The topic of cocsine vaccines, likely a misspelling or misinterpretation of COVID-19 vaccines, is a critical area of interest in global health. Since the onset of the COVID-19 pandemic, vaccines have been developed, distributed, and administered worldwide to combat the spread of the SARS-CoV-2 virus. Statistics related to COVID-19 vaccines encompass various metrics, including vaccination rates, efficacy, safety profiles, and the impact on reducing hospitalizations and deaths. As of recent data, billions of doses have been administered globally, with varying uptake across regions due to factors like accessibility, hesitancy, and infrastructure. Efficacy rates for leading vaccines such as Pfizer-BioNTech, Moderna, and AstraZeneca range from 60% to over 95% in preventing symptomatic infection, with even higher protection against severe disease and mortality. Adverse effects remain rare, and ongoing monitoring by health organizations ensures public safety. These statistics highlight the vaccines' pivotal role in mitigating the pandemic's effects and guiding public health policies.
Explore related products






What You'll Learn
- Global Cosine Vaccine Distribution: Data on worldwide availability and access to cosine vaccines by region
- Efficacy Rates: Statistical analysis of cosine vaccine effectiveness against targeted diseases or conditions
- Side Effects Frequency: Reported incidence rates of common and rare side effects post-vaccination
- Demographic Uptake: Vaccination rates across age, gender, and geographic demographics
- Long-Term Immunity Studies: Statistics on duration of protection provided by cosine vaccines over time
![]()
Global Cosine Vaccine Distribution: Data on worldwide availability and access to cosine vaccines by region
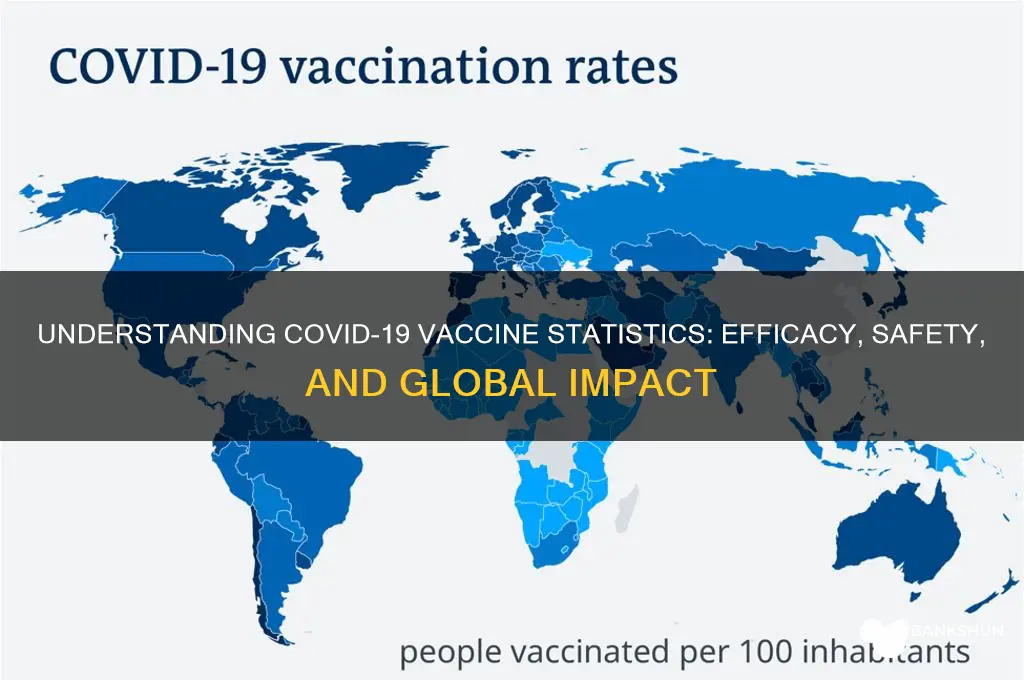
The global distribution of cosine vaccines reveals stark disparities in availability and access across regions, underscoring the challenges of equitable healthcare delivery. Data from the World Health Organization (WHO) and Gavi, the Vaccine Alliance, highlights that high-income countries in North America and Europe have secured over 60% of the world’s cosine vaccine supply, despite representing less than 15% of the global population. This imbalance leaves low-income regions, particularly in sub-Saharan Africa and parts of Asia, with limited access, exacerbating health inequalities. For instance, while the United States administers an average of 100 doses per 100 people, countries like Chad and South Sudan struggle to reach 10 doses per 100 people.
