The question of whether the polio vaccine was mandatory in the 1980s reflects a broader historical context of public health policies and societal attitudes toward vaccination. By the 1980s, polio had been largely eradicated in many developed countries thanks to widespread immunization efforts, particularly through the introduction of the Salk and Sabin vaccines in the 1950s and 1960s. While the polio vaccine was not universally mandated by federal law in the United States during this period, many states and school districts required proof of vaccination for children to attend public schools, effectively making it a de facto requirement. This approach aimed to maintain high vaccination rates and prevent outbreaks, ensuring herd immunity. Globally, the situation varied, with some countries implementing stricter mandatory vaccination policies as part of their public health strategies. The 1980s also marked a pivotal phase in the World Health Organization’s (WHO) global polio eradication initiative, which further emphasized the importance of vaccination, though mandates were often tailored to regional needs and challenges.
| Characteristics | Values |
|---|---|
| Mandatory Status in 1980s (USA) | Not federally mandated, but required by many states for school entry |
| Global Mandate in 1980s | Varied by country; some nations had mandatory policies, while others relied on strong recommendations |
| WHO's Role in 1980s | Launched the Global Polio Eradication Initiative in 1988, promoting widespread vaccination but not enforcing mandates |
| Public Perception in 1980s | Generally high acceptance due to polio's historical impact, with minimal organized opposition |
| Legal Framework (USA) | States had authority to set vaccination requirements, leading to variability in mandates |
| Vaccination Coverage (USA, 1980) | Approximately 90% of children received the polio vaccine by age 2 |
| Impact on Polio Cases (USA) | Polio cases were already rare by the 1980s due to successful vaccination campaigns since the 1950s |
| International Efforts | Increased focus on global vaccination through UNICEF, WHO, and Rotary International |
| Vaccine Type in 1980s | Oral Polio Vaccine (OPV) was widely used, with the Inactivated Polio Vaccine (IPV) also available |
| Policy Evolution | Mandatory policies were more common in earlier decades (1950s-1960s), with the 1980s seeing continued enforcement in many regions |
Explore related products






What You'll Learn
![]()
Polio eradication goals in the 1980s
The 1980s marked a pivotal decade in the global fight against polio, a disease that had long terrorized communities with its potential to cause paralysis and death. By this time, the polio vaccine, developed in the 1950s, had been widely distributed in many parts of the world, significantly reducing the disease’s prevalence. However, polio remained endemic in over 125 countries, particularly in regions with limited access to healthcare and vaccination infrastructure. The World Health Assembly, recognizing the urgency of the situation, set an ambitious goal in 1988: to eradicate polio worldwide by the year 2000. This target was not merely aspirational but backed by a strategic plan that emphasized mass immunization campaigns, surveillance, and international collaboration.
To achieve this goal, the Global Polio Eradication Initiative (GPEI) was launched as a public-private partnership led by national governments, the World Health Organization (WHO), Rotary International, the U.S. Centers for Disease Control and Prevention (CDC), and UNICEF. The initiative focused on delivering the oral polio vaccine (OPV) to children under five years old, as this age group was most vulnerable to the disease. OPV, administered in drops, was chosen for its ease of use and ability to induce intestinal immunity, which helped stop the spread of the virus in communities. Mass vaccination campaigns were organized in endemic countries, often reaching remote areas through door-to-door efforts and mobile clinics. By the end of the 1980s, these campaigns had begun to show results, with polio cases declining dramatically in regions where vaccination coverage was high.
Despite progress, challenges persisted. In many low-income countries, vaccine hesitancy, logistical hurdles, and political instability hindered efforts to reach every child. For instance, in some regions, rumors about the vaccine’s safety or religious concerns led to resistance among communities. To address these issues, the GPEI adopted a multi-pronged approach, including community engagement, education campaigns, and the involvement of local leaders to build trust. Additionally, surveillance systems were strengthened to detect and respond to outbreaks quickly. By 1989, the number of polio-endemic countries had dropped to 90, a testament to the effectiveness of these strategies, though the goal of complete eradication remained elusive.
A critical aspect of the 1980s eradication efforts was the emphasis on routine immunization alongside mass campaigns. While mass campaigns provided rapid coverage, routine immunization ensured sustained protection by integrating the polio vaccine into national health systems. This dual approach was essential for maintaining high immunity levels and preventing the re-emergence of the virus. For example, countries like India and Brazil implemented rigorous routine immunization programs, which, combined with mass campaigns, led to significant declines in polio cases. However, the success of these programs relied heavily on political commitment, adequate funding, and robust healthcare infrastructure—resources that were not uniformly available across all regions.
