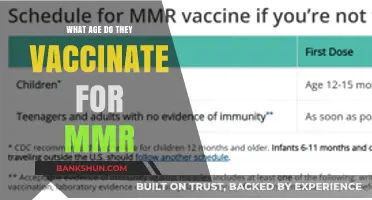
Meningococcal vaccines are crucial in preventing meningococcal disease, a potentially life-threatening bacterial infection that can lead to meningitis and sepsis. The recommended age for vaccination varies depending on the country and specific vaccine type, but generally, adolescents and young adults are prioritized due to their higher risk of infection. In many regions, the first dose is administered between 11 and 12 years of age, with a booster shot given at 16 years to ensure continued protection. Additionally, infants in some countries may receive the vaccine as early as 2 months old, particularly in areas with higher disease prevalence. It’s essential to consult local health guidelines or a healthcare provider to determine the appropriate vaccination schedule for meningococcal protection.
Explore related products






What You'll Learn
- Recommended Age Groups: Infants, adolescents, and young adults are primary targets for meningococcal vaccination
- Infant Vaccination Schedule: First dose at 2 months, followed by boosters as per healthcare guidelines
- Adolescent Vaccination: Typically administered at 11-12 years, with a booster at 16 years
- Catch-Up Vaccination: Unvaccinated older teens and young adults up to 23 years should get vaccinated
- High-Risk Groups: Individuals with certain medical conditions or living in close quarters may need earlier vaccination
![]()
Recommended Age Groups: Infants, adolescents, and young adults are primary targets for meningococcal vaccination
Infants are among the most vulnerable to meningococcal disease due to their underdeveloped immune systems. The Centers for Disease Control and Prevention (CDC) recommends that infants receive their first dose of the meningococcal conjugate vaccine (MenACWY) at age 11 or 12 years, with a booster dose at age 16 years. However, in certain high-risk situations, such as during a community outbreak or for infants with specific medical conditions like complement deficiencies or asplenia, vaccination may begin as early as 2 months of age. For these high-risk infants, a series of doses is typically administered, starting at 2 months, followed by doses at 4 months, 6 months, and a booster at 12-15 months. Parents should consult their pediatrician to determine the appropriate schedule based on individual risk factors.
Adolescents represent a critical age group for meningococcal vaccination, as they are at increased risk due to behaviors and living conditions that facilitate the spread of the bacteria. The CDC advises that all preteens receive the first dose of MenACWY at age 11 or 12, followed by a booster dose at age 16 to ensure continued protection during the high-risk years of late adolescence and early adulthood. Additionally, the meningococcal serogroup B (MenB) vaccine is recommended for adolescents aged 16-18 years, preferably at age 16 to 18, though it may be given as early as age 10 in certain circumstances. This two-pronged approach addresses the most common serogroups responsible for meningococcal disease in this age group.
Young adults, particularly college freshmen living in dormitories and military recruits, face elevated risks of meningococcal disease due to close quarters and increased social interactions. The CDC recommends that young adults who did not receive the MenACWY vaccine as adolescents should get vaccinated before starting college or other higher education programs. For those who received their last dose before age 16, a booster dose is advised to maintain immunity. The MenB vaccine is also recommended for young adults aged 16-23 years who are at increased risk, such as those with complement deficiencies, asplenia, or during outbreaks. Vaccination should ideally be completed before entering high-density living environments to maximize protection.
Practical tips for ensuring timely vaccination include scheduling appointments during routine check-ups or back-to-school physicals, keeping a record of vaccination dates, and staying informed about local outbreaks or updated guidelines. Parents and young adults should be aware that meningococcal vaccines are widely available at pediatrician offices, community health clinics, and pharmacies. Side effects are generally mild, such as soreness at the injection site or low-grade fever, and should not deter individuals from completing the recommended vaccine series. By targeting these age groups with tailored vaccination strategies, public health efforts can significantly reduce the incidence of meningococcal disease and its devastating complications.
Should Vaccines Be Mandated by Law? A Critical Debate
You may want to see also
Explore related products






![]()
Infant Vaccination Schedule: First dose at 2 months, followed by boosters as per healthcare guidelines
The meningococcal vaccine is a critical component of an infant's immunization journey, with the first dose typically administered at 2 months of age. This initial vaccination marks the beginning of a carefully structured schedule designed to provide robust protection against meningococcal disease, a severe bacterial infection that can lead to meningitis and sepsis. The timing of this first dose is strategic, aligning with the infant’s developing immune system and the vulnerability of early childhood. Healthcare providers emphasize the importance of adhering to this schedule to ensure optimal immunity, as delays can leave infants susceptible to infection during their most fragile months.
