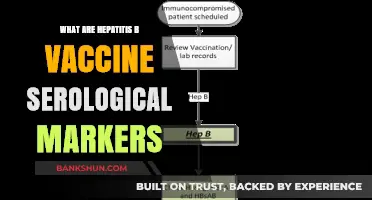
When discussing comorbidities in the context of vaccines, it refers to the presence of one or more additional health conditions alongside the primary disease or condition being targeted by the vaccine. These comorbidities can significantly impact the effectiveness, safety, and overall outcomes of vaccination. For instance, individuals with chronic illnesses such as diabetes, heart disease, or compromised immune systems are often considered to have comorbidities that may influence their response to vaccines. Understanding these comorbidities is crucial for healthcare providers to tailor vaccination strategies, ensuring optimal protection while minimizing potential risks for vulnerable populations.
Explore related products






What You'll Learn
- Chronic Respiratory Diseases: Asthma, COPD, cystic fibrosis increase vaccine comorbidity risks
- Cardiovascular Conditions: Heart disease, hypertension, stroke elevate vaccine comorbidity concerns
- Immune Disorders: HIV, autoimmune diseases, organ transplants affect vaccine comorbidity status
- Metabolic Disorders: Diabetes, obesity, kidney disease are key vaccine comorbidities
- Cancer and Treatments: Active cancer, chemotherapy, radiation therapy impact vaccine comorbidity considerations
![]()
Chronic Respiratory Diseases: Asthma, COPD, cystic fibrosis increase vaccine comorbidity risks
Chronic respiratory diseases such as asthma, chronic obstructive pulmonary disease (COPD), and cystic fibrosis (CF) significantly elevate the risks associated with vaccine comorbidities. These conditions compromise lung function and immune responses, making individuals more susceptible to severe outcomes from vaccine-preventable diseases. For instance, asthma patients, particularly those with moderate to severe forms, often experience exacerbated symptoms during respiratory infections, which vaccines aim to prevent. Similarly, COPD patients face heightened risks due to their already impaired lung capacity, while CF patients contend with recurrent infections and a weakened immune system. Understanding these risks is crucial for tailoring vaccination strategies to protect this vulnerable population effectively.
Vaccine administration in individuals with chronic respiratory diseases requires careful consideration of dosage and timing. For example, influenza and COVID-19 vaccines are strongly recommended for this group, but healthcare providers must monitor for potential side effects, such as respiratory distress. In asthma patients, vaccines should be administered during periods of stable disease control to minimize the risk of flare-ups. COPD patients may benefit from staggered dosing or adjuvanted vaccines to enhance immune response without overwhelming their compromised systems. CF patients, due to their frequent antibiotic use and unique immune challenges, often require personalized vaccination plans, including discussions about live attenuated vaccines, which are generally avoided in this population.
The interplay between chronic respiratory diseases and vaccine efficacy highlights the need for a proactive approach. Studies show that while vaccines are generally safe for these individuals, their effectiveness may be reduced due to underlying immune dysfunction. For instance, asthma patients with high IgE levels may mount a less robust response to certain vaccines. COPD patients often exhibit blunted immune reactions, necessitating booster doses or alternative formulations. CF patients, despite their challenges, can achieve adequate protection with timely and appropriately spaced vaccinations. Regular follow-ups and immune response assessments can help optimize outcomes for these groups.
Practical tips for managing vaccine comorbidities in chronic respiratory disease patients include maintaining open communication with healthcare providers, ensuring up-to-date vaccinations, and adhering to disease management plans. Patients should carry a detailed record of their respiratory conditions and medications to inform vaccination decisions. For caregivers and healthcare professionals, staying informed about the latest vaccine guidelines and contraindications is essential. Additionally, creating a supportive environment that addresses patient concerns and misconceptions about vaccines can improve compliance and overall health outcomes. By integrating these strategies, individuals with chronic respiratory diseases can navigate vaccination safely and effectively, reducing their risk of severe complications from preventable illnesses.
