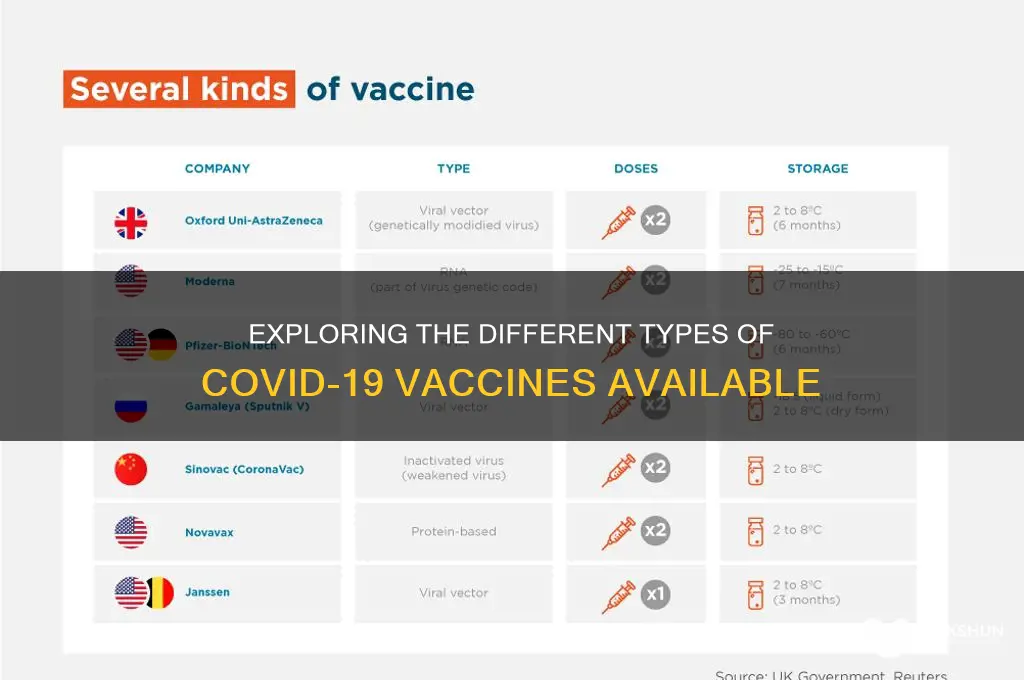
The COVID-19 pandemic has led to the rapid development and deployment of multiple vaccines to combat the SARS-CoV-2 virus. These vaccines fall into several distinct types, each utilizing different technologies to elicit an immune response. The primary categories include mRNA vaccines, such as Pfizer-BioNTech and Moderna, which use genetic material to instruct cells to produce a viral protein, triggering immunity. Viral vector vaccines, like AstraZeneca and Johnson & Johnson, employ a harmless virus to deliver genetic instructions to cells. Protein subunit vaccines, exemplified by Novavax, contain harmless pieces of the virus to stimulate an immune response. Additionally, inactivated or weakened virus vaccines, commonly used in countries like China and India, introduce a non-infectious form of the virus to build immunity. Understanding these types is crucial for informed decision-making and global vaccination efforts.
