mRNA vaccines, pioneered by their groundbreaking use in COVID-19 immunization, have revolutionized the field of vaccinology by leveraging messenger RNA to instruct cells to produce specific proteins, triggering an immune response. Beyond COVID-19, this technology is being explored for a variety of other diseases, including influenza, HIV, Zika virus, and even cancer. For instance, mRNA vaccines are in development to target seasonal flu strains, offering the potential for faster production and broader protection compared to traditional flu vaccines. Additionally, research is underway to create mRNA-based vaccines for malaria, tuberculosis, and cytomegalovirus, as well as personalized cancer vaccines tailored to an individual’s tumor mutations. These advancements highlight the versatility and promise of mRNA technology in addressing a wide range of global health challenges.
Explore related products






What You'll Learn
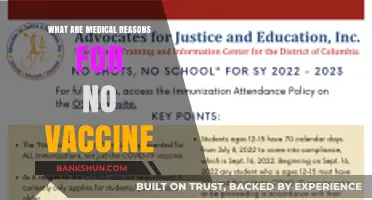
- COVID-19 mRNA Vaccines: Pfizer-BioNTech, Moderna, and their global impact on pandemic control
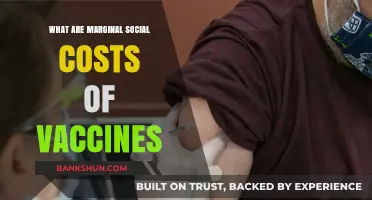
- Influenza mRNA Vaccines: Development for seasonal flu prevention and rapid response
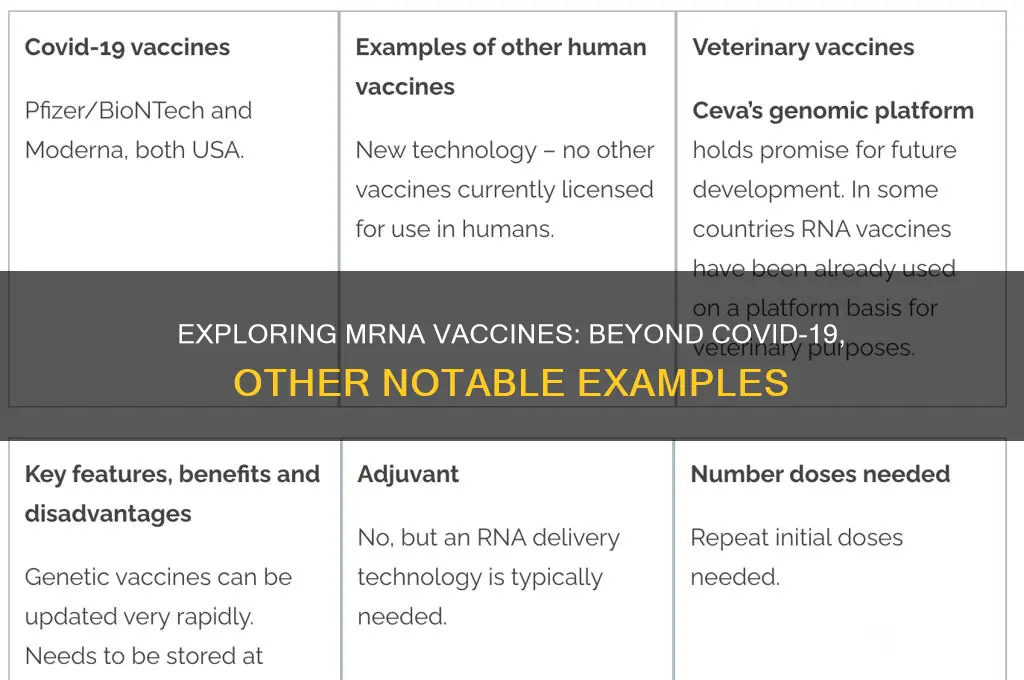
- Cancer mRNA Vaccines: Personalized therapies targeting tumors with specific mRNA sequences
- Zika Virus mRNA Vaccines: Experimental vaccines for preventing Zika virus infections
- Cytomegalovirus (CMV) mRNA Vaccines: Research for preventing CMV in vulnerable populations
![]()
COVID-19 mRNA Vaccines: Pfizer-BioNTech, Moderna, and their global impact on pandemic control
The COVID-19 pandemic accelerated the development and deployment of mRNA vaccines, with Pfizer-BioNTech and Moderna leading the charge. These vaccines, which teach cells to produce a harmless piece of the SARS-CoV-2 spike protein, triggered a global shift in vaccine technology. Unlike traditional vaccines that use weakened viruses or viral proteins, mRNA vaccines offer a rapid, adaptable platform, as evidenced by their record-breaking development timeline of less than a year. This innovation not only revolutionized pandemic response but also set a precedent for future vaccine development against other infectious diseases.
