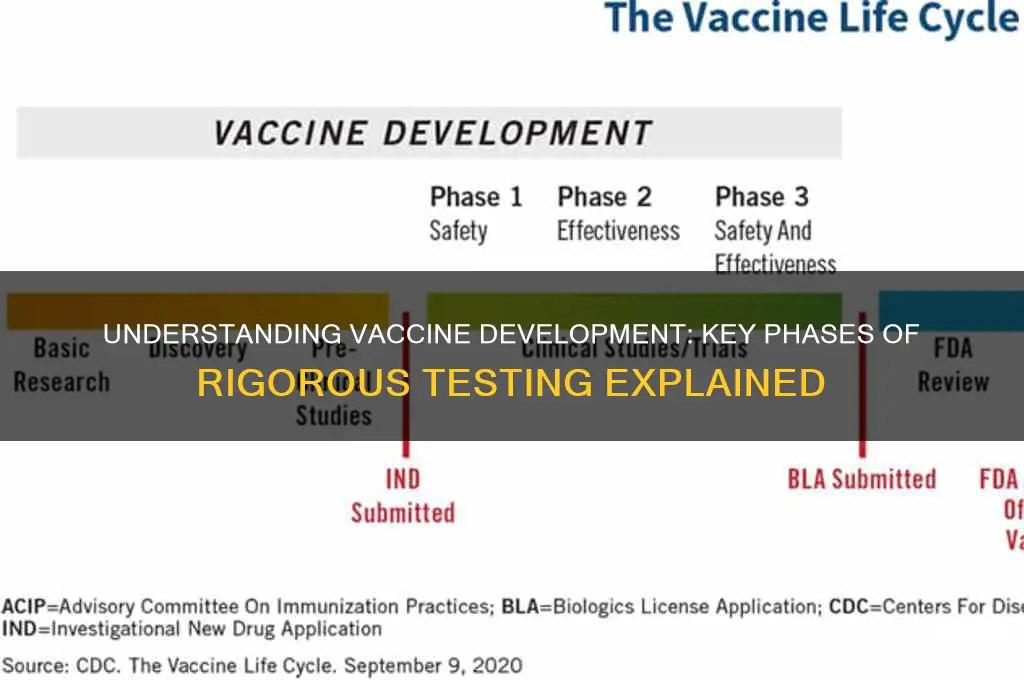
Vaccine development is a rigorous and multi-stage process designed to ensure safety, efficacy, and quality before a vaccine is approved for public use. The phases of vaccine testing typically include preclinical studies, where potential vaccines are tested in laboratory and animal models to assess safety and immune response, followed by three clinical trial phases in humans. Phase 1 focuses on safety, dosage, and initial immune response in a small group of healthy volunteers. Phase 2 expands testing to a larger group to evaluate efficacy, refine dosage, and monitor side effects. Phase 3 involves thousands of participants to confirm efficacy, identify rare side effects, and compare the vaccine to a placebo or existing vaccine. After successful completion of these phases, regulatory authorities review the data before approving the vaccine for public use, followed by Phase 4, which monitors long-term safety and effectiveness in the general population. Each phase is critical to ensuring the vaccine is both safe and effective.
Explore related products

