Conjugate vaccines, while highly effective in preventing bacterial infections such as those caused by *Streptococcus pneumoniae* and *Neisseria meningitidis*, are not without their drawbacks. One significant disadvantage is their high production cost, which can limit accessibility, particularly in low-resource settings. Additionally, conjugate vaccines often provide protection against only a specific subset of serotypes, leaving individuals vulnerable to strains not covered by the vaccine. This limitation can lead to serotype replacement, where non-vaccine serotypes become more prevalent. Furthermore, the complexity of their manufacturing process increases the risk of variability in vaccine quality, potentially affecting efficacy. Lastly, while rare, adverse reactions such as injection site pain, fever, or allergic responses can occur, raising concerns about safety in certain populations. These factors highlight the need for ongoing research and improvements in conjugate vaccine technology.
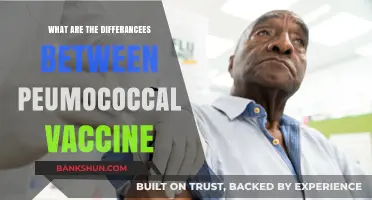
| Characteristics | Values |
|---|---|
| Cost | Generally more expensive to produce compared to traditional vaccines due to complex manufacturing processes involving conjugation of antigens to carrier proteins. |
| Storage Requirements | Often require strict cold chain storage to maintain stability, which can be challenging in resource-limited settings. |
| Number of Doses | May require multiple doses to achieve adequate immunity, which can be logistically demanding and impact compliance. |
| Limited Spectrum | Typically target specific serotypes of a pathogen, leaving individuals vulnerable to other serotypes not included in the vaccine. |
| Carrier Protein Reactions | In rare cases, the carrier protein used in conjugation can elicit an immune response, potentially leading to allergic reactions or other adverse events. |
| Hypo-responsiveness | Some individuals may exhibit hypo-responsiveness to conjugate vaccines, meaning they produce a weaker immune response compared to other vaccine types. |
Explore related products






What You'll Learn
- Limited serotype coverage in conjugate vaccines can leave some strains unprotected
- High production costs increase vaccine prices, reducing accessibility in low-income regions
- Potential for immune interference with natural immunity or other vaccines
- Short-term protection may require frequent booster doses for sustained immunity
- Risk of hypersensitivity reactions due to carrier proteins in conjugate formulations
![]()
Limited serotype coverage in conjugate vaccines can leave some strains unprotected
Conjugate vaccines, while revolutionary in preventing bacterial infections, face a critical limitation: their serotype coverage. Unlike broad-spectrum antibiotics, these vaccines target specific serotypes of pathogens, such as *Streptococcus pneumoniae* (pneumococcus). For instance, the 13-valent pneumococcal conjugate vaccine (PCV13) protects against 13 serotypes responsible for approximately 70-80% of invasive pneumococcal disease in children. However, this leaves a significant portion of strains—often referred to as non-vaccine serotypes—unprotected. These serotypes can continue to cause disease, particularly in regions with high pneumococcal diversity, undermining the vaccine’s overall effectiveness.
Consider the practical implications for immunization programs. PCV13 is typically administered in a 4-dose series to infants at 2, 4, 6, and 12-15 months of age. While this schedule maximizes protection against targeted serotypes, it does nothing to address the remaining 20-30% of strains. In low-resource settings, where non-vaccine serotypes may predominate, this limitation can lead to persistent disease burden despite high vaccination rates. For example, studies in Africa and Asia have shown an increase in non-PCV13 serotypes causing invasive pneumococcal disease post-vaccine introduction, highlighting the need for broader coverage.
Expanding serotype coverage is not a straightforward solution. Developing a conjugate vaccine that includes all 90+ known pneumococcal serotypes is impractical due to cost, complexity, and potential immune interference. Instead, researchers are exploring alternative strategies, such as protein-based vaccines targeting conserved pneumococcal proteins or whole-cell vaccines. However, these approaches are still in early stages, leaving current conjugate vaccines as the primary tool with inherent limitations.
