Polio vaccination is a critical component of global health efforts to eradicate this debilitating disease, and the age at which children receive their first dose varies depending on the country and its immunization schedule. In many regions, including the United States, the Centers for Disease Control and Prevention (CDC) recommends that infants receive their initial polio vaccine at 2 months of age, followed by additional doses at 4 months and 6-18 months, as part of a comprehensive vaccination series to ensure long-term immunity. However, in some developing countries with higher polio prevalence, vaccination campaigns may target children as young as 6 weeks old, with multiple rounds of immunization drives conducted to reach as many children as possible and prevent outbreaks. Understanding the appropriate age for polio vaccination is essential for parents, healthcare providers, and policymakers to ensure timely protection against this highly contagious and potentially life-threatening disease.
| Characteristics | Values |
|---|---|
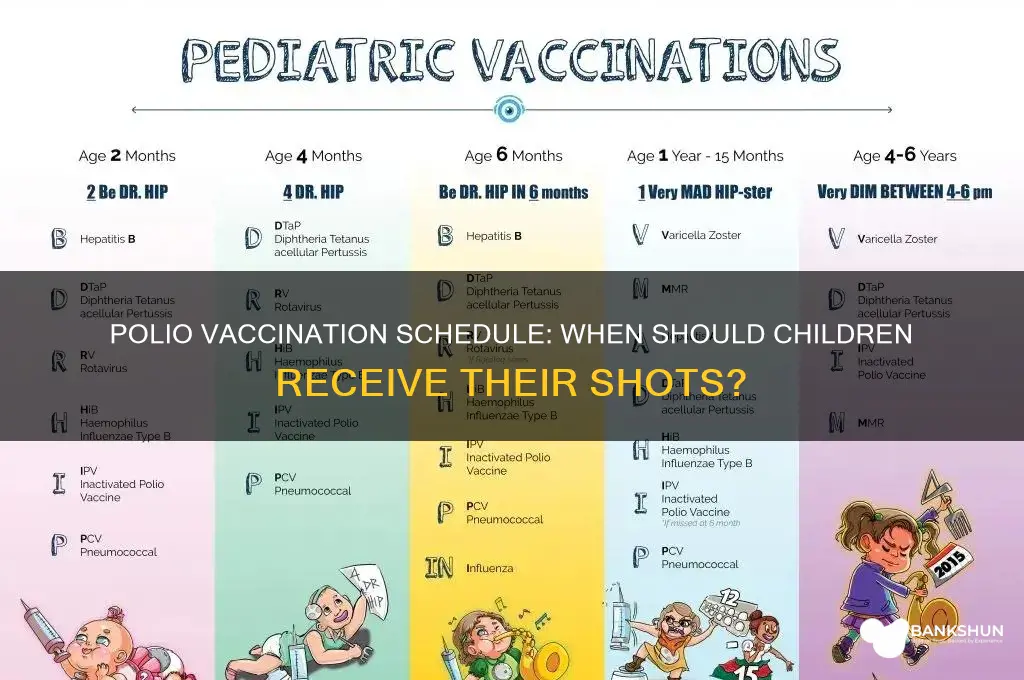
| Recommended Age for First Dose | 2 months (6 weeks to 2 months) |
| Subsequent Doses | 4 months, 6-18 months (depending on vaccine type and country schedule) |
| Booster Dose | 4-6 years (varies by country) |
| Vaccine Types | Inactivated Polio Vaccine (IPV), Oral Polio Vaccine (OPV) |
| Global Standardization | Varies; many countries use a 3-dose primary series + booster |
| WHO Recommendation | All children should receive at least 3 doses of polio vaccine |
| Age Range for Completion | Typically completed by 18 months, but can extend to 5 years |
| High-Risk Areas | Additional doses may be required in polio-endemic regions |
| Catch-Up Vaccination | Available for older children who missed earlier doses |
| Global Eradication Goal | Ongoing efforts to vaccinate children under 5 years globally |
Explore related products






What You'll Learn
![]()
Recommended Age for Polio Vaccine
The World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC) recommend a specific vaccination schedule for polio, a highly infectious disease that can lead to paralysis and even death. The age at which children receive their first polio vaccine varies slightly depending on the country and the type of vaccine used, but there is a general global consensus on the timing. In most countries, the polio vaccination series begins in infancy, with the first dose typically administered at 2 months of age. This initial dose is crucial, as it lays the foundation for the child's immunity against the poliovirus.
