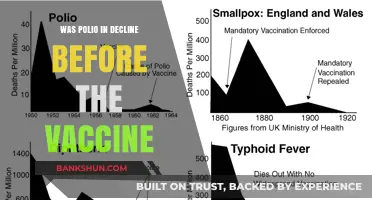
The 1950s marked a pivotal era in public health with the development and distribution of the polio vaccine, a breakthrough that promised to end the crippling disease that had terrified communities worldwide. As the vaccine became widely available, questions arose about its implementation, particularly whether it should be mandatory. While the polio vaccine was not federally mandated in the United States during the 1950s, its adoption was strongly encouraged through public health campaigns and local initiatives. Schools and institutions often required vaccination as a condition for attendance, effectively making it mandatory in practice for many children. This period highlighted the tension between individual choice and collective health, setting a precedent for future vaccination policies.
| Characteristics | Values |
|---|---|
| Mandatory Status in 1950s | Not universally mandatory; decisions were made at state or local levels. |
| Federal Mandate | No federal mandate existed for the polio vaccine in the 1950s. |
| State/Local Mandates | Some states or localities implemented school-entry requirements. |
| Public Acceptance | High public demand due to polio outbreaks; voluntary uptake was common. |
| Vaccine Availability | Jonas Salk's inactivated polio vaccine (IPV) was licensed in 1955. |
| Legal Framework | Vaccination laws varied; no standardized national policy. |
| Impact on School Attendance | Local mandates often tied vaccination to school enrollment. |
| Public Health Campaigns | Extensive campaigns promoted vaccination but did not enforce it federally. |
| Historical Context | Polio outbreaks in the 1950s spurred widespread vaccination efforts. |
| Long-Term Effect | Laid groundwork for future vaccine mandates and public health policies. |
Explore related products






What You'll Learn
- Polio Outbreaks and Public Fear: Widespread epidemics fueled demand for vaccination and potential mandatory policies
- Vaccine Development Timeline: Salk’s vaccine (1955) and Sabin’s (1960s) shaped immunization strategies globally
- Government Policies: Some regions mandated polio vaccines for school entry or public health
- Public Resistance: Anti-vaccine sentiments and skepticism challenged mandatory vaccination efforts
- Global Vaccination Campaigns: International efforts aimed to eradicate polio through widespread immunization
![]()
Polio Outbreaks and Public Fear: Widespread epidemics fueled demand for vaccination and potential mandatory policies
The polio outbreaks of the early to mid-20th century were not just medical crises but societal upheavals that reshaped public attitudes toward disease prevention. Between the 1940s and 1950s, polio cases surged in the United States, with over 57,000 reported in 1952 alone. These epidemics paralyzed not only bodies but also communities, as parents lived in terror of their children contracting the virus. Swimming pools, movie theaters, and schools closed during peak seasons, and public gatherings were often canceled. This widespread disruption fueled a collective desperation for a solution, setting the stage for the polio vaccine to become one of the most eagerly anticipated medical breakthroughs in history.
The fear of polio was deeply personal and pervasive, amplified by its unpredictable nature. Unlike other diseases, polio struck without warning, often affecting healthy children and young adults. The iron lung, a symbol of the disease’s severity, became a haunting image in newspapers and newsreels, driving home the urgency of finding a cure. Public health campaigns, such as the March of Dimes, capitalized on this fear, raising millions of dollars for research and fostering a sense of shared responsibility. By the time Jonas Salk’s inactivated polio vaccine (IPV) was declared safe and effective in 1955, the public was primed to embrace it, not just as a medical advancement but as a societal imperative.
The demand for the polio vaccine was so intense that it outpaced production capabilities, leading to innovative distribution strategies. The vaccine was initially administered in three doses, with the first dose providing partial immunity and the third offering near-complete protection. Schools became vaccination hubs, with children lining up in gymnasiums to receive their shots. However, the sheer scale of the rollout highlighted logistical challenges, such as ensuring proper refrigeration for the vaccine and managing public expectations. Despite these hurdles, within a year of its release, over 40 million Americans had received at least one dose, a testament to both the vaccine’s effectiveness and the public’s eagerness to end the polio menace.