For healthcare providers and policymakers, understanding this limitation is crucial for managing expectations and designing complementary interventions. In regions with high non-vaccine serotype prevalence, surveillance systems should monitor serotype shifts post-vaccination. Additionally, ensuring access to antibiotics for treating pneumococcal infections remains essential, particularly in vulnerable populations like young children and the elderly. While conjugate vaccines have transformed disease prevention, their limited serotype coverage serves as a reminder that no single intervention can fully eliminate the threat of bacterial pathogens.
Understanding Yes Bank's Share Count: A Comprehensive Overview
You may want to see also
Explore related products






![]()
High production costs increase vaccine prices, reducing accessibility in low-income regions
The high production costs of conjugate vaccines directly contribute to their elevated prices, creating a significant barrier to accessibility in low-income regions. Unlike traditional vaccines, conjugate vaccines require complex manufacturing processes, including the chemical linkage of a weak antigen (polysaccharide) to a carrier protein. This precision engineering demands advanced technology, specialized equipment, and stringent quality control, all of which drive up production expenses. For instance, the production of a single dose of the pneumococcal conjugate vaccine (PCV) can cost several times more than that of a whole-cell pertussis vaccine, making it less affordable for cash-strapped healthcare systems.
Consider the impact on immunization programs in sub-Saharan Africa, where the average per capita health expenditure is less than $50 annually. A single dose of PCV, priced at $15–$20 in the global market, represents a substantial financial burden for governments and families alike. While initiatives like Gavi, the Vaccine Alliance, subsidize costs for eligible countries, the subsidies often cover only a fraction of the total expense. This leaves many low-income regions with difficult choices: allocate limited resources to conjugate vaccines and risk neglecting other essential health services, or forgo these vaccines altogether, leaving populations vulnerable to preventable diseases.
To mitigate this challenge, stakeholders must explore innovative solutions. One approach is to streamline production processes through technological advancements, such as recombinant DNA technology, which could reduce reliance on costly chemical conjugation methods. Another strategy involves fostering partnerships between pharmaceutical companies and local manufacturers in low-income countries to build regional production capacity. For example, the Serum Institute of India has successfully produced affordable versions of conjugate vaccines, demonstrating the potential for cost-effective local manufacturing.
However, reducing production costs alone is insufficient without addressing distribution and administration challenges. Low-income regions often lack robust cold chain infrastructure, trained healthcare workers, and public awareness campaigns—all critical for vaccine delivery. Policymakers must adopt a holistic approach, investing in both production efficiency and healthcare system strengthening to ensure conjugate vaccines reach those who need them most. Without such integrated efforts, the promise of conjugate vaccines will remain out of reach for millions, perpetuating health disparities between high- and low-income regions.
Step-by-Step Guide to Becoming a Successful Bank Clerk
You may want to see also
Explore related products






![]()
Potential for immune interference with natural immunity or other vaccines
Conjugate vaccines, while revolutionary in preventing diseases like pneumococcal pneumonia and meningococcal meningitis, carry a nuanced risk: immune interference. This phenomenon occurs when the immune response triggered by one vaccine inadvertently affects the body’s ability to mount a robust response to another antigen, either from a different vaccine or natural exposure. For instance, studies have shown that the pneumococcal conjugate vaccine (PCV13) can reduce the immune response to certain serotypes not included in the vaccine, a process known as serotype replacement. This interference highlights the delicate balance between targeted immunity and the broader immune landscape.
Consider the practical implications for pediatric vaccination schedules. Infants receive multiple vaccines simultaneously, such as DTaP, Hib, and PCV13, often at 2, 4, and 6 months of age. While this approach maximizes compliance, it raises concerns about immune competition. Research suggests that high doses of certain conjugate vaccines can temporarily overshadow the immune response to co-administered vaccines, particularly in younger age groups. For example, a 2018 study found that PCV13 reduced the antibody titers to the *Haemophilus influenzae* type b (Hib) vaccine when given concurrently. To mitigate this, healthcare providers may consider staggering doses or adjusting the timing of vaccine administration, though this requires careful planning to avoid delays in protection.