Is PNC Bank's Website Down? Troubleshooting Tips and Updates
You may want to see also
Explore related products






![]()
Cardiovascular Conditions: Heart disease, hypertension, stroke elevate vaccine comorbidity concerns
Cardiovascular conditions such as heart disease, hypertension, and stroke significantly amplify the risks associated with vaccine-related complications. These conditions compromise the body’s ability to respond effectively to immunization, often due to underlying inflammation, reduced immune function, or medication interactions. For instance, individuals with hypertension may experience heightened stress on their vascular system during vaccine-induced immune responses, potentially exacerbating blood pressure fluctuations. Similarly, those with a history of stroke face elevated risks of thromboembolic events post-vaccination, particularly with certain vaccine types. Understanding these interactions is critical for healthcare providers to tailor vaccination strategies, ensuring both safety and efficacy for this vulnerable population.
Analyzing the mechanisms behind these concerns reveals a complex interplay between cardiovascular health and immune activation. Vaccines stimulate the immune system to produce antibodies, a process that can temporarily increase inflammation and strain on the heart and blood vessels. For patients with heart disease, this added stress may trigger arrhythmias or worsen heart failure symptoms. Hypertensive individuals, especially those poorly controlled, are at risk of sudden spikes in blood pressure, which could lead to adverse events like myocardial infarction. Stroke survivors, particularly those on antiplatelet medications, must be monitored for bleeding risks or clotting abnormalities post-vaccination. These physiological responses underscore the need for personalized vaccine protocols, including pre-vaccination assessments and post-vaccination monitoring.
Practical steps can mitigate risks for individuals with cardiovascular comorbidities. First, consult a cardiologist or primary care physician to evaluate baseline cardiovascular stability before vaccination. Patients with uncontrolled hypertension should aim for a systolic blood pressure below 140 mmHg and diastolic below 90 mmHg prior to receiving a vaccine. Those on anticoagulants or antiplatelet medications may require temporary dosage adjustments, though this should only be done under medical supervision. Post-vaccination, individuals should monitor for symptoms like chest pain, shortness of breath, or sudden weakness, seeking immediate care if these occur. Hydration and rest are essential in the 48 hours following vaccination to minimize cardiovascular stress.
Comparatively, not all cardiovascular conditions carry the same level of risk. For example, well-managed hypertension with consistent medication adherence poses less concern than uncontrolled hypertension. Similarly, individuals with stable, mild heart disease may tolerate vaccines better than those with advanced heart failure. Stroke survivors with no residual deficits generally face lower risks than those with ongoing neurological impairments. This variability highlights the importance of individualized risk assessment, rather than a one-size-fits-all approach. Vaccination remains a critical preventive measure, but its administration must be carefully calibrated to the patient’s cardiovascular profile.
In conclusion, cardiovascular conditions demand heightened vigilance in vaccine administration due to their potential to exacerbate comorbidity risks. By understanding the specific challenges posed by heart disease, hypertension, and stroke, healthcare providers can implement targeted strategies to safeguard patients. This includes pre-vaccination evaluations, medication management, and post-vaccination monitoring. Patients, too, play a role by adhering to preparatory guidelines and recognizing warning signs. With careful planning, the benefits of vaccination can be maximized while minimizing risks, ensuring optimal outcomes for those with cardiovascular vulnerabilities.
Discover Grand Junction, Colorado's Top Local and National Banks
You may want to see also
Explore related products





![]()
Immune Disorders: HIV, autoimmune diseases, organ transplants affect vaccine comorbidity status
Individuals with immune disorders face unique challenges when it comes to vaccination, as their compromised immune systems can alter both the safety and efficacy of vaccines. HIV, autoimmune diseases, and organ transplants are prime examples of conditions that significantly affect vaccine comorbidity status. Understanding these interactions is crucial for healthcare providers and patients alike to ensure optimal protection without undue risk.
Consider HIV, a condition that weakens the immune system by attacking CD4 T-cells. While inactivated vaccines like the flu shot or hepatitis B vaccine are generally safe for people with HIV, live-attenuated vaccines—such as MMR (measles, mumps, rubella) or varicella (chickenpox)—may pose risks. For instance, the CDC recommends avoiding live vaccines if CD4 counts fall below 200 cells/mm³. Even when live vaccines are administered, their efficacy may be reduced in HIV-positive individuals due to impaired immune responses. Regular monitoring of immune status and consultation with an infectious disease specialist are essential to tailor vaccination strategies effectively.