While the polio vaccine was not federally mandated in the 1950s, its widespread adoption was driven by a combination of public fear and grassroots advocacy. Local health departments and school districts often required proof of vaccination for attendance, effectively making it a de facto requirement for social participation. This approach mirrored the success of earlier mandatory vaccination campaigns, such as those for smallpox, but relied more on community pressure than legal enforcement. The polio vaccine’s rapid integration into routine childhood immunizations set a precedent for future public health initiatives, demonstrating the power of public demand in shaping medical policy.
The legacy of the polio outbreaks and the subsequent vaccination campaign offers a critical lesson for modern public health: fear, when channeled constructively, can drive unprecedented cooperation. However, it also underscores the importance of transparency and accessibility in vaccine distribution. For instance, ensuring that vaccination sites are conveniently located and that information is communicated clearly can mitigate hesitancy and logistical barriers. Today, as we confront new infectious diseases, the polio era reminds us that addressing public fear with actionable solutions is key to fostering trust and achieving widespread immunity.
Is the World Bank an Aid Organization? Unveiling Its Role and Impact
You may want to see also
Explore related products






![]()
Vaccine Development Timeline: Salk’s vaccine (1955) and Sabin’s (1960s) shaped immunization strategies globally
The development of polio vaccines in the mid-20th century marked a turning point in global public health, but their mandatory status in the 1950s varied widely by region. While the United States and some European countries embraced voluntary vaccination campaigns, others, like the Soviet Union, implemented stricter measures. This context is crucial for understanding how Jonas Salk’s inactivated poliovirus vaccine (IPV) in 1955 and Albert Sabin’s oral poliovirus vaccine (OPV) in the 1960s reshaped immunization strategies worldwide.
Salk’s vaccine, introduced in 1955, was administered via injection and required multiple doses to confer immunity. Typically, children received an initial series of three shots, spaced over several months, followed by booster doses. This vaccine was highly effective in preventing paralytic polio but did not stop asymptomatic transmission. Its success hinged on widespread adoption, which was facilitated by public trust in medical science and large-scale vaccination drives. For instance, the March of Dimes campaign in the U.S. played a pivotal role in funding research and promoting vaccination, though mandates were rare.
In contrast, Sabin’s oral vaccine, licensed in the 1960s, revolutionized polio immunization. Delivered as drops or on a sugar cube, it was easier to administer, particularly in low-resource settings. A single dose provided robust immunity, and the vaccine reduced viral shedding, curbing community transmission. This made OPV the cornerstone of global eradication efforts. Countries like India and Brazil adopted mass vaccination campaigns, often with mandatory components, to achieve high coverage rates. The simplicity and efficacy of Sabin’s vaccine underscored the importance of accessibility in immunization strategies.
The interplay between these vaccines highlights a shift from individual protection to community-wide immunity. Salk’s IPV laid the groundwork for public acceptance of vaccination, while Sabin’s OPV provided the tools to interrupt polio transmission globally. This dual approach informed later immunization programs, such as those for measles and COVID-19, emphasizing the need for both effective vaccines and strategic deployment.
Practical takeaways from this timeline include the importance of tailoring vaccine delivery to local contexts and leveraging public-private partnerships for success. For parents today, understanding this history underscores the value of timely vaccination schedules and the role of herd immunity in protecting vulnerable populations. While polio mandates were not universal in the 1950s, the legacy of Salk and Sabin’s vaccines demonstrates how innovation and collaboration can transform global health outcomes.