The interplay between conjugate vaccines and natural immunity adds another layer of complexity. Natural infections often elicit a broader immune response compared to vaccination, involving both humoral and cell-mediated immunity. Conjugate vaccines, however, primarily stimulate antibody production. This disparity can lead to situations where vaccinated individuals may be less equipped to handle serotypes not covered by the vaccine, as their immune systems have not been exposed to the full spectrum of antigens. For example, while PCV13 protects against 13 pneumococcal serotypes, it does not cover all 90+ known serotypes, leaving room for non-vaccine serotypes to cause disease. This underscores the importance of surveillance programs to monitor shifting serotype prevalence.
From a persuasive standpoint, the potential for immune interference should not overshadow the undeniable benefits of conjugate vaccines. However, it does call for a more tailored approach to vaccine development and administration. For instance, incorporating additional serotypes into existing vaccines or developing next-generation conjugates with improved immunogenicity could reduce interference risks. Parents and caregivers should also be educated about the rationale behind vaccine schedules and the possibility of minor immune interactions, ensuring informed decision-making. Ultimately, while immune interference is a valid concern, it is a manageable one with proactive strategies and ongoing research.
Is J&J Vaccine Available in Florida? Latest Updates and Locations
You may want to see also
![]()
Short-term protection may require frequent booster doses for sustained immunity
Conjugate vaccines, while revolutionary in preventing diseases like pneumococcal pneumonia and meningococcal meningitis, often provide short-term protection compared to natural infection or live-attenuated vaccines. This limitation stems from their design: they combine a weak antigen (polysaccharide) with a strong carrier protein to enhance immune response. However, this engineered immunity wanes faster, typically within 5–10 years, depending on the vaccine and individual factors like age and immune status. For instance, the pneumococcal conjugate vaccine (PCV13) requires a booster dose as early as 5 years after the initial series in certain high-risk groups, such as immunocompromised individuals.
The need for frequent boosters introduces practical challenges. For children, adhering to a multi-dose schedule can be burdensome for parents, requiring repeated clinic visits and potential disruptions to daily routines. Adults, particularly the elderly, may face accessibility issues, as booster reminders are often less systematic compared to childhood immunization programs. For example, the meningococcal conjugate vaccine (MenACWY) is recommended every 5 years for at-risk adolescents and young adults, but compliance rates drop significantly after the initial dose. This inconsistency undermines herd immunity and leaves individuals vulnerable during gaps between doses.
From a public health perspective, the logistical and financial implications of frequent boosters are substantial. Vaccination campaigns must account for storage, distribution, and administration costs, which multiply with each additional dose. In low-resource settings, these demands can strain already fragile healthcare systems. For instance, the Haemophilus influenzae type b (Hib) conjugate vaccine, requiring a primary series plus booster, has been challenging to implement in regions with limited infrastructure. Even in high-income countries, the economic burden of repeated doses can deter policymakers from prioritizing conjugate vaccines over alternatives with longer-lasting immunity.
Despite these challenges, strategies exist to mitigate the need for frequent boosters. Adjuvants, such as aluminum salts or newer lipid-based formulations, can enhance the immune response to conjugate vaccines, potentially extending protection. Research into alternative dosing schedules, like fractional dosing or delayed boosters, is also underway. For example, studies have shown that a single booster dose of PCV13 administered 3–5 years after the primary series can significantly elevate antibody levels in adults. Practical tips for individuals include setting calendar reminders for booster appointments and inquiring about combination vaccines that reduce the number of clinic visits.