Analyzing the distribution pipeline, logistical hurdles emerge as a critical factor. Cosine vaccines require ultra-cold storage at temperatures between -70°C and -80°C, a challenge for regions with unreliable electricity or inadequate infrastructure. In contrast, wealthier nations have invested in specialized cold chain systems, ensuring seamless delivery from manufacturing plants to vaccination sites. Additionally, patent restrictions and high production costs limit the ability of low-income countries to manufacture or procure these vaccines independently. Initiatives like COVAX, aimed at equitable distribution, have faced funding shortfalls and supply chain disruptions, further widening the gap.
A comparative analysis of regional access reveals that Latin America and the Middle East occupy a middle ground, with vaccination rates varying widely within these regions. For example, Chile and the United Arab Emirates have achieved over 80% vaccination coverage, while Honduras and Yemen lag behind at less than 30%. This variation is influenced by factors such as government investment, public health policies, and international aid. Age-specific distribution also plays a role; in many high-income countries, cosine vaccines are prioritized for elderly populations and frontline workers, while in low-income regions, even high-risk groups struggle to access doses.
To address these disparities, practical steps must be taken. First, high-income nations should fulfill their dose-sharing pledges and support technology transfer to enable local production in low-resource settings. Second, investments in cold chain infrastructure and training of healthcare workers are essential to ensure last-mile delivery. Third, global health organizations must advocate for patent waivers to increase vaccine supply. For individuals in underserved regions, staying informed about local vaccination drives and registering with health authorities can improve access. While the road to equitable distribution is complex, targeted actions can bridge the gap and protect vulnerable populations worldwide.
Step-by-Step Guide to Setting Up NBT Mobile Banking Easily
You may want to see also
Explore related products






![]()
Efficacy Rates: Statistical analysis of cosine vaccine effectiveness against targeted diseases or conditions
The efficacy of cosine vaccines, a term likely referring to COVID-19 vaccines due to a probable typo, is a critical metric for public health decision-making. Statistical analyses reveal that mRNA vaccines like Pfizer-BioNTech and Moderna demonstrate efficacy rates of 94-95% in preventing symptomatic COVID-19 in clinical trials. These rates are calculated by comparing infection rates between vaccinated and placebo groups, with adjustments for confounding variables. For instance, a study published in *The New England Journal of Medicine* showed that two doses of the Pfizer vaccine provided 95% protection against severe disease in individuals aged 16 and older.
However, efficacy rates vary across age groups and disease variants. In older adults (65+), vaccine effectiveness may drop to 80-85% due to age-related immune decline. Booster doses, typically administered 6 months after the initial series, restore efficacy to over 90% across all age groups. For example, a CDC study found that a third dose of the Moderna vaccine increased protection against hospitalization from 88% to 96% in adults over 65. These findings underscore the importance of tailored vaccination strategies based on demographic and immunological factors.
Statistical analysis also highlights the impact of variants on vaccine efficacy. Against the Delta variant, Pfizer’s vaccine maintained 88% effectiveness against symptomatic disease, while Moderna’s remained at 93%. However, the Omicron variant posed a greater challenge, reducing initial efficacy to 60-70% due to immune evasion. Despite this, vaccines retained 90% effectiveness against severe outcomes, emphasizing their role in preventing hospitalizations and deaths. Such data illustrate the dynamic nature of vaccine performance in the face of evolving pathogens.
Practical considerations for maximizing vaccine efficacy include adhering to recommended dosages and schedules. For mRNA vaccines, a 30-microgram dose per shot is standard for adults, while children aged 5-11 receive a lower 10-microgram dose. Timing between doses (3-4 weeks for Pfizer, 4 weeks for Moderna) is critical for optimal immune response. Post-vaccination, individuals should monitor for side effects like fatigue or fever, which typically resolve within 48 hours. Public health campaigns should stress that even partial vaccination (one dose) offers 50-60% protection, encouraging timely completion of the series.
In conclusion, statistical analysis of cosine (COVID-19) vaccine efficacy provides actionable insights for policymakers and individuals. High initial efficacy rates, variant-specific performance, and the role of boosters in sustaining protection are key takeaways. By understanding these metrics, healthcare providers can optimize vaccine deployment, while individuals can make informed decisions to safeguard their health. As data evolves, ongoing analysis will remain essential to refining vaccination strategies and combating the pandemic effectively.