In the United States, the CDC recommends a four-dose schedule for the inactivated poliovirus vaccine (IPV). After the initial dose at 2 months, subsequent doses are given at 4 months, 6-18 months, and 4-6 years of age. This schedule ensures that children are protected during the periods when they are most vulnerable to the virus. It's essential to follow this timeline, as delaying doses can leave children susceptible to infection. For example, if a child misses the 4-month dose, it should be administered as soon as possible, and the subsequent doses should be given at the recommended intervals.
In contrast, some countries use the oral poliovirus vaccine (OPV), which has a slightly different schedule. The WHO recommends a primary series of three OPV doses, starting at 6 weeks of age, with a minimum interval of 4 weeks between doses. A fourth dose is often given as a booster, typically at 12-23 months of age. This schedule is particularly effective in providing rapid protection and has been instrumental in global polio eradication efforts. However, it's worth noting that OPV can, in rare cases, cause vaccine-associated paralytic polio (VAPP), which is why some countries prefer the IPV.
When traveling to areas where polio is still endemic or during outbreaks, additional precautions may be necessary. The CDC advises that adults who received their childhood vaccinations should get a one-time booster dose of IPV before traveling to such regions. For children, ensuring they are up-to-date with their vaccinations is crucial. If a child is behind on their polio vaccine schedule, a catch-up plan should be discussed with a healthcare provider. This might involve administering missed doses at specific intervals to ensure optimal protection.
In summary, the recommended age for initiating polio vaccination is during infancy, with the first dose typically given at 2 months of age. The subsequent doses are then administered at specific intervals, depending on the type of vaccine used. Adhering to this schedule is vital for individual protection and contributes to the global effort to eradicate polio. Parents and caregivers should consult their healthcare providers to ensure their children receive the appropriate vaccinations at the right time, especially before traveling to high-risk areas. This proactive approach is key to preventing the spread of polio and protecting future generations from this devastating disease.
Launching Your Mobile Banking App: A Step-by-Step Guide to Success
You may want to see also
Explore related products






![]()
Polio Vaccine Schedule for Infants
The polio vaccine schedule for infants is a critical component of early childhood immunization, designed to provide robust protection against poliomyelitis, a highly contagious viral disease that can lead to paralysis or death. In most countries, the World Health Organization (WHO) and national health authorities recommend a series of doses starting as early as 6 weeks of age. This staggered approach ensures the development of strong immunity while minimizing the risk of infection during the most vulnerable stages of infancy.
Analytical Perspective: The standard polio vaccine schedule typically begins with the first dose administered at 2 months of age, followed by subsequent doses at 4 months and 6–18 months, depending on the region and vaccine type. Inactivated Poliovirus Vaccine (IPV) is commonly used in many developed countries, while Oral Polio Vaccine (OPV) remains prevalent in areas with higher polio transmission rates. The timing of these doses is strategically planned to coincide with the waning of maternal antibodies, which can interfere with vaccine efficacy if administered too early. Studies show that this schedule provides over 99% protection against all three poliovirus strains after completion.
Instructive Approach: Parents and caregivers should adhere strictly to the recommended schedule provided by their healthcare provider. For IPV, the dosage is typically 0.5 mL per injection, administered intramuscularly or subcutaneously. OPV, on the other hand, is given orally in a 2-drop dose. It’s essential to complete all doses, as partial vaccination leaves children susceptible to infection. Missed doses can often be caught up without restarting the series, but consulting a healthcare professional is crucial to ensure proper timing.
Comparative Insight: Unlike some vaccines that require annual boosters, the polio vaccine series confers long-term immunity after completion. However, in polio-endemic regions, additional booster doses may be recommended during outbreaks or for travelers. This contrasts with the measles vaccine, for instance, which often requires a booster dose later in childhood. The polio vaccine’s efficacy and safety profile make it a cornerstone of global eradication efforts, with over 18 million cases of paralysis prevented since 1988 through widespread vaccination.
Practical Tips: To ensure a smooth vaccination experience, schedule appointments during times when your infant is well-rested and fed. After vaccination, monitor for mild side effects such as soreness at the injection site or low-grade fever, which typically resolve within 24–48 hours. Keep a record of vaccination dates and share this information with all healthcare providers to avoid missed doses. Finally, stay informed about local vaccination campaigns or updates to the schedule, especially if traveling to areas with ongoing polio transmission.