In retrospect, the polio eradication goals of the 1980s laid the foundation for one of the most ambitious public health endeavors in history. While the 2000 target was not met, the decade’s efforts demonstrated the feasibility of global eradication through coordinated action. The lessons learned—such as the importance of community engagement, surveillance, and sustained political will—continue to guide ongoing eradication efforts. Today, polio remains endemic in only two countries, a remarkable achievement that traces its roots to the bold vision set in the 1980s. The story of polio eradication is a reminder that even the most daunting global health challenges can be tackled with determination, innovation, and collaboration.
Secure Your Axis Bank Account: A Step-by-Step Guide to Creating Your MPIN
You may want to see also
Explore related products






![]()
Global vaccination policies during the decade
The 1980s marked a pivotal era in global vaccination policies, characterized by intensified efforts to eradicate polio and standardize immunization programs worldwide. The World Health Assembly’s 1988 resolution to eradicate polio by 2000 spurred countries to adopt more rigorous vaccination strategies. While the polio vaccine was not universally mandatory, many nations integrated it into their routine immunization schedules, often requiring proof of vaccination for school enrollment or international travel. This decade saw the widespread use of the oral polio vaccine (OPV), administered in multiple doses starting at 2 months of age, with a focus on reaching children in low-resource settings through mass vaccination campaigns.
Analyzing regional approaches reveals significant variations in policy implementation. In the United States, the polio vaccine was effectively mandatory for school entry, with exemptions granted only for medical or religious reasons. Similarly, European countries like Sweden and Germany incorporated polio vaccination into their national health programs, achieving high coverage rates through public health education and accessible healthcare systems. In contrast, developing nations faced challenges such as vaccine supply shortages, logistical hurdles, and public mistrust, which hindered universal coverage. The Global Polio Eradication Initiative (launched in 1988) played a crucial role in coordinating efforts, providing funding, and distributing vaccines to underserved regions.
A comparative perspective highlights the role of international collaboration in shaping vaccination policies. The Pan American Health Organization’s success in eliminating polio from the Americas by 1994 demonstrated the effectiveness of regional partnerships and standardized protocols. Meanwhile, countries in Africa and Southeast Asia struggled with lower vaccination rates due to weak healthcare infrastructure and political instability. These disparities underscored the need for tailored strategies, such as door-to-door vaccination drives and community engagement, to overcome local barriers. The decade also saw the introduction of the Expanded Program on Immunization (EPI), which aimed to integrate polio vaccination with other essential vaccines like measles and diphtheria, tetanus, and pertussis (DTP).
From a practical standpoint, the 1980s emphasized the importance of cold chain management and vaccine delivery systems. OPV, being heat-sensitive, required meticulous storage and transportation, particularly in tropical climates. Health workers were trained to administer the vaccine on a flexible schedule, ensuring children received all recommended doses (typically three to four) by age 5. Public awareness campaigns, often supported by UNICEF and WHO, educated parents about the vaccine’s safety and efficacy, addressing misconceptions that had fueled hesitancy in some communities. These efforts laid the groundwork for the significant decline in polio cases globally, from 350,000 in 1988 to just a few thousand by the decade’s end.
In conclusion, global vaccination policies in the 1980s were defined by a mix of mandatory measures, international cooperation, and innovative strategies to combat polio. While the vaccine was not universally compulsory, its integration into national health programs and mass campaigns achieved unprecedented coverage. The lessons from this decade—such as the need for adaptable policies, robust infrastructure, and community trust—continue to inform global health initiatives today. As we reflect on this era, it’s clear that the fight against polio was not just about administering doses but about building systems capable of reaching every child, everywhere.
Banks' Social Responsibility: Impact, Ethics, and Community Engagement Explored
You may want to see also
Explore related products






![]()
Mandatory vaccination laws by country
The 1980s marked a pivotal decade in the global fight against polio, with vaccination campaigns intensifying worldwide. While the polio vaccine itself wasn't universally mandated during this period, many countries implemented school-entry requirements that effectively made vaccination compulsory for children. This approach leveraged existing educational systems to ensure high immunization rates without formal nationwide mandates. For instance, the United States required proof of polio vaccination for school attendance, though enforcement varied by state. Similarly, European nations like Germany and France tied vaccination to school enrollment, creating a de facto mandate. These policies were instrumental in achieving the high coverage rates necessary for herd immunity, paving the way for polio eradication in many regions.
Contrastingly, some countries adopted direct legal mandates for polio vaccination during the 1980s, particularly in regions with persistent outbreaks. India, for example, launched aggressive vaccination drives under the Universal Immunization Programme (UIP) in 1985, making polio vaccination compulsory for all children under the age of five. This was coupled with mass immunization campaigns, such as National Immunization Days, where children received oral polio vaccine (OPV) doses of 0.1 mL, administered orally in two rounds annually. The success of these efforts was evident in the dramatic decline of polio cases, setting a precedent for future eradication initiatives.