Mastering the Path to Becoming a Bank President: Strategies and Insights
You may want to see also
Explore related products






![]()
Government Policies: Some regions mandated polio vaccines for school entry or public health
In the 1950s, as the polio vaccine became widely available, governments faced a critical decision: how to ensure widespread immunization without overstepping individual freedoms. Some regions adopted mandatory policies, tying vaccination to school entry or public health participation. For instance, in the United States, states like New York and California required proof of polio vaccination for children enrolling in public schools. This approach leveraged the existing school system to reach a vulnerable population—children under 15, who accounted for over 50% of polio cases. The mandate typically applied to children aged 5 to 9, with a standard dosage of 0.5 mL of the inactivated poliovirus vaccine (IPV) administered in a series of three shots over 6 to 12 months.
Analyzing these policies reveals a strategic balance between public health goals and practical implementation. Mandates were often accompanied by public education campaigns, emphasizing the vaccine’s safety and efficacy. For example, health departments distributed informational pamphlets and held community meetings to address parental concerns. However, enforcement varied; some regions allowed medical or religious exemptions, while others took a stricter approach. In Sweden, a similar mandate led to a 90% vaccination rate within two years, demonstrating the policy’s effectiveness when paired with accessible healthcare infrastructure.
From a persuasive standpoint, these mandates were not merely about compliance but about collective responsibility. Polio was a highly contagious disease with no cure, and vaccination was the only proven prevention method. By requiring immunization for school entry, governments protected not only vaccinated children but also those who could not receive the vaccine due to medical reasons. This concept of herd immunity became a cornerstone of public health policy, influencing future vaccination strategies for diseases like measles and mumps.
Comparatively, regions without mandatory policies often struggled to achieve similar vaccination rates. In the UK, where vaccination was voluntary, uptake was slower, and polio outbreaks persisted into the 1960s. This contrast highlights the role of government intervention in accelerating disease eradication. However, it also underscores the importance of trust in public health systems; mandates were most successful when citizens understood the rationale behind them and had access to reliable healthcare services.
Practically, implementing such policies required careful planning. Schools became de facto vaccination hubs, with on-site clinics offering doses during enrollment periods. Parents were instructed to bring their child’s immunization records or schedule vaccinations through local health departments. For families in rural areas, mobile clinics were deployed to ensure accessibility. These logistical efforts were critical to the success of mandatory policies, turning theoretical mandates into actionable public health measures.
Exploring the Possibility of a Rheumatic Fever Vaccine: What We Know
You may want to see also
Explore related products






![]()
Public Resistance: Anti-vaccine sentiments and skepticism challenged mandatory vaccination efforts
The polio vaccine, a groundbreaking medical achievement, faced significant public resistance in the 1950s despite its potential to eradicate a debilitating disease. This skepticism wasn't merely a fringe movement; it reflected deep-seated fears and mistrust that challenged the very concept of mandatory vaccination.
One major source of resistance stemmed from a lack of understanding about the vaccine's development and potential side effects. The rapid rollout of the Salk vaccine, while a testament to scientific progress, left some feeling uneasy. Rumors and misinformation spread, often fueled by sensationalized media reports, amplifying concerns about potential risks. This highlights the crucial need for transparent communication and public education during the introduction of any new medical intervention.
Imagine a parent, bombarded with conflicting information, grappling with the decision to vaccinate their child. They hear whispers of potential long-term effects, yet witness the devastating impact of polio firsthand. This internal struggle exemplifies the complex emotional landscape navigated by many during this time.
Anti-vaccine sentiments weren't solely rooted in fear of the unknown. Historical context played a significant role. Past medical experiments, particularly those conducted on marginalized communities, had left a legacy of mistrust towards the medical establishment. This distrust, coupled with a general skepticism towards government mandates, created fertile ground for resistance.
To effectively address this resistance, public health officials needed to acknowledge these historical grievances and engage in open dialogue. Building trust required not just scientific data but also empathy and a willingness to address legitimate concerns.
The polio vaccine's story serves as a cautionary tale. While mandatory vaccination can be a powerful tool in disease prevention, its success hinges on public trust and informed consent. By understanding the roots of resistance and addressing them head-on, we can foster a more receptive environment for future medical advancements. This involves transparent communication, community engagement, and a commitment to ethical practices that prioritize individual autonomy alongside public health goals.
Should Banks Have the Right to Refuse Service to Customers?