$248.78 $84.99





What You'll Learn
- Pre-clinical Testing: Lab and animal studies to assess safety and immune response
- Phase 1 Trials: Small human trials to evaluate safety and dosage
- Phase 2 Trials: Expanded trials to assess efficacy and side effects
- Phase 3 Trials: Large-scale testing to confirm effectiveness and monitor risks
- Post-Approval Monitoring: Ongoing surveillance for long-term safety and efficacy
![]()
Pre-clinical Testing: Lab and animal studies to assess safety and immune response
Before a vaccine candidate ever reaches human trials, it undergoes rigorous pre-clinical testing, a critical phase that lays the groundwork for its safety and efficacy. This stage is where the vaccine’s potential is scrutinized in controlled environments, using laboratory and animal studies to predict how it might perform in humans. The goal is twofold: to ensure the vaccine does not cause harm and to confirm it triggers a desirable immune response. Without this foundational step, advancing to human trials would be reckless, risking unnecessary exposure to untested substances.
In the lab, scientists begin by testing the vaccine’s components in cell cultures, often using human or animal cells to simulate biological responses. For instance, researchers might expose cells to varying dosages of the vaccine—ranging from micrograms to milligrams—to observe toxicity levels and immune activation. This phase is highly analytical, relying on assays like ELISA (Enzyme-Linked Immunosorbent Assay) to measure antibody production or PCR (Polymerase Chain Reaction) to detect viral or bacterial replication. These tests provide quantitative data, helping researchers refine the vaccine’s formulation before moving to more complex models.
Animal studies are the next critical step, offering a bridge between in vitro experiments and human trials. Typically, small animals like mice or rats are used initially, followed by larger species such as rabbits, monkeys, or ferrets, depending on the vaccine’s target. For example, influenza vaccines are often tested in ferrets due to their respiratory systems’ similarity to humans. Animals are administered the vaccine at different dosages—sometimes as low as 0.1 mg or as high as 10 mg—and monitored for adverse reactions, such as inflammation, organ damage, or behavioral changes. Simultaneously, blood samples are analyzed to assess immune response, including the production of antibodies and activation of immune cells. These studies not only evaluate safety but also help determine the optimal dosage and administration route for future phases.
A key consideration in pre-clinical testing is the ethical treatment of animals, governed by strict protocols like the Three Rs (Replace, Reduce, Refine). Researchers must justify the use of animals, minimize their numbers, and ensure their welfare throughout the study. This ethical framework underscores the responsibility inherent in vaccine development, balancing scientific progress with humane practices. For instance, pain management and anesthesia are used when necessary, and studies are designed to end as soon as sufficient data is collected.
The takeaway from pre-clinical testing is its role as a gatekeeper, filtering out unsafe or ineffective vaccine candidates before they reach humans. While lab and animal studies cannot perfectly predict human responses, they provide essential insights into potential risks and benefits. For example, a vaccine that causes severe allergic reactions in animals would likely be halted, preventing unnecessary harm in clinical trials. Conversely, a candidate that induces robust immunity in animal models gains credibility, warranting further investigation. This phase is not just a regulatory hurdle but a vital step in building confidence in a vaccine’s potential to protect public health.
Mastering Surviv.io: Strategies to Outsmart the Secret Banker
You may want to see also
Explore related products






![]()
Phase 1 Trials: Small human trials to evaluate safety and dosage
Phase 1 trials mark the first time a vaccine candidate is tested in humans, a critical step that bridges the gap between laboratory research and broader clinical application. Typically involving 20 to 100 healthy volunteers, these trials are designed to answer two fundamental questions: Is the vaccine safe, and what dosage is most effective? Participants are closely monitored in a controlled environment, often an inpatient clinic, to detect any immediate adverse reactions. For instance, in the early stages of COVID-19 vaccine development, Phase 1 trials assessed doses ranging from 10 to 250 micrograms, with researchers observing for symptoms like fever, fatigue, or injection site pain.
The process is deliberate and methodical, often employing a dose-escalation strategy. Volunteers are divided into groups, each receiving a different dose of the vaccine. The lowest dose is administered first, and only if it proves safe is the next higher dose tested. This stepwise approach minimizes risk and ensures that potentially harmful doses are not given to a larger group. For example, in a Phase 1 trial for a dengue vaccine, participants were initially given 10 micrograms, then 20, and finally 50 micrograms, with safety data reviewed at each stage before proceeding.
While safety is the primary focus, Phase 1 trials also provide early insights into the vaccine’s immunogenicity—its ability to provoke an immune response. Blood samples are taken at regular intervals to measure antibody levels and other immune markers. However, these trials are not designed to determine efficacy, as the sample size is too small and the study duration too short. Instead, they lay the groundwork for larger, more definitive trials by identifying the optimal dose that balances safety and immune response.
Practical considerations for participants include strict inclusion criteria, such as age (typically 18–55 years), absence of chronic illnesses, and no history of severe allergic reactions. Volunteers are often compensated for their time and may need to commit to multiple visits over several weeks. For researchers, the challenge lies in balancing speed and caution, as rushing this phase can lead to oversight of critical safety issues, while undue delay can stall progress in addressing urgent public health needs.
In summary, Phase 1 trials are a careful, controlled exploration of a vaccine’s safety and dosage in humans. They are the first real-world test of years of laboratory work, providing essential data to guide subsequent phases. While limited in scope, these trials are indispensable, ensuring that only the safest and most promising candidates advance to larger studies. For both participants and researchers, they represent a critical step in the journey from lab to clinic.
How to Transfer Bitcoin to Your Bank Account Using BitGo
You may want to see also
Explore related products