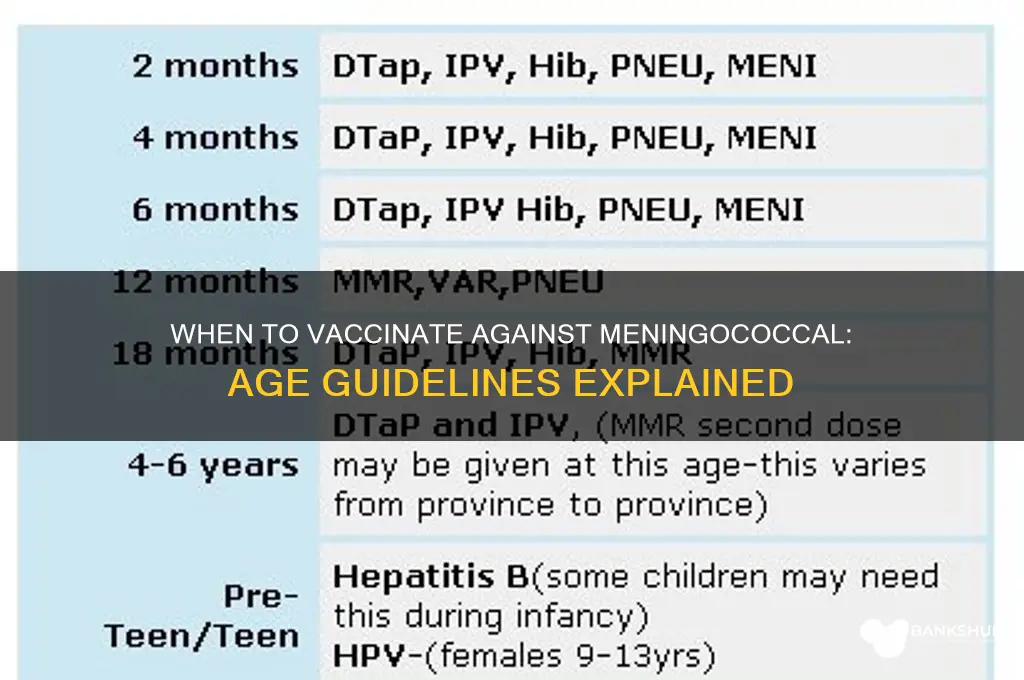
Following the first dose at 2 months, the meningococcal vaccine schedule includes boosters administered according to healthcare guidelines. For instance, the Centers for Disease Control and Prevention (CDC) recommends a second dose at 4 months and a third dose at 6 months for the meningococcal conjugate vaccine (MenACWY) in certain high-risk populations. However, for the general population, a booster dose is often given between 12 and 23 months of age. These boosters are essential to reinforce the immune response, ensuring long-term protection. Parents should consult their pediatrician to confirm the specific schedule, as individual health conditions or regional recommendations may influence timing.
One practical tip for parents is to integrate the meningococcal vaccine schedule with other routine immunizations to minimize clinic visits and reduce stress for both the child and caregiver. For example, the 2-month visit often includes vaccinations for hepatitis B, rotavirus, DTaP, Hib, and pneumococcal disease. By coordinating these appointments, parents can ensure their infant receives all necessary vaccines without overwhelming their schedule. Additionally, keeping a detailed record of vaccination dates and upcoming boosters can help avoid missed doses, which are critical for maintaining immunity.
It’s important to note that the meningococcal vaccine is available in different formulations, such as MenACWY and MenB, each targeting specific strains of the bacteria. The choice of vaccine and schedule may vary based on factors like age, risk of exposure, and regional disease prevalence. For example, MenB vaccines like Bexsero and Trumenba are typically given in a two- or three-dose series starting at 2 months, with intervals of at least one month between doses. Healthcare providers will guide parents on the most appropriate vaccine and schedule for their child, ensuring comprehensive protection.