Autoimmune diseases, such as rheumatoid arthritis, lupus, or multiple sclerosis, present another layer of complexity. These conditions involve the immune system mistakenly attacking healthy tissues, and immunosuppressive medications often used to manage them can blunt vaccine responses. For example, corticosteroids or biologics like TNF inhibitors may reduce the effectiveness of vaccines, particularly those requiring robust T-cell or B-cell activation. However, this doesn’t mean vaccination should be avoided. Instead, timing is critical: vaccines should ideally be administered during periods of disease remission and before starting immunosuppressive therapy. For instance, the shingles vaccine (Shingrix) is recommended for adults over 50 with autoimmune conditions, but it should be delayed if high-dose steroids are in use.
Organ transplant recipients face perhaps the most delicate balance, as their immune systems are intentionally suppressed to prevent organ rejection. This makes them highly susceptible to vaccine-preventable diseases while also reducing vaccine efficacy. For example, the COVID-19 mRNA vaccines have shown lower seroconversion rates in transplant recipients—often below 50% after two doses. A third dose is now recommended to improve protection, though responses remain suboptimal. Live vaccines are generally contraindicated in this population, but inactivated or subunit vaccines, such as those for influenza or pneumococcus, are strongly encouraged. Close collaboration with a transplant team is vital to determine the safest and most effective vaccination schedule.
Practical tips for managing vaccine comorbidities in immune disorders include maintaining open communication with healthcare providers, ensuring up-to-date immunization records, and considering antibody testing to assess vaccine-induced immunity when feasible. For caregivers and family members, staying current on their own vaccinations (e.g., flu, Tdap) can create a protective cocoon around immunocompromised individuals. While immune disorders complicate vaccination, they do not eliminate its necessity—with careful planning, vaccines remain a cornerstone of preventive care for these vulnerable populations.
MBA Graduates: Top Banking Careers to Launch Your Success
You may want to see also
Explore related products






![]()
Metabolic Disorders: Diabetes, obesity, kidney disease are key vaccine comorbidities
Metabolic disorders, particularly diabetes, obesity, and kidney disease, significantly impact vaccine efficacy and safety, making them critical comorbidities to consider in immunization strategies. These conditions alter immune responses, increase infection risks, and complicate vaccine administration, requiring tailored approaches for optimal protection.
Diabetes: A Double-Edged Risk
Individuals with diabetes, both type 1 and type 2, face heightened susceptibility to infections due to impaired immune function and chronic inflammation. Vaccines like the flu shot or COVID-19 vaccines are generally safe but may elicit weaker immune responses in this population. For instance, a 2021 study in *The Lancet Diabetes & Endocrinology* found that people with diabetes had lower antibody titers post-COVID-19 vaccination compared to non-diabetic controls. Practical tips include maintaining stable blood glucose levels before vaccination, as hyperglycemia can further dampen immune responses. Healthcare providers may also recommend adjuvanted vaccines or booster doses to enhance protection, particularly for older adults or those with poorly controlled diabetes.
Obesity: Beyond Physical Complications
Obesity, defined by a BMI ≥30, disrupts immune function through chronic low-grade inflammation and altered cytokine production. This metabolic state reduces vaccine efficacy, as seen with influenza and hepatitis B vaccines. A 2017 study in *Vaccine* reported that obese individuals had a 90% lower seroprotection rate after hepatitis B vaccination compared to normal-weight counterparts. For COVID-19 vaccines, obesity is linked to reduced neutralizing antibody levels and increased breakthrough infections. Practical strategies include prioritizing weight management through diet and exercise, though this should not delay vaccination. Clinicians may consider higher vaccine doses or additional boosters, though current guidelines do not specify obesity-related adjustments.