| Characteristics | Values |
|---|---|
| Types of COVID-19 Vaccines | mRNA, Viral Vector, Protein Subunit, Inactivated Virus, DNA |
| mRNA Vaccines | Pfizer-BioNTech (Comirnaty), Moderna (Spikevax) |
| Mechanism (mRNA) | Delivers genetic material to cells to produce spike protein, triggering immune response |
| Viral Vector Vaccines | Oxford-AstraZeneca (Vaxzevria), Johnson & Johnson (Janssen) |
| Mechanism (Viral Vector) | Uses a modified virus to deliver genetic material for spike protein production |
| Protein Subunit Vaccines | Novavax (Nuvaxovid) |
| Mechanism (Protein Subunit) | Contains harmless pieces of the virus (spike protein) to induce immunity |
| Inactivated Virus Vaccines | Sinovac (CoronaVac), Sinopharm (BBIBP-CorV) |
| Mechanism (Inactivated Virus) | Uses killed virus particles to trigger an immune response |
| DNA Vaccines | Zydus Cadila (ZyCoV-D) |
| Mechanism (DNA) | Delivers DNA instructions to cells to produce spike protein |
| Efficacy (Approx.) | mRNA: 90-95%, Viral Vector: 60-90%, Protein Subunit: 80-90%, Inactivated: 50-80%, DNA: 67% |
| Dose Regimen | Typically 2 doses (mRNA, Viral Vector, Protein Subunit), 1 dose (J&J), 3 doses (ZyCoV-D) |
| Storage Requirements | mRNA: Ultra-cold (-70°C to -20°C), Others: Standard refrigeration (2-8°C) |
| Common Side Effects | Pain at injection site, fatigue, headache, muscle pain, fever |
| Approval Status | Varies by country; most are WHO-approved or authorized for emergency use |
| Booster Recommendations | Recommended for enhanced immunity, especially against variants |
Explore related products





What You'll Learn
- mRNA Vaccines: Pfizer-BioNTech, Moderna use genetic material to trigger immune response against COVID-19
- Viral Vector Vaccines: AstraZeneca, Johnson & Johnson use modified viruses to deliver COVID-19 proteins
- Protein Subunit Vaccines: Novavax uses harmless COVID-19 spike proteins to induce immunity
- Inactivated Vaccines: Sinovac, Sinopharm use killed COVID-19 viruses to stimulate immune response
- DNA Vaccines: Experimental type uses DNA to produce COVID-19 proteins for immunity
![]()
mRNA Vaccines: Pfizer-BioNTech, Moderna use genetic material to trigger immune response against COVID-19
MRNA vaccines represent a groundbreaking approach in the fight against COVID-19, with Pfizer-BioNTech and Moderna leading the charge. Unlike traditional vaccines that use weakened viruses or viral proteins, these vaccines deliver genetic material—specifically, messenger RNA (mRNA)—into cells to instruct them to produce a harmless piece of the SARS-CoV-2 spike protein. This triggers a robust immune response, preparing the body to recognize and combat the actual virus. The Pfizer-BioNTech vaccine, administered in a two-dose series 21 days apart, requires ultra-cold storage due to its mRNA fragility, while Moderna’s vaccine offers slightly more flexibility with a 28-day interval and less stringent storage conditions.
The efficacy of mRNA vaccines is remarkable, with both Pfizer-BioNTech and Moderna reporting around 95% effectiveness in preventing symptomatic COVID-19 in clinical trials. For Pfizer, the dosage is 30 micrograms per shot for individuals aged 12 and older, while Moderna administers 100 micrograms for adults and a lower dose for adolescents. Booster shots have become essential to maintain immunity, especially against emerging variants. These vaccines are particularly advantageous because their mRNA technology allows for rapid adaptation to new strains, a critical feature in the ever-evolving pandemic landscape.
One of the most compelling aspects of mRNA vaccines is their safety profile. Common side effects, such as fatigue, headache, and muscle pain, are mild and short-lived, indicating the immune system’s active response. Rare cases of myocarditis, primarily in young males after the second dose, have been reported but are typically resolved with minimal intervention. For parents, Pfizer’s vaccine is the only mRNA option approved for children aged 5–11, with a lower dosage of 10 micrograms per shot, ensuring safety and efficacy in this age group.
Practical considerations for receiving an mRNA vaccine include scheduling flexibility for potential side effects after the second dose and ensuring access to a healthcare provider if needed. It’s also crucial to follow local guidelines for booster shots, as recommendations may vary based on age, health status, and regional virus circulation. While mRNA vaccines have been a cornerstone of global vaccination efforts, their success underscores the importance of continued research and public trust in scientific innovation. By understanding how these vaccines work and their unique benefits, individuals can make informed decisions to protect themselves and their communities.