![]()
Phase 2 Trials: Expanded trials to assess efficacy and side effects
Phase 2 trials mark a critical juncture in vaccine development, expanding the scope of testing to hundreds of participants to rigorously evaluate both safety and efficacy. Unlike Phase 1, which focuses on a small, healthy cohort, Phase 2 introduces diversity by including individuals from varying age groups, ethnicities, and sometimes those with underlying health conditions. This broader demographic representation is essential to understanding how the vaccine performs across different populations, ensuring its effectiveness isn't limited to a narrow subset of people. For instance, a vaccine might be tested in adults aged 18–55, followed by a separate cohort of seniors over 65, whose immune responses often differ significantly.
One of the primary objectives of Phase 2 is to determine the optimal dosage. Researchers test multiple dose levels—for example, 25 µg, 50 µg, and 100 µg—to identify the lowest effective dose that elicits a robust immune response without causing undue side effects. This step is both scientific and practical: a lower dose reduces the risk of adverse reactions and can lower production costs, making the vaccine more accessible globally. Participants are closely monitored for side effects, such as fever, fatigue, or injection site pain, which are documented to refine the vaccine's safety profile.
Efficacy assessment in Phase 2 often involves measuring immune responses, such as antibody levels or T-cell activation, rather than direct exposure to the pathogen. For example, in a COVID-19 vaccine trial, researchers might measure neutralizing antibody titers 28 days after the second dose to predict protective immunity. This phase also explores the vaccine's immunogenicity in specific subgroups, like immunocompromised individuals or pregnant women, who are often excluded from earlier trials. Practical tips for participants include maintaining a symptom diary and adhering strictly to follow-up schedules to ensure accurate data collection.
Despite its expanded scale, Phase 2 is not without challenges. Balancing speed and thoroughness is critical, as rushing through this phase can lead to oversight of rare but serious side effects. For instance, a rare allergic reaction occurring in 1 in 10,000 participants might go undetected without careful monitoring. Additionally, placebo-controlled designs, where some participants receive a saline injection, raise ethical questions when an effective vaccine is already available for the disease in question. Researchers must navigate these complexities while ensuring transparency and participant safety.
In conclusion, Phase 2 trials serve as a bridge between initial safety studies and large-scale efficacy trials, refining the vaccine's dosage, identifying potential side effects, and assessing its immunogenicity across diverse populations. By addressing these critical questions, Phase 2 lays the groundwork for Phase 3, where the vaccine's real-world effectiveness is finally put to the test. For stakeholders, from researchers to participants, understanding this phase underscores the meticulous process behind every approved vaccine.
Master Net Banking: A Step-by-Step Guide to Paying Bills Online
You may want to see also
Explore related products



$101.39 $171.95

$149.99 $176.95


![]()
Phase 3 Trials: Large-scale testing to confirm effectiveness and monitor risks
Phase 3 trials are the crucible where a vaccine’s promise meets real-world scrutiny. Involving tens of thousands of volunteers, often across multiple countries, this stage is designed to confirm whether the vaccine works as intended and to identify rare side effects that smaller trials might miss. For instance, the COVID-19 vaccine trials in 2020 enrolled over 30,000 participants each, ensuring diverse representation in age, ethnicity, and health status. This scale is critical because it mirrors the vaccine’s eventual use in the general population, where variability is the norm, not the exception.
Consider the logistics: participants are randomly assigned to receive either the vaccine or a placebo, with neither they nor the researchers knowing who gets which until the trial’s end. This double-blind design minimizes bias. Volunteers are monitored for months, sometimes up to two years, to assess both short-term reactions (e.g., soreness at the injection site) and long-term outcomes (e.g., sustained immunity). For example, in the Pfizer-BioNTech COVID-19 trial, participants received two doses 21 days apart, and efficacy was measured starting seven days after the second dose. Such precision in dosing and timing is non-negotiable, as it directly impacts the trial’s conclusions.
One of the most persuasive arguments for Phase 3 trials is their ability to detect rare but serious adverse events. While Phase 1 and 2 trials might involve a few hundred to a few thousand participants, their size limits their ability to uncover risks that occur in 1 in 10,000 people. Phase 3 trials, by contrast, are statistically powered to catch these anomalies. For example, the Johnson & Johnson COVID-19 vaccine trial identified a rare blood clotting issue in approximately 7 per 1 million vaccinated women aged 18–49. This finding, though concerning, underscores the trial’s success in balancing efficacy and safety.
Practical tips for participants are essential. Volunteers should keep a detailed symptom diary, noting even minor changes like fatigue or headaches. They must also adhere strictly to follow-up schedules, as missed appointments can skew results. For parents enrolling children, it’s crucial to understand age-specific protocols—some trials exclude those under 18, while others focus exclusively on pediatric populations. Transparency with researchers about pre-existing conditions is equally vital, as these can influence both vaccine response and side effect profiles.
In conclusion, Phase 3 trials are not just about confirming what we hope to be true; they’re about uncovering what we need to know. Their large scale and rigorous design provide the definitive evidence required for regulatory approval, ensuring that vaccines are both effective and safe for widespread use. Without this phase, even the most promising candidates would remain speculative, not solutions.
Should You Get Two Pneumovax 23 Vaccines? Expert Insights
You may want to see also
Explore related products