A comparative analysis reveals that mandates alone were insufficient without robust infrastructure and public trust. Countries like Brazil and Mexico, which also mandated polio vaccination, supplemented laws with community engagement and accessible healthcare services. In Brazil, health workers went door-to-door to administer OPV, targeting children aged 0–5 years with a two-dose regimen spaced 4–6 weeks apart. This combination of legal requirements and grassroots efforts ensured that even remote populations were reached, contributing to the eventual eradication of polio in the Americas by 1994.
From a persuasive standpoint, the 1980s polio vaccination mandates underscore the balance between individual rights and public health. While some critics argue that mandates infringe on personal freedoms, the success of these policies in reducing polio cases highlights their effectiveness in protecting vulnerable populations. For instance, Australia’s "No Jab, No Play" policy, though implemented later, mirrors the 1980s approach by linking vaccination to childcare and school access. This model demonstrates that mandates, when paired with education and accessibility, can achieve high compliance without coercion.
In conclusion, the 1980s polio vaccination landscape was characterized by diverse strategies tailored to local contexts. Whether through school-entry requirements, direct legal mandates, or community-driven campaigns, countries prioritized immunization to combat polio. Practical takeaways include the importance of integrating mandates with infrastructure, ensuring vaccine accessibility, and fostering public trust. These lessons remain relevant today as nations navigate new vaccination challenges, proving that the 1980s polio efforts were not just a historical footnote but a blueprint for global health success.
Should You Sign a Refusal to Vaccinate Form? Key Considerations
You may want to see also
Explore related products






![]()
Public health campaigns and awareness
The 1980s marked a pivotal era in the global fight against polio, a disease that had once paralyzed or killed thousands annually. Public health campaigns during this decade were instrumental in driving awareness and vaccination uptake, though the mandate status of the polio vaccine varied by region. In the United States, for instance, while the vaccine was not federally mandated, individual states enforced school immunization requirements, effectively making it compulsory for school attendance. This hybrid approach—combining public health messaging with localized mandates—highlighted the power of awareness campaigns in achieving high vaccination rates.
One of the most effective strategies employed during this period was the use of clear, actionable messaging tailored to specific audiences. Campaigns often emphasized the simplicity and safety of the oral polio vaccine (OPV), which required just two drops administered orally, typically to children under five. Posters, television spots, and community health workers disseminated information about vaccination schedules, often recommending a series of doses at 2, 4, and 6 months of age, followed by boosters at 4 years and later. This specificity ensured parents understood not just the "why," but also the "how" of protecting their children.
Comparatively, global initiatives like the World Health Organization’s (WHO) Expanded Programme on Immunization (EPI) demonstrated how awareness campaigns could transcend borders. In countries where polio remained endemic, door-to-door campaigns and mass vaccination drives were paired with educational materials in local languages. For example, in India, health workers used visual aids and simple slogans to communicate the vaccine’s benefits, addressing cultural hesitancies and logistical barriers. This localized approach underscored the importance of adapting public health messaging to diverse contexts.
A critical takeaway from these campaigns is the role of trust-building in public health. By involving community leaders, healthcare providers, and survivors of polio in awareness efforts, campaigns humanized the issue and fostered credibility. For instance, testimonials from individuals who had experienced polio’s devastating effects served as powerful motivators for vaccination. This emotional appeal, combined with scientific evidence, created a compelling narrative that resonated with audiences worldwide.
Finally, the 1980s campaigns offer a blueprint for modern public health efforts, particularly in addressing vaccine hesitancy. By focusing on accessibility, clarity, and community engagement, these initiatives achieved remarkable success in reducing polio cases globally. For today’s health communicators, the lesson is clear: effective awareness campaigns must be informed by the needs and beliefs of their target audiences, leveraging both data and storytelling to drive action. Whether combating polio or other preventable diseases, this approach remains a cornerstone of public health strategy.