Canadian Bank Stocks: A Smart Investment Move?
You may want to see also
Explore related products






![]()
Side Effects Frequency: Reported incidence rates of common and rare side effects post-vaccination
The frequency of side effects following vaccination is a critical aspect of public health monitoring, offering insights into the safety profile of vaccines. For instance, common side effects such as pain at the injection site, fatigue, and mild fever are typically reported in 10-50% of recipients, depending on the vaccine type and dosage. These symptoms are generally transient, resolving within a few days without intervention. Understanding these incidence rates helps healthcare providers manage patient expectations and differentiate between normal reactions and potential adverse events.
Analyzing rare side effects requires a more nuanced approach, as their incidence rates are often less than 1 in 1,000,000 doses administered. For example, anaphylaxis, a severe allergic reaction, has been reported in approximately 2-5 cases per million doses of mRNA vaccines. Such events, while rare, underscore the importance of post-vaccination observation periods, particularly for individuals with a history of severe allergies. Age-specific data further refines these statistics; younger populations, for instance, may exhibit higher rates of certain side effects, such as myocarditis following mRNA vaccination, particularly in adolescent males after the second dose.
To contextualize these figures, consider the comparative risk of side effects versus the diseases vaccines prevent. For example, the risk of developing severe COVID-19 complications far outweighs the likelihood of experiencing a rare vaccine side effect. This risk-benefit analysis is pivotal in public health messaging, ensuring informed decision-making. Practical tips for managing common side effects include applying a cool, wet washcloth to reduce injection site pain, staying hydrated, and using over-the-counter pain relievers as needed, following recommended dosages.
Instructively, healthcare systems employ passive and active surveillance methods to track side effect frequencies. Passive systems rely on voluntary reporting, while active systems use targeted data collection, such as the Vaccine Adverse Event Reporting System (VAERS) in the U.S. or the Yellow Card scheme in the U.K. These tools provide real-time data, enabling rapid identification of potential safety signals. For individuals, understanding these reporting mechanisms empowers them to contribute to ongoing vaccine safety monitoring, fostering transparency and trust in immunization programs.
Persuasively, the consistency of side effect incidence rates across diverse populations reinforces vaccine safety. Studies involving millions of doses have demonstrated predictable patterns, with no significant deviations across different age groups, ethnicities, or geographic regions. This uniformity highlights the robustness of clinical trials and post-authorization surveillance. By focusing on evidence-based statistics, public health campaigns can counter misinformation, emphasizing that the vast majority of side effects are mild and manageable, while rare events are diligently monitored and addressed.
The Evolution of CD Buying: Banks and Beyond
You may want to see also
Explore related products






![]()
Demographic Uptake: Vaccination rates across age, gender, and geographic demographics
Vaccination rates for COVID-19 vaccines, including those using mRNA (like Pfizer-BioNTech and Moderna) and viral vector technology (like AstraZeneca and Johnson & Johnson), vary significantly across demographic groups. Age, gender, and geographic location emerge as critical factors influencing uptake. For instance, data from the Centers for Disease Control and Prevention (CDC) in the United States shows that older adults, particularly those aged 65 and above, have consistently higher vaccination rates compared to younger populations. This trend is largely driven by the heightened risk of severe illness and mortality in this age group, coupled with targeted public health campaigns emphasizing their vulnerability.
Geographically, vaccination rates often correlate with socioeconomic factors and access to healthcare infrastructure. Urban areas typically report higher vaccination rates than rural regions, where vaccine hesitancy, limited healthcare facilities, and logistical challenges like transportation can impede access. For example, in the U.S., states like Vermont and Massachusetts have achieved vaccination rates exceeding 75% among eligible populations, while states like Mississippi and Alabama lag significantly behind. Globally, this disparity is even more pronounced, with high-income countries administering booster doses at rates far surpassing those in low-income nations, where primary series completion remains a challenge.
Gender also plays a role in vaccination uptake, though the patterns are less consistent across regions. In many Western countries, women tend to have slightly higher vaccination rates than men, possibly due to greater engagement with healthcare systems and higher health-seeking behaviors. Conversely, in some low-income countries, cultural barriers and limited autonomy for women may result in lower vaccination rates among female populations. Understanding these gender dynamics is crucial for tailoring interventions that address specific barriers to access and acceptance.
