Vaccine eligibility is often determined by underlying health conditions that may increase an individual's risk of severe illness or complications from certain diseases. These conditions can vary widely and may include chronic illnesses such as heart disease, diabetes, and respiratory disorders, as well as immunocompromised states resulting from conditions like HIV, cancer treatments, or organ transplants. Additionally, age-related vulnerabilities, such as those in young children or older adults, and lifestyle factors like smoking or obesity, can also influence eligibility. Understanding these underlying conditions is crucial for prioritizing vaccine distribution, ensuring that those most at risk receive protection first, and ultimately reducing the burden of preventable diseases on public health systems.
Explore related products






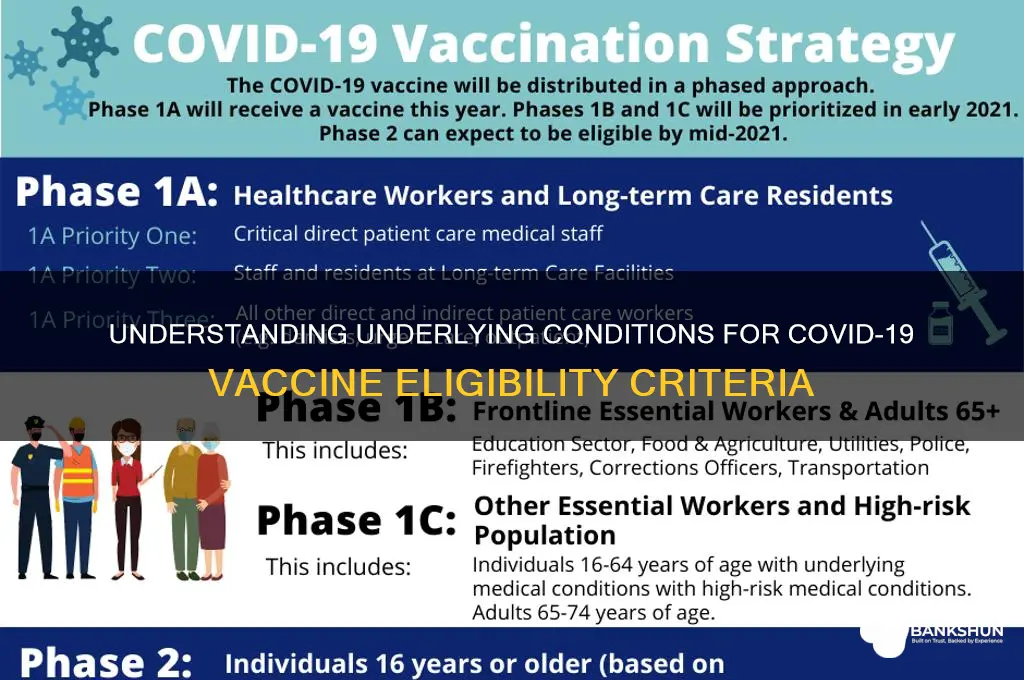
What You'll Learn
- Age Requirements: Specific age groups prioritized based on vulnerability and risk factors
- Health Conditions: Chronic illnesses like diabetes, heart disease, or asthma increase eligibility
- Occupational Risks: Frontline workers, healthcare staff, and essential workers often qualify early
- Immunocompromised Status: Individuals with weakened immune systems are prioritized for protection
- Geographic Considerations: High-risk areas or outbreak zones may influence eligibility criteria
![]()
Age Requirements: Specific age groups prioritized based on vulnerability and risk factors
Vaccine distribution strategies often prioritize age groups based on their vulnerability to severe outcomes from infectious diseases. Older adults, particularly those aged 65 and above, are consistently identified as a high-priority category due to age-related immune system decline, known as immunosenescence. This physiological change increases susceptibility to infections and reduces vaccine efficacy, necessitating tailored dosing or adjuvanted formulations. For instance, high-dose influenza vaccines containing four times the antigen of standard doses are recommended for this demographic to enhance immune response. Similarly, COVID-19 vaccine rollouts in many countries began with individuals aged 80 and older, gradually expanding to younger age brackets as supply increased.