Is Sewickley Savings Bank a Notary Public? Find Out Here
You may want to see also
Explore related products






![]()
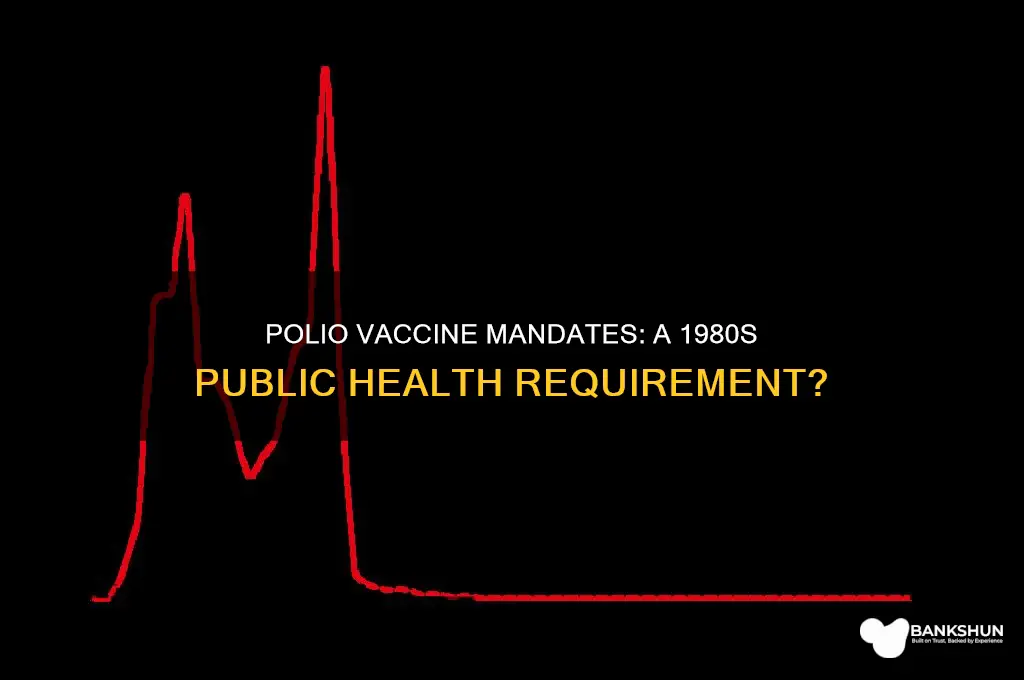
Impact of vaccination on polio cases
The global incidence of polio plummeted from an estimated 350,000 cases in 1988 to just 33 reported cases in 2018, a staggering 99.9% reduction. This dramatic decline is directly attributable to widespread vaccination efforts, particularly through the oral polio vaccine (OPV) and, later, the inactivated polio vaccine (IPV). The OPV, administered as drops, was favored in many countries due to its ease of delivery and ability to induce intestinal immunity, crucial for blocking transmission in endemic areas. Typically, the OPV regimen involves multiple doses starting at 6 weeks of age, with a minimum of three doses required for full protection.
Consider the contrasting trajectories of countries with high versus low vaccination rates. In India, where vaccination campaigns reached over 90% of the target population, polio was eradicated by 2014. Conversely, regions with vaccine hesitancy or logistical challenges, such as parts of Afghanistan and Pakistan, continue to report sporadic cases. For instance, in 2020, Afghanistan reported 56 cases, while Pakistan reported 84, highlighting the persistent risk in under-vaccinated populations. These examples underscore the critical role of achieving and maintaining high vaccination coverage to interrupt polio transmission.
From a practical standpoint, parents and caregivers must adhere to the recommended vaccination schedule to ensure immunity. The IPV, often used in combination with OPV in some countries, is administered via injection and provides robust protection against all three polio serotypes. It is particularly important in regions transitioning from OPV to IPV to prevent vaccine-derived poliovirus (VDPV) cases. For travelers to polio-endemic areas, the CDC recommends a single lifetime IPV booster dose for adults who completed the childhood series, ensuring continued protection against imported cases.
A comparative analysis reveals that the success of polio vaccination extends beyond individual immunity to herd immunity, which protects vulnerable populations, including newborns and immunocompromised individuals. For example, in the Americas, where polio vaccination became mandatory in many countries during the 1980s, the disease was eradicated by 1994. This achievement was facilitated by synchronized vaccination campaigns, such as National Immunization Days, which ensured high coverage across diverse populations. Such strategies demonstrate the power of collective action in disease eradication.
Finally, the impact of vaccination on polio cases serves as a testament to the effectiveness of public health interventions when rigorously implemented. However, complacency remains a risk. In 2020, the COVID-19 pandemic disrupted routine immunization services in many countries, leading to a resurgence of vaccine-preventable diseases. To sustain progress, governments and health organizations must prioritize vaccine accessibility, address misinformation, and strengthen surveillance systems. Practical steps include integrating polio vaccination into broader health services, leveraging digital tools for tracking, and engaging community leaders to build trust. The fight against polio is not over, but with continued vigilance and innovation, its eradication remains within reach.
Does U.S. Bank Stadium Feature a Retractable Roof? Facts Revealed
You may want to see also
Frequently asked questions
While the polio vaccine was not federally mandated in the 1980s, many states required proof of vaccination for school entry as part of their immunization laws.
No, policies varied by country. Some nations implemented mandatory polio vaccination programs, while others relied on strong recommendations and public health campaigns.
Yes, in places where the vaccine was required, exemptions were often available for medical, religious, or philosophical reasons, depending on local laws.
The 1980s saw continued enforcement of existing vaccination policies rather than major changes. Efforts focused on maintaining high immunization rates to prevent polio outbreaks.