You may want to see also
Explore related products






![]()
Global Vaccination Campaigns: International efforts aimed to eradicate polio through widespread immunization
The 1950s marked a pivotal era in the fight against polio, a disease that had long terrorized communities worldwide, leaving children paralyzed or worse. While the polio vaccine itself wasn’t universally mandatory during this decade, the development and distribution of Jonas Salk’s inactivated polio vaccine (IPV) in 1955 sparked an unprecedented global vaccination campaign. This effort laid the groundwork for international collaboration in disease eradication, blending scientific innovation with public health strategy. Countries like the United States, Canada, and parts of Europe rapidly adopted the vaccine, though its rollout varied in terms of accessibility and enforcement. The success of these early campaigns demonstrated the power of widespread immunization, setting a precedent for future global health initiatives.
One of the most striking aspects of the polio vaccination drive was its reliance on mass immunization programs. In the U.S., for instance, the March of Dimes played a crucial role in funding research and distributing the vaccine, ensuring that millions of children received their doses. Schools and community centers became hubs for vaccination clinics, with children as young as 6 months receiving the initial series of three shots, spaced over several months. In developing nations, however, logistical challenges such as refrigeration requirements for the IPV and limited healthcare infrastructure slowed progress. This disparity highlighted the need for international cooperation, leading to the formation of organizations like the World Health Organization’s (WHO) Expanded Programme on Immunization in the 1970s, which aimed to standardize vaccine delivery globally.
The transition from Salk’s IPV to Albert Sabin’s oral polio vaccine (OPV) in the early 1960s further revolutionized global vaccination efforts. OPV, administered as drops, was cheaper, easier to distribute, and didn’t require needles, making it ideal for mass campaigns in low-resource settings. By the 1980s, countries like India and Brazil began implementing door-to-door vaccination drives, targeting children under 5 years old. These campaigns often included supplementary doses of vitamin A to boost immunity, showcasing the integration of multiple health interventions. The success of OPV in reducing polio cases by 99% globally underscored the importance of adaptable, context-specific strategies in disease eradication.
Despite these advancements, challenges persisted. Vaccine hesitancy, fueled by misinformation and cultural barriers, threatened to derail progress in some regions. In Nigeria, for example, rumors that the polio vaccine was a Western plot to sterilize Muslim children led to a boycott in the early 2000s, causing a resurgence of the disease. Addressing such concerns required culturally sensitive communication strategies, involving local leaders and community health workers. The lessons learned from these setbacks emphasized the need for trust-building and education as integral components of global vaccination campaigns.
Today, the legacy of the 1950s polio vaccination efforts lives on in the Global Polio Eradication Initiative (GPEI), launched in 1988. This partnership between WHO, UNICEF, Rotary International, and others has reduced polio cases by 99.9% worldwide, with only a handful of countries still reporting wild poliovirus transmission. The initiative’s success hinges on its multi-pronged approach: routine immunization, supplementary vaccination campaigns, surveillance, and outbreak response. Practical tips for modern campaigns include ensuring cold chain integrity for vaccine storage, training healthcare workers in remote areas, and leveraging digital tools for real-time monitoring. As the world inches closer to polio eradication, the lessons from the 1950s remain clear: global collaboration, innovation, and persistence are the keys to conquering infectious diseases.
Vaccine Decision Dilemma: Weighing Risks, Benefits, and Personal Health Choices
You may want to see also
Frequently asked questions
The polio vaccine was not federally mandated in the 1950s, but many states and local school districts implemented vaccination requirements for children to attend public schools.
No, not all schools required the polio vaccine in the 1950s. Requirements varied by state and local jurisdiction, with some mandating vaccination and others leaving it optional.
Yes, exemptions existed in some areas for medical, religious, or personal reasons, though the availability and criteria for exemptions varied widely depending on local policies.
The polio vaccine was widely accepted by the public in the 1950s due to the devastating impact of polio outbreaks. However, there were still pockets of skepticism and resistance, particularly in the early years of its introduction.