By following the polio vaccine schedule for infants, parents play a vital role in protecting their children and contributing to the global effort to eradicate this devastating disease.
Is 1st Security Bank Compatible with Samsung Pay? Find Out Here
You may want to see also
Explore related products






![]()
Booster Shots for Polio in Children
Polio vaccination schedules typically begin in infancy, with the first dose administered as early as 6 weeks of age in some countries. However, the need for booster shots later in childhood is a critical yet often overlooked aspect of polio eradication efforts. These boosters are designed to reinforce the immune system’s memory, ensuring long-term protection against the poliovirus. In most regions, the initial series of polio vaccines is followed by a booster dose between the ages of 4 and 6 years. This timing aligns with the maturation of the immune system, maximizing the vaccine’s effectiveness.
The dosage and type of booster shot can vary depending on the vaccine used in the primary series. For instance, if the initial doses were administered using the oral polio vaccine (OPV), the booster may also be OPV, though some countries transition to the inactivated polio vaccine (IPV) for added safety. IPV boosters are particularly common in regions where wild poliovirus transmission has been eliminated, as they eliminate the rare risk of vaccine-derived polio associated with OPV. The standard dose for an IPV booster is 0.5 mL, injected intramuscularly, typically in the thigh for younger children or the deltoid muscle for older ones.
One practical challenge with booster shots is ensuring adherence. Parents and caregivers may assume that the initial polio vaccine series provides lifelong immunity, unaware of the need for a booster. Healthcare providers play a crucial role in educating families about the importance of this additional dose. Reminder systems, such as text messages or immunization cards, can help improve compliance. Additionally, integrating the polio booster with other routine vaccinations, such as the DTaP or MMR, can streamline the process and reduce missed opportunities.
Comparatively, the approach to polio boosters differs significantly from other childhood vaccines. While some vaccines, like the MMR, require only one or two doses for long-term immunity, polio’s boosters reflect the virus’s persistence in certain regions and the need to maintain herd immunity. This distinction underscores the unique challenges of polio eradication, particularly in areas with low vaccination coverage or vaccine hesitancy. By prioritizing booster shots, public health systems can close immunity gaps and move closer to global eradication.
In conclusion, booster shots for polio in children are a vital component of the vaccination strategy, ensuring sustained protection against this debilitating disease. Administered typically between ages 4 and 6, these boosters reinforce immunity at a critical developmental stage. Practical measures, such as education and integrated vaccination schedules, can enhance adherence, while the choice of vaccine type (OPV or IPV) should align with regional health priorities. As the world edges closer to polio eradication, maintaining vigilance with booster doses remains essential to safeguard future generations.
Is It Safe to Do Bank Transfers? Security Tips and Risks
You may want to see also
Explore related products






![]()
Global Polio Vaccination Age Guidelines
The World Health Organization (WHO) recommends a standardized polio vaccination schedule to ensure global eradication of this crippling disease. This schedule typically begins with the first dose administered at 6 weeks of age, followed by subsequent doses at 10 weeks and 14 weeks. This initial series of three doses is crucial for building a strong foundation of immunity in infants. The specific vaccines used vary by region, with oral polio vaccine (OPV) being more common in developing countries due to its ease of administration and lower cost, while inactivated polio vaccine (IPV) is preferred in developed nations for its higher safety profile.
Booster doses play a vital role in maintaining long-term immunity. A fourth dose is generally given at 12-18 months, followed by a final booster between 4-6 years of age. These boosters are essential to reinforce the immune response and provide lasting protection against all three poliovirus strains. In some high-risk areas, additional campaigns may be conducted to administer supplementary doses, ensuring that even hard-to-reach populations are covered.
Regional variations in vaccination schedules reflect local disease prevalence and healthcare infrastructure. For instance, countries with ongoing polio transmission may adopt more aggressive vaccination strategies, including mass immunization campaigns targeting children up to 5 years of age. In contrast, countries that have been polio-free for years might focus on maintaining routine immunization with fewer supplementary doses. These tailored approaches ensure that resources are allocated efficiently to areas of greatest need.