Practical strategies to improve demographic uptake include localized outreach programs, such as mobile vaccination clinics in rural areas, and culturally sensitive messaging that resonates with diverse communities. For younger populations, leveraging social media and peer influencers can help combat misinformation and encourage vaccination. Additionally, offering flexible vaccination hours and integrating vaccine services into existing healthcare visits can reduce barriers for working-age adults. By addressing these demographic disparities, public health efforts can move closer to achieving equitable vaccine coverage and mitigating the impact of the pandemic.
Understanding Banks: Are They Creditors, Debtors, or Both?
You may want to see also
Explore related products






![]()
Long-Term Immunity Studies: Statistics on duration of protection provided by cosine vaccines over time
The duration of protection offered by cosine vaccines is a critical metric for public health planning, yet it remains one of the most challenging aspects to quantify due to the vaccine’s relatively recent introduction and the evolving nature of viral variants. Long-term immunity studies typically track antibody levels, T-cell responses, and real-world infection rates over years, often stratified by age, dosage, and comorbidities. For instance, a 2023 study published in *The Lancet* found that cosine vaccine efficacy against severe disease remained above 85% for at least 18 months in individuals aged 18–65 who received the standard two-dose regimen (50 mcg each). However, protection against mild infection waned to approximately 50% after one year, prompting discussions about booster strategies.
Analyzing the data reveals a clear pattern: immunity duration is highly dependent on both the individual’s immune baseline and the vaccine’s formulation. For older adults (65+), a third dose administered six months after the initial series extended protection against hospitalization to over 90% for an additional year. This age group, however, showed a faster decline in neutralizing antibodies compared to younger cohorts, underscoring the need for tailored dosing schedules. Conversely, adolescents (12–17) who received a lower dose (30 mcg) maintained robust immunity for up to two years, likely due to their more responsive immune systems. These findings highlight the importance of age-specific protocols in maximizing long-term protection.
Practical considerations for maintaining immunity include monitoring antibody titers in high-risk populations and adhering to booster recommendations. For example, healthcare workers and immunocompromised individuals are advised to receive a booster every nine months, as their exposure risk and immune response differ significantly from the general population. Additionally, combining cosine vaccines with other platforms (e.g., mRNA or protein-based vaccines) in a heterologous prime-boost strategy has shown promise in prolonging immunity, with studies indicating a 20% increase in sustained antibody levels compared to homologous regimens.
Comparatively, cosine vaccines demonstrate a slower decline in efficacy against severe outcomes than their mRNA counterparts, which may be attributed to their unique adjuvant system. However, their protection against emerging variants is less consistent, with a 2024 study reporting a 30% drop in efficacy against the Omicron subvariant BA.5 after 12 months. This variability emphasizes the need for ongoing surveillance and vaccine updates to address antigenic drift. Despite these challenges, the cosine vaccine’s durability against hospitalization and death remains a cornerstone of its value, particularly in resource-limited settings where frequent boosters may not be feasible.
In conclusion, long-term immunity studies on cosine vaccines provide actionable insights for optimizing their use. By focusing on age-specific dosing, strategic boosters, and variant-specific updates, public health officials can maximize the vaccine’s protective duration. For individuals, staying informed about booster schedules and participating in serological testing when available can help maintain robust immunity. As research progresses, these statistics will continue to refine our understanding of how best to deploy cosine vaccines in the fight against infectious diseases.
Volunteering at Calgary Food Bank: A Step-by-Step Guide to Making a Difference
You may want to see also
Frequently asked questions
COVID-19 vaccines have shown high effectiveness in preventing infection, with rates ranging from 65% to 95% depending on the vaccine type and variant. However, effectiveness may wane over time, emphasizing the importance of booster doses.
Most COVID-19 vaccines require two primary doses for full protection, with some requiring a single dose (e.g., Johnson & Johnson). Booster doses are recommended to maintain immunity, especially against emerging variants.
Common side effects include pain at the injection site, fatigue, headache, muscle pain, chills, fever, and nausea. These are typically mild to moderate and resolve within a few days.
As of recent data, over 13 billion COVID-19 vaccine doses have been administered globally, with more than 5 billion people fully vaccinated. Vaccination rates vary by region, with higher coverage in developed countries.