Pfizer-BioNTech’s BNT162b2 and Moderna’s mRNA-1273 were among the first mRNA vaccines authorized for emergency use, with efficacy rates of 95% and 94%, respectively, in clinical trials. Both vaccines require a two-dose primary series, typically administered 3–4 weeks apart, followed by booster doses to maintain immunity against emerging variants. Pfizer’s vaccine is approved for individuals aged 5 and older, while Moderna’s is authorized for those aged 6 months and older, with dosage adjustments for younger age groups. For example, children aged 6 months to 5 years receive a lower dose (3–10 micrograms) compared to adults (30 micrograms), ensuring safety and efficacy across populations.
The global impact of these vaccines cannot be overstated. By mid-2023, over 13 billion COVID-19 vaccine doses had been administered worldwide, with mRNA vaccines playing a pivotal role in reducing severe illness, hospitalizations, and deaths. Countries with high vaccination rates, such as Canada and Singapore, saw significant declines in COVID-19 mortality, highlighting the vaccines’ effectiveness in pandemic control. However, disparities in vaccine access, particularly in low-income countries, underscored the need for equitable distribution and local manufacturing capabilities. Initiatives like COVAX aimed to address these gaps, but challenges in logistics and hesitancy persisted.
A comparative analysis reveals that mRNA vaccines offer distinct advantages over other COVID-19 vaccine platforms, such as viral vector (e.g., AstraZeneca) or inactivated virus (e.g., Sinovac) vaccines. mRNA vaccines demonstrated higher efficacy against symptomatic disease and were more effective against variants like Delta and Omicron. Additionally, their side effect profiles—primarily mild to moderate reactions like fatigue, headache, and injection site pain—were well-tolerated by most recipients. This safety and efficacy profile bolstered public confidence, though misinformation and hesitancy remained barriers in some regions.
Moving forward, the success of COVID-19 mRNA vaccines has spurred research into their application for other diseases. Clinical trials are underway for mRNA-based vaccines targeting influenza, HIV, Zika, and even cancer. For instance, Moderna’s mRNA flu vaccine candidate has shown promising results in Phase 3 trials, potentially offering broader protection than traditional flu vaccines. Practical tips for individuals include staying informed about booster recommendations, especially for vulnerable populations, and verifying vaccine information from credible sources to combat misinformation. The legacy of Pfizer-BioNTech and Moderna’s mRNA vaccines lies not only in their role in ending the COVID-19 pandemic but also in their potential to transform global health for decades to come.
Securely Link Your Bank Account to Social Security Benefits: A Guide
You may want to see also
Explore related products


$26.59 $32.99




![]()
Influenza mRNA Vaccines: Development for seasonal flu prevention and rapid response
The seasonal flu remains a persistent global health challenge, causing millions of illnesses and hundreds of thousands of deaths annually. Traditional influenza vaccines, while effective, face limitations in their production speed and ability to match evolving viral strains. Influenza mRNA vaccines emerge as a promising solution, offering the potential for faster development, greater adaptability, and potentially broader protection.
Unlike traditional vaccines that use weakened or inactivated viruses, mRNA vaccines deliver genetic instructions to our cells, prompting them to produce a harmless piece of the flu virus, triggering an immune response. This approach allows for rapid manufacturing, as the mRNA sequence can be quickly updated to target new flu strains, a crucial advantage in the face of constantly mutating viruses.
Developing influenza mRNA vaccines involves several key steps. First, scientists identify the dominant flu strains circulating globally, a process guided by the World Health Organization. Next, they synthesize mRNA encoding for a specific viral protein, typically hemagglutinin, a key target for the immune system. This mRNA is then encapsulated in lipid nanoparticles, protecting it during delivery and facilitating its entry into cells. Clinical trials rigorously assess safety, dosage (typically in the microgram range), and efficacy across different age groups, from young children to the elderly, who are often more susceptible to severe flu complications.
One of the most significant advantages of mRNA technology is its potential for rapid response during flu pandemics. Traditional vaccine production can take months, leaving populations vulnerable during the early stages of an outbreak. mRNA vaccines, with their streamlined manufacturing process, could be developed and deployed within weeks, potentially saving countless lives.
While still under development, influenza mRNA vaccines hold immense promise for revolutionizing flu prevention. Their ability to adapt quickly to emerging strains, coupled with potentially broader immune responses, could lead to more effective and accessible seasonal flu vaccines. Furthermore, the platform's versatility opens doors for developing vaccines against other respiratory viruses, paving the way for a future with better protection against a wider range of infectious diseases.