Contrastingly, younger age groups, such as adolescents and young adults, are often prioritized for vaccines targeting diseases with higher transmission rates in these populations. For example, HPV vaccination campaigns focus on individuals aged 9 to 26, with optimal response observed when administered before potential exposure to the virus. This age-specific strategy not only prevents infection but also reduces long-term risks of cervical, oropharyngeal, and other cancers. In some cases, catch-up doses are recommended for individuals who missed the initial vaccination window, though efficacy may be slightly diminished.
Pediatric populations, particularly infants and toddlers, require specialized vaccine schedules due to their developing immune systems. Vaccines like DTaP (diphtheria, tetanus, pertussis) and MMR (measles, mumps, rubella) are administered in multiple doses starting at 2 months of age, with boosters at 4, 6, and 12–15 months. This staggered approach ensures adequate immune memory without overwhelming the immature immune system. Delayed or missed doses necessitate consultation with healthcare providers to determine appropriate catch-up schedules, often involving shorter intervals between doses.
Practical considerations for age-based prioritization include logistical planning and communication strategies. For older adults, vaccination sites may offer accessible locations, such as senior centers or mobile clinics, while younger populations benefit from school-based programs or workplace initiatives. Clear, age-appropriate messaging is essential; for instance, materials for adolescents might emphasize protection for themselves and their communities, while those for older adults focus on reducing hospitalization risks. Caregivers and family members should also be informed about potential side effects and the importance of completing all recommended doses.
In conclusion, age-based prioritization in vaccine eligibility is a nuanced strategy that balances immunological principles with practical implementation. By understanding the unique vulnerabilities and risk factors associated with different age groups, public health efforts can maximize vaccine impact, ensuring protection for those most at risk while fostering herd immunity across populations. Tailored dosing, scheduling, and outreach methods are critical components of this approach, underscoring the importance of age as a determinant in vaccine distribution frameworks.
Free ATM Access: Banks That Don't Charge Withdrawal Fees
You may want to see also
Explore related products






![]()
Health Conditions: Chronic illnesses like diabetes, heart disease, or asthma increase eligibility
Chronic health conditions significantly elevate the risk of severe outcomes from vaccine-preventable diseases, making individuals with these illnesses a priority for immunization. Conditions like diabetes, heart disease, and asthma compromise the body’s ability to fight infections, often due to weakened immune systems or organ dysfunction. For instance, diabetes impairs immune response and increases inflammation, while heart disease can worsen complications from respiratory infections. Asthma, particularly when uncontrolled, heightens susceptibility to severe respiratory illnesses. Recognizing these risks, health authorities universally prioritize individuals with such conditions for vaccine eligibility, ensuring they receive protection against preventable diseases.
Consider the practical implications for someone managing diabetes. Flu vaccines, for example, are recommended annually, with studies showing they reduce hospitalization rates by up to 79% in diabetic patients. Similarly, individuals with heart disease benefit from pneumonia vaccines (PCV13 and PPSV23), which lower the risk of cardiac complications from pneumococcal infections. Asthmatics, especially those requiring daily medication, are urged to receive flu and COVID-19 vaccines, as these illnesses can trigger severe asthma attacks. Dosage and timing vary—adults with chronic conditions typically require standard vaccine doses, but immunocompromised individuals may need additional boosters or adjuvanted formulations for enhanced immunity.
A comparative analysis reveals disparities in vaccine uptake among those with chronic illnesses. Despite eligibility, many delay vaccination due to misconceptions about safety or efficacy. For example, some asthmatics fear vaccines could exacerbate symptoms, though evidence shows no increased risk of asthma attacks post-vaccination. Addressing these concerns requires targeted education, emphasizing that vaccines are rigorously tested in populations with chronic conditions. Healthcare providers play a critical role here, offering personalized advice and dispelling myths to encourage timely immunization.