Banking Bias: How Financial Systems Marginalize the Poor
You may want to see also
Explore related products






![]()
Viral Vector Vaccines: AstraZeneca, Johnson & Johnson use modified viruses to deliver COVID-19 proteins
Viral vector vaccines represent a clever approach to immunization, leveraging the body's natural response to viral invaders. AstraZeneca and Johnson & Johnson’s COVID-19 vaccines exemplify this technology, using modified, harmless viruses (adenoviruses) as vehicles to deliver genetic instructions for producing the SARS-CoV-2 spike protein. Once injected, these vectors enter cells, prompting the immune system to recognize and combat the foreign protein, thereby building immunity without causing illness. This method combines the precision of genetic delivery with the robustness of a traditional immune response.
Mechanism and Administration
Both vaccines require a two-dose regimen, though Johnson & Johnson’s is unique in offering single-dose protection. AstraZeneca’s vaccine, administered in two doses 4–12 weeks apart, uses a chimpanzee adenovirus (ChAdOx1) as its vector, while Johnson & Johnson employs a human adenovirus (Ad26). The latter’s single-dose convenience made it particularly valuable in hard-to-reach populations or areas with limited healthcare access. Storage requirements further differentiate them: AstraZeneca’s vaccine is stable in standard refrigerators (2–8°C), whereas Johnson & Johnson’s can withstand higher temperatures (up to 25°C for 12 hours), enhancing its distribution flexibility.
Efficacy and Safety
Clinical trials demonstrated AstraZeneca’s vaccine to be 76% effective against symptomatic COVID-19 and 100% effective against severe disease and hospitalization after two doses. Johnson & Johnson’s single-dose vaccine showed 66% efficacy globally, rising to 85% against severe disease. Both vaccines have been linked to rare side effects, such as thrombosis with thrombocytopenia syndrome (TTS), occurring in approximately 1 in 100,000 recipients, predominantly in younger adults. Health authorities recommend monitoring for symptoms like persistent headaches or abdominal pain post-vaccination, particularly within 2–3 weeks of receiving the jab.
Practical Considerations
For individuals aged 18 and older, these vaccines offer viable alternatives to mRNA options, especially in regions with limited access to ultra-cold storage. Pregnant individuals and those with a history of blood clots should consult healthcare providers before vaccination. Notably, AstraZeneca’s vaccine has been authorized in over 170 countries, while Johnson & Johnson’s has been pivotal in global vaccine equity initiatives. Recipients should avoid pain relievers like ibuprofen before vaccination unless medically advised, as they may interfere with immune response.
Comparative Advantage
Viral vector vaccines bridge the gap between traditional and cutting-edge technologies, offering durability and ease of distribution. Unlike mRNA vaccines, they do not require extreme cold storage, making them logistically advantageous in low-resource settings. However, their efficacy rates are generally lower, and the rare but serious side effects necessitate targeted risk communication. For populations prioritizing accessibility and single-dose convenience, these vaccines remain a critical tool in the global fight against COVID-19.
Which Bank Does American Express Partner With for Banking Services?
You may want to see also
Explore related products






![]()
Protein Subunit Vaccines: Novavax uses harmless COVID-19 spike proteins to induce immunity
Protein subunit vaccines represent a precision-focused approach in the fight against COVID-19, and Novavax’s offering stands out by leveraging a key viral component: the SARS-CoV-2 spike protein. Unlike whole-virus vaccines, which use weakened or inactivated pathogens, subunit vaccines contain only the specific protein fragments needed to trigger an immune response. Novavax’s vaccine, known as NVX-CoV2373, isolates the harmless spike proteins of the coronavirus, presenting them to the immune system without introducing any infectious material. This method minimizes risks while maximizing the body’s ability to recognize and combat the virus.