![]()
Post-Approval Monitoring: Ongoing surveillance for long-term safety and efficacy
Vaccine approval marks a significant milestone, but it’s not the end of the road. Post-approval monitoring is a critical phase that ensures long-term safety and efficacy, addressing rare side effects or unforeseen interactions that clinical trials, limited by size and duration, might miss. This ongoing surveillance is a cornerstone of public health, providing real-world data that can inform dosage adjustments, age-specific recommendations, and even vaccine reformulations. For instance, the COVID-19 vaccines underwent rapid post-approval monitoring, leading to booster dose recommendations and age-specific guidelines, such as lower dosages for children aged 5–11.
One key tool in post-approval monitoring is pharmacovigilance systems, which collect and analyze adverse event reports from healthcare providers and the public. These systems, like the CDC’s Vaccine Adverse Event Reporting System (VAERS) or the WHO’s VigiBase, rely on voluntary reporting but are complemented by active surveillance programs. For example, the Vaccine Safety Datalink (VSD) in the U.S. continuously monitors electronic health records of over 12 million people, enabling rapid detection of potential safety signals. Practical tip: Healthcare providers should report any unusual reactions, even if uncertain of causation, to ensure comprehensive data collection.
Another layer of post-approval monitoring involves phase IV studies, which are optional but often conducted to assess long-term outcomes in diverse populations. These studies might explore how a vaccine performs in specific groups, such as pregnant individuals, the immunocompromised, or those with chronic conditions. For the HPV vaccine, post-approval studies confirmed its efficacy in preventing cervical cancer over a decade, leading to expanded recommendations for adults up to age 45. Comparative analysis shows that vaccines like the flu shot require annual monitoring due to evolving strains, while others, like the measles vaccine, are monitored for rare but serious complications like vaccine-associated thrombocytopenia.
A critical takeaway is that post-approval monitoring is not just about identifying problems—it’s about optimizing vaccine use. For instance, data from this phase can justify extending vaccine shelf life, reducing dosage in certain populations, or even discontinuing a vaccine if risks outweigh benefits. The rotavirus vaccine, initially linked to intussusception in rare cases, was reformulated and reintroduced with strict age restrictions (first dose before 15 weeks, last dose before 32 weeks) to maximize safety. This iterative process underscores the dynamic nature of vaccine science, where monitoring is as vital as development.
Instructively, individuals can contribute to post-approval monitoring by staying informed and participating in reporting systems. For parents, keeping vaccination records and noting any reactions can aid healthcare providers in accurate reporting. For policymakers, investing in robust surveillance infrastructure ensures that vaccines remain safe and effective for all. Ultimately, post-approval monitoring is not a passive phase but an active commitment to public health, ensuring that vaccines continue to protect populations long after they leave the lab.
How Foreign Central Banks Purchase U.S. Dollars: A Comprehensive Guide
You may want to see also
Frequently asked questions
Vaccine testing typically involves three phases: Phase 1 focuses on safety and dosage in a small group of healthy volunteers; Phase 2 expands to a larger group to assess safety, immunogenicity (ability to provoke an immune response), and optimal dosage; Phase 3 involves thousands of participants to evaluate efficacy, safety, and side effects in a real-world setting.
The duration of each phase varies, but generally, Phase 1 takes several months, Phase 2 lasts 6–12 months, and Phase 3 can take 1–4 years, depending on the disease, vaccine type, and trial design.
After successful Phase 3 trials, the vaccine developer submits data to regulatory authorities (e.g., FDA, WHO) for approval or authorization. If approved, the vaccine enters Phase 4 (post-market surveillance) to monitor long-term safety and effectiveness in the general population.