In conclusion, the infant vaccination schedule for the meningococcal vaccine begins at 2 months, with boosters tailored to healthcare guidelines. This structured approach is designed to maximize immunity during the critical early months of life. By staying informed, coordinating with healthcare providers, and maintaining a vaccination record, parents can ensure their child receives timely doses and remains protected against this potentially life-threatening disease. Adherence to this schedule is a proactive step in safeguarding an infant’s health and well-being.
Crafting a Durable Fiberglass Bank Pole: A Step-by-Step Guide
You may want to see also
Explore related products

$20.46 $21.95





![]()
Adolescent Vaccination: Typically administered at 11-12 years, with a booster at 16 years
The meningococcal vaccine is a critical component of adolescent immunization schedules, designed to protect against meningococcal disease, a rare but potentially life-threatening bacterial infection. Adolescents are a primary target group for this vaccine due to their increased risk of contracting the disease, particularly as they enter their teenage years and early adulthood. The recommended vaccination timeline for this age group is a strategic approach to ensuring optimal protection during a vulnerable period.
The Initial Dose: A Preteen Milestone
At the age of 11 or 12, adolescents are advised to receive their first dose of the meningococcal conjugate vaccine, often referred to as MenACWY. This vaccine is a powerful tool, offering protection against four strains of the meningococcal bacteria (A, C, W, and Y). The timing of this vaccination is crucial, as it coincides with a period when the immune system is highly responsive, allowing for the development of robust immunity. A single dose at this age can provide substantial protection, but it's just the beginning of the vaccination journey.
Booster Shot: Reinforcing Immunity
Fast forward to the age of 16, and a booster dose becomes essential. This second dose serves as a critical reinforcement, ensuring that the immunity developed during early adolescence remains strong. The booster is typically another MenACWY vaccine, further solidifying defense against the targeted bacterial strains. This two-dose regimen is a strategic approach, maximizing the body's ability to recognize and combat potential meningococcal infections.
Practical Considerations and Tips:
- Scheduling: Parents and caregivers should aim to schedule the initial vaccination during a routine check-up at age 11 or 12, making it a convenient addition to other adolescent health assessments.
- Reminders: Setting a reminder for the booster dose is essential, as it ensures that the 16-year-old recipient doesn't miss this crucial second step.
- Side Effects: Mild side effects like soreness at the injection site, mild fever, or fatigue are common and typically subside within a few days. These are normal signs that the body is building immunity.
- Travel and Outbreaks: Adolescents planning international travel or living in areas with reported outbreaks may require additional considerations. Consulting a healthcare provider for region-specific advice is recommended.
This vaccination schedule is a well-structured strategy to combat meningococcal disease, a serious health threat. By following this timeline, adolescents can significantly reduce their risk, ensuring they are protected during a critical phase of their development. It's a simple yet powerful tool in the realm of preventive healthcare.
Jerusalem to West Bank: Distance, Travel Time, and Routes Explained
You may want to see also
Explore related products






![]()
Catch-Up Vaccination: Unvaccinated older teens and young adults up to 23 years should get vaccinated
Older teens and young adults who missed the meningococcal vaccine during adolescence face a critical gap in protection against a potentially deadly infection. Meningococcal disease, caused by the bacterium *Neisseria meningitidis*, can lead to meningitis or septicemia, with rapid onset and high fatality rates even in otherwise healthy individuals. While routine vaccination is recommended at ages 11–12, with a booster at 16, life’s unpredictability—whether due to oversight, lack of access, or personal circumstances—leaves many unvaccinated. For those aged 16 to 23, catch-up vaccination isn’t optional; it’s a necessary safeguard.
The catch-up schedule is straightforward but requires attention to detail. Unvaccinated individuals aged 16 to 23 should receive a single dose of the meningococcal conjugate vaccine (MenACWY), which protects against four serogroups (A, C, W, Y) responsible for most cases in this age group. If vaccinated after age 16, a booster dose isn’t required. However, those living in high-risk settings, such as college dormitories or military barracks, should prioritize vaccination due to the disease’s propensity to spread in close quarters. Practical tip: check with your healthcare provider or local health department for vaccine availability, as some clinics offer walk-in services or catch-up clinics tailored to this age group.
Comparing the risks of vaccination to the risks of meningococcal disease underscores the urgency of catch-up efforts. The vaccine is safe, with common side effects limited to mild soreness at the injection site or low-grade fever. In contrast, meningococcal disease progresses swiftly, often within hours, and even with treatment, 10–15% of infected individuals die, while survivors may face long-term complications like limb amputation or neurological damage. For young adults transitioning to independent living—whether starting college, traveling, or entering the workforce—vaccination is a small but life-saving step toward protecting their health and future.