The development of Novavax’s vaccine involved a two-dose regimen, administered 21 days apart, with each dose containing 5 micrograms of the spike protein combined with an adjuvant, Matrix-M. The adjuvant enhances the immune response, ensuring that even a small amount of protein can elicit robust protection. Clinical trials demonstrated that this formulation was 90.4% effective in preventing symptomatic COVID-19 in adults aged 18 and older. Notably, the vaccine’s side effects were mild to moderate, typically limited to pain at the injection site, fatigue, and headaches, making it a well-tolerated option for diverse populations.
One of the key advantages of protein subunit vaccines like Novavax’s is their stability and ease of storage. Unlike mRNA vaccines, which require ultra-cold temperatures, NVX-CoV2373 can be stored at standard refrigerator temperatures (2°C to 8°C). This feature simplifies distribution, particularly in regions with limited access to advanced cold-chain infrastructure. Additionally, the vaccine’s traditional technology, which has been used for decades in vaccines like those for hepatitis B and pertussis, may appeal to individuals hesitant about newer platforms like mRNA.
For practical application, Novavax’s vaccine is suitable for individuals aged 12 and older, with dosage and administration protocols varying slightly by region. In the U.S., for instance, it is authorized for both primary vaccination and booster doses. Recipients should follow post-vaccination guidelines, such as monitoring for allergic reactions and staying hydrated, though serious adverse events are rare. Its approval in over 40 countries underscores its global relevance, offering a reliable alternative in the vaccine landscape.
In summary, Novavax’s protein subunit vaccine exemplifies innovation within a proven framework. By isolating the COVID-19 spike protein and pairing it with an effective adjuvant, it achieves strong immunity with minimal side effects. Its logistical advantages and familiarity with traditional vaccine technology make it a valuable tool in the ongoing pandemic response, particularly for populations seeking an alternative to mRNA or viral vector vaccines. As vaccination efforts continue, Novavax’s contribution highlights the importance of diversity in vaccine platforms to meet global health needs.
Vaccines and Viral Evolution: Are They Strengthening the Virus?
You may want to see also
Explore related products






![]()
Inactivated Vaccines: Sinovac, Sinopharm use killed COVID-19 viruses to stimulate immune response
Inactivated vaccines, such as Sinovac (CoronaVac) and Sinopharm (BBIBP-CorV), harness a time-tested approach to immunization by using killed COVID-19 viruses to trigger an immune response. Unlike live vaccines, these inactivated versions cannot replicate or cause disease, making them a safer option for individuals with compromised immune systems or specific health conditions. This method has been widely used in vaccines for diseases like influenza and polio, establishing a foundation of trust in its efficacy and safety.
The process begins with growing the SARS-CoV-2 virus in a lab, then inactivating it using chemicals like beta-propiolactone. This renders the virus incapable of infection but leaves its structural proteins intact, allowing the immune system to recognize and respond to it. Both Sinovac and Sinopharm vaccines require a two-dose regimen, typically administered 2–4 weeks apart, depending on local health guidelines. For Sinovac, the standard dosage is 3 micrograms per 0.5 mL dose, while Sinopharm uses 4 micrograms per 0.5 mL dose. Booster shots are often recommended 6–12 months after the initial series to enhance immunity, particularly against emerging variants.
One of the key advantages of inactivated vaccines is their stability at standard refrigerator temperatures (2–8°C), making them easier to distribute in regions with limited cold-chain infrastructure. This has been particularly beneficial in low- and middle-income countries, where Sinovac and Sinopharm have been widely deployed. However, their efficacy rates, typically ranging from 50–80% depending on the study, are generally lower than mRNA vaccines. This has sparked debates about their effectiveness, especially against highly transmissible variants like Omicron.
For practical use, recipients should be aware of potential side effects, which are usually mild and include soreness at the injection site, fatigue, and low-grade fever. These symptoms typically resolve within 48 hours. It’s crucial to follow local health authority guidelines regarding eligibility, as these vaccines are often approved for individuals aged 3 and older, though age limits may vary by country. Pregnant or immunocompromised individuals should consult healthcare providers before vaccination to weigh risks and benefits.