In conclusion, while conjugate vaccines are indispensable tools in disease prevention, their short-term protection necessitates careful planning and innovation. Balancing the benefits of immunity with the practicalities of frequent boosters requires collaboration among healthcare providers, policymakers, and individuals. By adopting evidence-based strategies and leveraging technological advancements, the drawbacks of this limitation can be minimized, ensuring sustained protection for vulnerable populations.
Deutsche Bank's Organizational Structure: Exploring Its Diverse Business Divisions
You may want to see also
![]()
Risk of hypersensitivity reactions due to carrier proteins in conjugate formulations
Conjugate vaccines, while revolutionary in preventing diseases like meningitis and pneumonia, carry a unique risk: hypersensitivity reactions triggered by carrier proteins. These proteins, essential for enhancing the immune response to the polysaccharide antigen, can inadvertently provoke an allergic response in susceptible individuals. Unlike traditional vaccines, conjugate formulations introduce foreign proteins that may not have been encountered before, increasing the likelihood of an immune system overreaction. This risk is particularly notable in vaccines such as Prevnar 13, where the carrier protein CRM197 (a non-toxic diphtheria toxin variant) has been associated with rare but severe allergic reactions.
The mechanism behind these reactions lies in the carrier protein’s ability to stimulate both the desired immune response and an unintended allergic response. When the immune system misidentifies the carrier protein as a threat, it produces IgE antibodies, which can lead to immediate hypersensitivity reactions upon re-exposure. Symptoms range from mild, such as localized swelling or hives, to severe, including anaphylaxis—a life-threatening condition requiring immediate medical intervention. Infants and young children, who receive conjugate vaccines as part of routine immunization schedules (e.g., at 2, 4, 6, and 12–15 months), are at higher risk due to their developing immune systems.
Clinicians must remain vigilant for signs of hypersensitivity, particularly during and after vaccine administration. Pre-vaccination screening for a history of allergies, especially to diphtheria toxoid or other vaccine components, is critical. For individuals with known allergies, alternative vaccines or desensitization protocols may be considered, though these options are limited. Post-vaccination observation for 15–30 minutes is standard practice to monitor for immediate reactions, and caregivers should be educated on recognizing delayed symptoms, such as persistent rash or difficulty breathing.
Despite these risks, the benefits of conjugate vaccines in preventing deadly diseases far outweigh the potential for hypersensitivity reactions. However, ongoing research aims to mitigate this issue by exploring alternative carrier proteins or adjuvants that reduce allergenicity while maintaining vaccine efficacy. For instance, studies are investigating the use of recombinant proteins or synthetic carriers that minimize the risk of immune cross-reactivity. Until such advancements become standard, healthcare providers must balance the imperative of disease prevention with the need for individualized risk assessment and management.
In practical terms, parents and caregivers can take proactive steps to minimize risks. Ensure all known allergies are communicated to healthcare providers before vaccination. Keep a record of previous vaccine reactions, if any, and report them promptly. In the event of a severe reaction, epinephrine auto-injectors should be readily available, especially for those with a history of allergies. While hypersensitivity reactions to carrier proteins are rare, awareness and preparedness are key to ensuring the safe administration of conjugate vaccines.
Kaiser's Role in Monkeypox Vaccination: Availability and Eligibility Explained
You may want to see also
Frequently asked questions
Conjugate vaccines, like all vaccines, can cause mild side effects such as pain or swelling at the injection site, fever, or irritability. Rarely, more serious reactions like severe allergic responses may occur, though these are extremely uncommon.
There is no scientific evidence to suggest that conjugate vaccines cause long-term health issues. Extensive testing and ongoing monitoring ensure their safety, and they are widely considered one of the safest and most effective types of vaccines.
While conjugate vaccines are highly effective, their efficacy can vary depending on factors like age, immune status, and the specific vaccine. For example, older adults or immunocompromised individuals may have a reduced response, requiring additional doses or alternative strategies.
Conjugate vaccines target specific bacterial strains and do not contribute to antibiotic resistance. In fact, they reduce the prevalence of vaccine-preventable bacterial infections, decreasing the need for antibiotics and indirectly combating resistance.