Practical considerations for parents and caregivers include adhering strictly to the recommended schedule, as delays can leave children vulnerable during critical developmental stages. If a dose is missed, it’s important to consult healthcare providers promptly to reschedule. Additionally, keeping a vaccination record is essential for tracking doses and ensuring compliance, especially when traveling or relocating to different regions with varying health protocols.
Despite the success of global polio vaccination efforts, challenges remain. Vaccine hesitancy, logistical hurdles in remote areas, and the need for cold chain maintenance for IPV can disrupt immunization coverage. Addressing these issues requires coordinated efforts from governments, NGOs, and communities to educate, mobilize, and sustain vaccination drives. By understanding and following global polio vaccination age guidelines, we can collectively move closer to a polio-free world.
Locate TCF Bank on Zelle: A Quick and Easy Guide
You may want to see also
Explore related products






![]()
Polio Vaccine Timing in Different Countries
The timing of polio vaccination varies significantly across countries, reflecting differences in public health priorities, disease prevalence, and healthcare infrastructure. For instance, in the United States, the Centers for Disease Control and Prevention (CDC) recommends a series of four doses: at 2 months, 4 months, 6–18 months, and 4–6 years. This schedule is designed to ensure robust immunity before children enter school, where the risk of exposure might increase. In contrast, India, which has historically faced higher polio prevalence, administers the first dose at birth, followed by three additional doses at 6, 10, and 14 weeks, with boosters at 16–24 months and 5 years. This accelerated schedule addresses the higher risk of transmission in densely populated areas.
In countries with ongoing polio outbreaks or low vaccination coverage, the World Health Organization (WHO) often recommends supplementary immunization activities (SIAs) alongside routine schedules. For example, in Afghanistan and Pakistan, where wild poliovirus remains endemic, children under 5 years receive repeated doses during mass vaccination campaigns, sometimes as frequently as every 4–8 weeks. These campaigns use the oral polio vaccine (OPV), which is easier to administer in resource-limited settings but requires multiple doses to achieve full immunity. In contrast, wealthier nations like Canada and Australia primarily use the inactivated polio vaccine (IPV), which is injected and typically given in combination with other vaccines (e.g., DTaP-IPV-Hib) at 2, 4, 6, and 18 months, followed by a booster at 4–6 years.
A comparative analysis reveals that countries with high polio risk often prioritize early and frequent dosing, while those with low risk focus on fewer, strategically timed doses. For instance, the United Kingdom administers IPV at 8, 12, and 16 weeks, with a preschool booster, reflecting its polio-free status since 2003. Meanwhile, Nigeria, which was declared polio-free in 2020 after years of outbreaks, follows a schedule similar to India’s, with an additional focus on reaching underserved populations through SIAs. This highlights how vaccine timing is tailored to local epidemiology and healthcare access.
Practical considerations also influence timing. In regions with limited cold chain infrastructure, OPV is preferred due to its stability at room temperature, enabling wider distribution. However, its use requires careful planning to avoid vaccine-derived poliovirus (VDPV) cases, which can occur in underimmunized populations. Countries transitioning from OPV to IPV, as part of the global polio eradication strategy, must adjust schedules to ensure uninterrupted immunity. For parents, understanding these variations is crucial when traveling internationally, as some countries may require proof of vaccination or additional doses for visiting children.
Ultimately, polio vaccine timing is a dynamic, context-specific strategy shaped by disease burden, vaccine type, and logistical constraints. While global guidelines provide a framework, local adaptations ensure maximum protection. For families, staying informed about their country’s schedule and adhering to it remains the most effective way to safeguard children against this once-devastating disease.
Print Your FNB Bank Confirmation Letter: A Step-by-Step Guide
You may want to see also
Frequently asked questions
Children are typically vaccinated against polio starting at 2 months of age, with additional doses given at 4 months and 6-18 months, depending on the country’s immunization schedule.
The polio vaccine requires multiple doses for full protection. The exact number of doses varies by country, but it usually includes a primary series of 3-4 doses in infancy, followed by booster shots later in childhood.
Yes, children who missed their earlier doses can still receive the polio vaccine. Healthcare providers will create a catch-up schedule to ensure they receive the necessary doses for protection.
There are two types of polio vaccines: the inactivated poliovirus vaccine (IPV) and the oral poliovirus vaccine (OPV). The age of vaccination can vary depending on the type and the country’s immunization policy, but both are typically started in infancy.