Kidney Disease: A Silent Comorbidity
Chronic kidney disease (CKD) impairs immune function and increases infection risks, particularly in end-stage renal disease (ESRD) patients. Vaccines like pneumococcal, influenza, and COVID-19 shots are recommended but often underperform in this population. For example, dialysis patients may require higher doses or more frequent boosters of the hepatitis B vaccine to achieve immunity. COVID-19 vaccines, while safe, show reduced efficacy in CKD patients, especially those on immunosuppressive therapies. Practical advice includes scheduling vaccinations on non-dialysis days for ESRD patients and ensuring coordination with nephrologists for timing and dosage adjustments.
Comparative Analysis and Takeaway
While diabetes, obesity, and kidney disease share metabolic roots, their impacts on vaccination differ. Diabetes primarily weakens immune responses, obesity reduces vaccine efficacy through inflammation, and kidney disease complicates immunization due to immune dysfunction and medication interactions. A unified approach involves proactive management of these conditions, individualized vaccine scheduling, and potential dose adjustments. For instance, the CDC recommends annual flu shots and COVID-19 boosters for all three groups, emphasizing the need for tailored strategies to bridge the immunity gap.
Practical Steps for Healthcare Providers
- Screen for Metabolic Comorbidities: Identify diabetes, obesity, and kidney disease during pre-vaccination assessments.
- Optimize Timing: Schedule vaccinations during periods of metabolic stability (e.g., controlled blood sugar, post-dialysis).
- Consider Boosters: Recommend additional doses for patients with suboptimal responses, particularly for COVID-19 and influenza vaccines.
- Educate Patients: Emphasize the importance of managing underlying conditions to enhance vaccine efficacy.
By addressing metabolic disorders as key vaccine comorbidities, healthcare providers can improve immunization outcomes and reduce infection risks in vulnerable populations.
BB&T Bank in Sedona: Exploring Banking Options in the Red Rock City
You may want to see also
Explore related products





![]()
Cancer and Treatments: Active cancer, chemotherapy, radiation therapy impact vaccine comorbidity considerations
Cancer patients face unique challenges when it comes to vaccination, as their immune systems are often compromised, either by the disease itself or by the treatments they undergo. Active cancer, particularly blood cancers like leukemia or lymphoma, can impair the body’s ability to mount an effective immune response. This means that even standard vaccine doses may not provide adequate protection. For instance, a study published in *Clinical Infectious Diseases* found that only 45% of leukemia patients developed sufficient antibodies after receiving the influenza vaccine, compared to 90% in the general population. This underscores the need for tailored vaccination strategies in this group.
Chemotherapy, a cornerstone of cancer treatment, further complicates vaccine efficacy. By targeting rapidly dividing cells, chemotherapy can suppress the immune system for weeks or months, depending on the regimen. For example, patients undergoing high-dose cyclophosphamide or anthracycline-based therapies may experience prolonged neutropenia, a condition where the body has abnormally low levels of infection-fighting white blood cells. Vaccination during this period is generally discouraged, as the immune system may not respond adequately. Instead, healthcare providers often recommend administering vaccines at least two weeks before starting chemotherapy or waiting until three months after treatment completion. However, this timeline can vary based on the specific drugs and the patient’s overall health.
Radiation therapy, while localized in its delivery, can also impact vaccine comorbidity considerations. Patients receiving radiation to lymph node areas, such as the axilla or groin, may experience lymphopenia, a reduction in lymphocyte counts. This can impair the immune response to vaccines, particularly those requiring robust T-cell activation, like the shingles vaccine. For these patients, delaying vaccination until after radiation therapy is completed—typically 4 to 6 weeks post-treatment—is often advised. Additionally, adjuvanted vaccines, which contain additives to enhance immune response, may be considered for patients with compromised immunity, though their use must be weighed against potential side effects.
Practical tips for cancer patients and their caregivers include maintaining open communication with the oncology team about vaccination schedules. For example, if a patient is due for a COVID-19 booster but is scheduled for chemotherapy in the next month, the provider might recommend accelerating the vaccine dose. Similarly, patients should be encouraged to receive annual influenza vaccines and stay up-to-date on pneumococcal vaccinations, as respiratory infections can be particularly dangerous for immunocompromised individuals. Finally, documenting all vaccinations in a centralized record, such as a CDC immunization card or digital health app, ensures continuity of care across providers.
