlike injections, which can be feared or stigmatized, the sugar cube was a familiar treat, making vaccination a more positive experience, especially for children. This psychological aspect cannot be understated, as public trust and participation are essential for any vaccination program's success.
Despite its undeniable impact, the sugar cube method wasn't without limitations. The live, attenuated vaccine carried a minuscule risk of vaccine-derived poliovirus, a concern in areas with low vaccination rates. Additionally, the sugar cube's stability was temperature-dependent, requiring careful handling and storage. These factors led to the gradual transition to more modern delivery methods, such as oral drops, which offered similar convenience with improved safety profiles.
In conclusion, the sugar cube vaccine stands as a testament to the power of innovative thinking in public health. Its effectiveness in polio eradication was multifaceted, combining scientific ingenuity with a deep understanding of human behavior. While no longer the primary method, its legacy continues to inspire new approaches to vaccine delivery, reminding us that sometimes, the sweetest solutions are the most effective.
Provident Bank of Ohio's Evolution: A Journey to Its Current Identity
You may want to see also
Explore related products






![]()
Transition from Sugar Cube to Liquid Drops
The polio vaccine's journey from sugar cube to liquid drops marks a significant shift in vaccine administration, driven by practicality, cost, and evolving medical standards. Initially, the Sabin oral polio vaccine (OPV) was delivered on a sugar cube, a method chosen for its simplicity and palatability, especially for children. This approach, introduced in the 1960s, revolutionized mass vaccination campaigns, making it easier to distribute and administer the vaccine globally. However, the sugar cube method had limitations, including variability in vaccine dosage due to uneven absorption and the logistical challenges of storing and transporting sugar cubes.
Transitioning to liquid drops addressed these issues by standardizing dosage and simplifying distribution. The liquid form of OPV, typically administered in 0.1 mL doses for infants and young children, ensures precise delivery using a dropper or syringe. This method eliminates the need for a physical medium like sugar, reducing costs and minimizing the risk of contamination. Health workers can now carry vials of the vaccine, making it more accessible in remote or resource-limited areas. The shift also aligns with modern vaccine delivery practices, which prioritize efficiency and accuracy.
From a practical standpoint, the liquid drop method offers flexibility in administration. Parents and caregivers can easily administer the vaccine at home, following simple instructions: tilt the child’s head back slightly, place the drops into their mouth, and ensure they swallow. For infants, the vaccine is often given between 6 weeks and 4 years of age, with multiple doses spaced 4–8 weeks apart to build immunity. This approach has been instrumental in global polio eradication efforts, as it allows for rapid vaccination of large populations during outbreaks.
Despite its advantages, the transition to liquid drops required public education to overcome familiarity with the sugar cube method. Campaigns emphasized the safety, efficacy, and convenience of the new format, reassuring parents and healthcare providers. The liquid form also allowed for easier integration with other oral vaccines, streamlining immunization schedules. Today, the liquid drop method remains a cornerstone of polio vaccination, reflecting how innovation in vaccine delivery can enhance public health outcomes.
In conclusion, the shift from sugar cube to liquid drops exemplifies how small changes in vaccine administration can have far-reaching impacts. By prioritizing precision, cost-effectiveness, and ease of use, this transition has played a crucial role in the fight against polio. It serves as a reminder that the delivery method is just as important as the vaccine itself in ensuring widespread protection.
Accessing the West Bank: Essential Entry Requirements and Travel Tips
You may want to see also
Frequently asked questions
Yes, the oral polio vaccine (OPV) developed by Albert Sabin was often administered on a sugar cube to make it more palatable, especially for children.
The sugar cube was used as a convenient and child-friendly way to deliver the oral polio vaccine, which was in liquid form, ensuring accurate dosage and making the experience less intimidating.
The sugar cube method was widely used in the 1960s and 1970s during mass vaccination campaigns, particularly in the United States and other countries, to eradicate polio.
No, the sugar cube method is no longer used. Modern oral polio vaccines are typically administered via drops directly into the mouth or on a spoon.
No, the sugar cube was merely a vehicle to deliver the vaccine. The actual vaccine was a liquid that was absorbed into the sugar cube before being given to the recipient.