Understanding the Structure of Central Banking in the United States
You may want to see also
Explore related products






![]()
Cancer mRNA Vaccines: Personalized therapies targeting tumors with specific mRNA sequences
Cancer mRNA vaccines represent a groundbreaking shift in oncology, leveraging the precision of mRNA technology to create personalized therapies tailored to individual tumor profiles. Unlike traditional vaccines that target pathogens, these vaccines encode specific mRNA sequences derived from a patient’s own tumor mutations, training the immune system to recognize and attack cancer cells uniquely. This approach hinges on neoantigens—proteins produced by tumor-specific mutations—which serve as distinct markers for immune targeting. By sequencing a patient’s tumor and identifying these neoantigens, researchers can design mRNA vaccines that stimulate a robust, targeted immune response, minimizing off-target effects.
The process begins with tumor biopsy and genomic sequencing to identify mutations unique to the patient’s cancer. Bioinformatics tools then predict which mutations are most likely to produce immunogenic neoantigens. These selected neoantigens are encoded into mRNA molecules, encapsulated in lipid nanoparticles for delivery, and administered via intramuscular injection. Clinical trials have explored dosing regimens, with typical protocols involving 3–4 doses spaced 3–4 weeks apart, though optimal dosing remains under investigation. Early-phase trials have demonstrated safety and immunogenicity, with some patients achieving durable responses, particularly when combined with checkpoint inhibitors.
One of the most compelling aspects of cancer mRNA vaccines is their adaptability. Tumors evolve over time, accumulating new mutations that can render initial treatments ineffective. However, the mRNA platform allows for rapid redesign and production of updated vaccines to target emerging neoantigens. This dynamic approach mirrors the evolving nature of cancer itself, offering a sustained therapeutic strategy. For instance, a patient with metastatic melanoma might receive an initial vaccine targeting 10–20 neoantigens, followed by a booster vaccine addressing new mutations identified during disease progression.
Despite promising results, challenges remain. Manufacturing personalized vaccines is resource-intensive and time-consuming, requiring coordination between biopsy, sequencing, and production. Additionally, not all tumors harbor sufficient mutations to generate effective neoantigens, limiting applicability. Cost is another barrier, as individualized therapies are inherently more expensive than off-the-shelf treatments. However, as technology advances and scales, these hurdles may diminish, making cancer mRNA vaccines a viable option for a broader patient population.
In practice, cancer mRNA vaccines are most advanced in melanoma, non-small cell lung cancer, and glioblastoma, where tumor mutational burden is often high. Patients considering this therapy should discuss eligibility with their oncologist, as factors like tumor type, mutational load, and overall health influence suitability. While still experimental, these vaccines embody the future of cancer treatment—a future where therapy is as unique as the disease itself. As research progresses, they may become a cornerstone of personalized medicine, transforming how we approach one of humanity’s most complex challenges.
Step-by-Step Guide to Making a Bank Giro Payment Easily
You may want to see also
Explore related products






![]()
Zika Virus mRNA Vaccines: Experimental vaccines for preventing Zika virus infections
The Zika virus, once a relatively obscure pathogen, gained global attention during the 2015-2016 outbreak in the Americas due to its link to severe birth defects and neurological disorders. While the urgency has subsided, the need for a vaccine remains, particularly for at-risk populations in endemic regions. mRNA technology, proven effective in COVID-19 vaccines, offers a promising avenue for Zika prevention. Several experimental mRNA vaccines are under development, leveraging the platform’s speed, adaptability, and safety profile.
One notable example is the mRNA-1893 vaccine, developed by Moderna in collaboration with the National Institute of Allergy and Infectious Diseases (NIAID). This vaccine encodes for the Zika virus pre-membrane and envelope proteins, triggering an immune response that produces neutralizing antibodies. Clinical trials have shown that a two-dose regimen, administered 28 days apart, induces robust immunity in healthy adults aged 18-49. Dosage typically ranges from 25 to 100 micrograms per injection, with minimal side effects such as mild pain at the injection site, fatigue, and headaches. While not yet approved for widespread use, mRNA-1893 represents a significant step forward in Zika prevention.
Another approach involves self-amplifying mRNA (saRNA) vaccines, which include genetic elements that enhance protein production within cells, potentially allowing for lower doses. The saRNA vaccine developed by the Walter Reed Army Institute of Research (WRAIR) has demonstrated efficacy in preclinical studies, protecting non-human primates from Zika infection. This technology could be particularly advantageous in resource-limited settings, as smaller doses may reduce production costs and improve accessibility. However, saRNA vaccines are still in earlier stages of development, with ongoing research to optimize stability and delivery methods.