In comparison to other vaccine types, inactivated vaccines offer a balance of accessibility and safety, though their efficacy may require supplementation with boosters. Their role in global vaccination efforts cannot be understated, particularly in regions where mRNA vaccines are less available. By understanding their mechanism, dosage, and practical considerations, individuals can make informed decisions about their immunization journey.
Protect Your Savings: Strategies to Avoid Bank Bail-Ins in the UK
You may want to see also
Explore related products






![]()
DNA Vaccines: Experimental type uses DNA to produce COVID-19 proteins for immunity
DNA vaccines represent a cutting-edge approach in the fight against COVID-19, leveraging genetic material to stimulate immunity. Unlike traditional vaccines that introduce a weakened or inactivated virus, DNA vaccines deliver a small, circular piece of DNA called a plasmid. This plasmid contains the genetic instructions for producing a harmless piece of the SARS-CoV-2 spike protein, the key component the virus uses to enter human cells. Once inside the body, the plasmid enters cells, which then read the genetic code and produce the spike protein. This triggers the immune system to recognize and attack the protein, creating a memory response to protect against future COVID-19 infections.
The administration of DNA vaccines typically involves a series of injections, often two doses given several weeks apart. For example, the experimental DNA vaccine developed by Inovio Pharmaceuticals, known as INO-4800, is administered via a device that uses a brief electrical pulse to facilitate DNA uptake into cells. This method, called electroporation, enhances the vaccine’s effectiveness by ensuring the DNA reaches the cell nucleus. While DNA vaccines are still in clinical trials and not yet widely approved for public use, early studies suggest they are safe and capable of eliciting both antibody and T-cell responses, which are crucial for robust immunity.
One of the most compelling advantages of DNA vaccines is their versatility and potential for rapid development. Since they rely on synthesizing DNA sequences rather than growing viruses or cells, they can be produced quickly in response to new variants or emerging pathogens. This makes them a promising tool not only for COVID-19 but also for future pandemics. Additionally, DNA vaccines are stable at higher temperatures compared to mRNA vaccines, which require ultra-cold storage, making them more accessible for distribution in low-resource settings.
However, DNA vaccines are not without challenges. Their efficacy can be limited by the body’s natural barriers to DNA uptake, which is why techniques like electroporation are often necessary. Furthermore, public acceptance may be hindered by skepticism surrounding genetic-based technologies, despite their safety profile in trials. For those considering participation in DNA vaccine trials or awaiting approval, it’s essential to stay informed about the latest research and consult healthcare providers for personalized advice.
In conclusion, DNA vaccines offer a novel and innovative strategy for combating COVID-19 by harnessing the body’s own cellular machinery to build immunity. While still experimental, their potential for scalability, adaptability, and ease of storage positions them as a valuable addition to the global vaccine arsenal. As research progresses, DNA vaccines may not only play a role in ending the current pandemic but also pave the way for next-generation vaccines against other infectious diseases.
Understanding Food Bank Tax Status: Are They 501(c)(3) Organizations?
You may want to see also
Frequently asked questions
The main types of COVID-19 vaccines include mRNA vaccines (e.g., Pfizer-BioNTech, Moderna), viral vector vaccines (e.g., Johnson & Johnson, AstraZeneca), and inactivated virus vaccines (e.g., Sinopharm, Sinovac).
mRNA vaccines (like Pfizer and Moderna) teach cells to produce a harmless protein that triggers an immune response. Viral vector vaccines (like J&J) use a modified virus to deliver genetic material, while inactivated vaccines (like Sinopharm) use a killed version of the virus to build immunity.
While all approved vaccines are effective at preventing severe illness, hospitalization, and death, their efficacy rates vary. mRNA vaccines generally show higher efficacy against symptomatic infection, but all types provide robust protection against severe outcomes.