Persuasively, the argument for catch-up vaccination rests on both individual and communal benefits. Young adults are not only safeguarding themselves but also reducing the disease’s spread in their social circles. This is particularly vital during late adolescence and early adulthood, when increased social interaction and shared living spaces elevate exposure risks. Parents, educators, and healthcare providers play a role in reminding this age group about the importance of vaccination, as many may assume they’ve “aged out” of eligibility. In reality, the window for catch-up vaccination closes at 23, making timely action essential.
In conclusion, catch-up meningococcal vaccination for unvaccinated older teens and young adults up to 23 years is a critical yet often overlooked health measure. With a single dose of MenACWY, individuals can bridge the immunity gap and shield themselves from a severe, fast-acting disease. Practical steps include verifying vaccination status, locating accessible clinics, and prioritizing vaccination before high-risk activities like college enrollment or international travel. By acting now, this age group can ensure their health remains a priority during a pivotal life stage.
Does US Bank Offer Hardship Programs? Exploring Financial Relief Options
You may want to see also
Explore related products






![]()
High-Risk Groups: Individuals with certain medical conditions or living in close quarters may need earlier vaccination
Certain medical conditions can compromise the immune system, leaving individuals more susceptible to meningococcal disease. For example, those with complement deficiencies (e.g., C5-C9, properdin, or factor H deficiencies) or asplenia (absence of a functioning spleen) face a significantly higher risk. The CDC recommends that individuals with these conditions receive the meningococcal conjugate vaccine (MenACWY) as early as 2 months of age, followed by booster doses every 3–5 years. For those with HIV infection, vaccination should begin at 2 months, with a 2-dose primary series of MenACWY and a booster dose every 5 years.
Living in close quarters, such as college dormitories, military barracks, or during outbreaks, amplifies the risk of meningococcal disease due to increased bacterial transmission. In these settings, vaccination is often prioritized earlier than the general population. For instance, college students living in dorms, particularly freshmen, are advised to receive a dose of MenACWY before starting school, even if they received a previous dose earlier than age 16. Similarly, military recruits are typically vaccinated upon entry into basic training, regardless of prior vaccination history, to mitigate the risk in crowded environments.
Practical tips for high-risk groups include maintaining a vaccination record to track doses and due dates for boosters. For individuals with medical conditions, consulting a healthcare provider is essential to determine the appropriate vaccine schedule and dosage. In communal living situations, institutions should implement vaccination campaigns and educate residents about the importance of timely immunization. Additionally, during outbreaks, public health officials may recommend serogroup B meningococcal (MenB) vaccination for those at risk, even if they’ve already received MenACWY.
Comparing the two high-risk categories, medical conditions often require lifelong adherence to a vaccination schedule, while those in close quarters may need temporary or situation-specific protection. For example, a person with asplenia will need regular MenACWY boosters indefinitely, whereas a college student may only need a single dose of MenB during their time in dorms. This distinction highlights the importance of tailoring vaccination strategies to individual risk factors and environments.
In conclusion, early and targeted vaccination is critical for high-risk groups to prevent meningococcal disease. Whether due to medical vulnerabilities or living conditions, these individuals benefit from accelerated or modified vaccine schedules. By understanding these specific needs, healthcare providers and at-risk populations can work together to ensure timely protection against this potentially life-threatening infection.
Tornado Targets Bank: Unheard-of Twister Tales
You may want to see also
Frequently asked questions
The meningococcal vaccine is typically recommended for preteens and teens, with the first dose given at age 11 or 12, followed by a booster dose at age 16.
Yes, younger children at increased risk, such as those with certain medical conditions or traveling to high-risk areas, may receive the meningococcal vaccine as early as age 2, depending on the specific vaccine type.
Many colleges and universities require the meningococcal vaccine for students living in dorms, typically before starting their freshman year, as teens and young adults are at higher risk for meningococcal disease.
Yes, there are two main types: MenACWY (recommended for preteens, teens, and young adults) and MenB (recommended for those at increased risk or as advised by a healthcare provider, regardless of age).
Yes, adults who are at increased risk, such as those with certain medical conditions, travelers to high-risk areas, or military recruits, can receive the meningococcal vaccine after consulting with their healthcare provider.