Despite these advancements, challenges remain. Zika’s low prevalence in recent years has complicated large-scale clinical trials, making it difficult to assess vaccine efficacy in real-world settings. Additionally, the virus’s similarity to other flaviviruses, such as dengue, raises concerns about antibody-dependent enhancement (ADE), a phenomenon where pre-existing antibodies could worsen infection. Researchers are addressing these issues through careful trial design and the inclusion of diverse populations, including pregnant women and individuals in endemic areas.
For those interested in participating in Zika mRNA vaccine trials or staying informed, practical steps include monitoring clinical trial registries like ClinicalTrials.gov, consulting healthcare providers, and staying updated on public health advisories. While these vaccines are not yet available, their development underscores the versatility of mRNA technology in addressing emerging infectious diseases. As research progresses, Zika mRNA vaccines could become a critical tool in protecting vulnerable populations and preventing future outbreaks.
Jim Ovia's Journey: Founding Zenith Bank and Shaping Nigeria's Finance
You may want to see also
Explore related products






![]()
Cytomegalovirus (CMV) mRNA Vaccines: Research for preventing CMV in vulnerable populations
Cytomegalovirus (CMV) is a common virus that often causes mild or no symptoms in healthy individuals but poses significant risks to vulnerable populations, including newborns, pregnant women, and immunocompromised patients. Developing an mRNA vaccine for CMV is a critical area of research, as current preventive measures are limited. Unlike traditional vaccines, mRNA technology offers a rapid and adaptable approach to targeting viral proteins, such as CMV’s glycoprotein B (gB), which plays a key role in viral entry into host cells. Early studies have shown promising results, with mRNA vaccines eliciting robust neutralizing antibody responses in preclinical models, paving the way for human trials.
One of the challenges in CMV vaccine development is ensuring protection for pregnant women to prevent congenital CMV infection, a leading cause of birth defects. mRNA vaccines, with their ability to be quickly modified and scaled, could address this gap. For instance, a Phase 1 trial of a CMV mRNA vaccine (mRNA-1647) demonstrated safety and immunogenicity in healthy adults, with doses ranging from 20 to 100 µg. This trial highlighted the potential for mRNA vaccines to induce both humoral and cellular immune responses, crucial for preventing CMV transmission and disease. However, further research is needed to evaluate efficacy in pregnant women and neonates, where the immune response may differ.
Comparatively, CMV mRNA vaccines share similarities with other mRNA vaccines, such as those for COVID-19, in their mechanism of action but differ in target populations and disease burden. While COVID-19 vaccines were developed for widespread use, CMV vaccines are targeted at specific high-risk groups, requiring tailored dosing and delivery strategies. For example, immunocompromised patients, such as organ transplant recipients, may need higher doses or adjuvanted formulations to overcome their weakened immune systems. This precision underscores the versatility of mRNA technology in addressing diverse public health challenges.
Practical considerations for CMV mRNA vaccines include storage and distribution, particularly in low-resource settings where CMV prevalence is high. Unlike early mRNA vaccines requiring ultra-cold storage, newer formulations are being developed to remain stable at standard refrigerator temperatures, improving accessibility. Additionally, educating healthcare providers and at-risk populations about the importance of CMV prevention will be crucial for vaccine uptake. For pregnant women, screening for CMV immunity and offering vaccination to seronegative individuals could become a standard prenatal care practice, reducing the risk of congenital infection.
In conclusion, CMV mRNA vaccines represent a promising frontier in preventive medicine, leveraging the flexibility and efficacy of mRNA technology to protect vulnerable populations. While challenges remain, ongoing research and advancements in vaccine design and delivery are bringing us closer to a world where CMV-related complications are significantly reduced. As with other mRNA vaccines, the success of CMV vaccines will depend on rigorous clinical trials, equitable distribution, and public health strategies tailored to the unique needs of at-risk groups.
TCF Bank in California: Locations, Services, and Availability Explained
You may want to see also
Frequently asked questions
Other examples of mRNA vaccines in development or clinical trials include those for influenza (flu), Zika virus, rabies, and cytomegalovirus (CMV). Additionally, mRNA technology is being explored for vaccines against HIV, tuberculosis, and various types of cancer.
Yes, mRNA vaccines are being developed for veterinary use. For example, an mRNA vaccine for infectious bronchitis virus (IBV) in chickens has been studied, and research is ongoing for mRNA vaccines to protect livestock and pets against various diseases.
Experimental mRNA vaccines in research include those targeting respiratory syncytial virus (RSV), malaria, norovirus, and certain types of allergies. mRNA technology is also being investigated for personalized cancer vaccines and vaccines against autoimmune diseases.