In conclusion, cancer and its treatments introduce complex considerations for vaccine comorbidity. Active cancer, chemotherapy, and radiation therapy can all diminish immune responses, necessitating individualized vaccination plans. By understanding these interactions and following evidence-based guidelines, healthcare providers can optimize vaccine efficacy and protect this vulnerable population from preventable diseases. Patients, too, play a critical role by staying informed and proactive about their immunization status.
Moody's Downgrades 10 Major Banks: Financial Stability Concerns Rise
You may want to see also
Frequently asked questions
Comorbidities refer to the presence of one or more additional medical conditions or diseases alongside a primary condition in an individual. In the context of vaccines, certain comorbidities may influence vaccine recommendations, efficacy, or potential risks.
Common comorbidities that often factor into vaccine prioritization include cardiovascular disease, diabetes, chronic respiratory diseases (e.g., COPD), obesity, chronic kidney disease, immunocompromised states (e.g., HIV, cancer treatment), and liver disease. These conditions increase the risk of severe illness from vaccine-preventable diseases.
Yes, some comorbidities can impact vaccine efficacy. For example, immunocompromised individuals may have a reduced immune response to vaccines, making them less effective. In such cases, additional doses or specific vaccine types may be recommended.
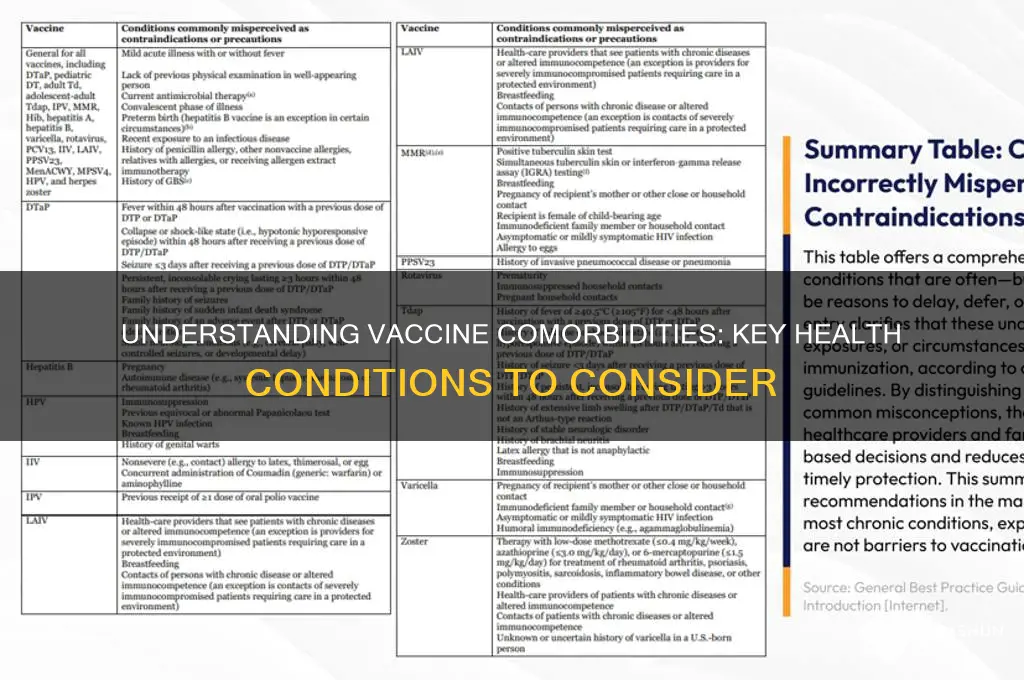
Certain live-attenuated vaccines, such as the MMR (measles, mumps, rubella) or varicella (chickenpox) vaccines, may be contraindicated or require caution in immunocompromised individuals due to the risk of vaccine-related complications. Inactivated or subunit vaccines are generally safer for this population.
Comorbidities can sometimes increase the likelihood or severity of vaccine side effects. For instance, individuals with a history of severe allergic reactions may be at higher risk for anaphylaxis from certain vaccine components. Healthcare providers assess these risks to determine the safest vaccination approach.