Persuasively, prioritizing vaccine eligibility for those with chronic illnesses is not just a health measure—it’s a societal imperative. Unvaccinated individuals with these conditions not only face higher mortality rates but also strain healthcare systems during disease outbreaks. By protecting this vulnerable group, we reduce hospitalizations, save lives, and foster herd immunity. Practical tips include scheduling vaccinations during stable health periods, carrying medication lists to appointments, and monitoring for rare side effects like allergic reactions. For caregivers, ensuring regular vaccine updates for dependents with chronic conditions is non-negotiable.
In conclusion, chronic illnesses like diabetes, heart disease, and asthma are not just personal health challenges—they are criteria for prioritized vaccine eligibility. From tailored dosages to myth-busting, the approach to immunizing this group must be informed, empathetic, and proactive. By understanding the unique risks and addressing barriers to access, we can safeguard those most vulnerable and strengthen public health resilience.
How to Deposit or Hold a Cheque in HDFC Bank: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Occupational Risks: Frontline workers, healthcare staff, and essential workers often qualify early
Frontline workers, healthcare staff, and essential workers are often among the first to qualify for vaccines due to their heightened exposure to infectious diseases. These individuals serve as the backbone of society, ensuring that critical services continue even during public health crises. Their roles—whether in hospitals, grocery stores, or public transportation—place them in constant contact with large numbers of people, significantly increasing their risk of infection. Recognizing this, public health authorities prioritize their vaccination to protect both the workers themselves and the communities they serve.
Consider the healthcare sector, where nurses, doctors, and support staff face daily exposure to pathogens. Studies show that healthcare workers are up to three times more likely to contract vaccine-preventable diseases compared to the general population. For instance, during the COVID-19 pandemic, healthcare workers accounted for nearly 10% of all cases in some countries, despite representing less than 3% of the population. Early vaccination not only reduces their risk of severe illness but also minimizes staff shortages that could cripple healthcare systems. Most vaccine protocols recommend a two-dose regimen for this group, with the second dose administered 3–4 weeks after the first, to ensure robust immunity.
Essential workers in other sectors, such as grocery clerks, teachers, and public transit operators, also face elevated risks. Unlike healthcare workers, they may lack access to personal protective equipment (PPE) or work in environments where physical distancing is impractical. For example, a cashier in a busy supermarket interacts with hundreds of customers daily, often in enclosed spaces with poor ventilation. Vaccinating these workers early helps maintain the continuity of essential services and prevents community spread. Practical tips for employers include scheduling vaccinations during shifts to minimize disruption and providing educational materials to address vaccine hesitancy.
Comparatively, the prioritization of these workers highlights a broader principle in public health: protecting those who protect us. While age and underlying health conditions are often the primary criteria for vaccine eligibility, occupational risk serves as a critical secondary factor. For instance, a 30-year-old teacher may qualify for vaccination before a 60-year-old remote worker, despite the latter’s higher age-related risk. This approach reflects a strategic balance between individual vulnerability and societal function.
In conclusion, prioritizing frontline workers, healthcare staff, and essential workers for early vaccination is both a practical and ethical imperative. Their roles place them at the intersection of personal risk and public safety, making their protection a cornerstone of pandemic response. By focusing on occupational risks, public health strategies not only safeguard these workers but also fortify the systems that depend on them. Employers and policymakers must collaborate to ensure seamless vaccine access, from flexible scheduling to on-site clinics, to maximize uptake and minimize barriers.
Are Sasha Banks and Seth Rollins Dating? The Truth Revealed
You may want to see also
Explore related products


$8.54 $14.99




![]()
Immunocompromised Status: Individuals with weakened immune systems are prioritized for protection
Immunocompromised individuals face a heightened risk of severe illness from vaccine-preventable diseases due to their weakened immune systems. Conditions such as HIV/AIDS, cancer treatments, organ transplants, and autoimmune disorders requiring immunosuppressive medications all fall under this category. These individuals often cannot mount a full immune response to infections, making vaccination a critical protective measure. However, not all vaccines are safe or effective for them. For instance, live-attenuated vaccines like the MMR (measles, mumps, rubella) or varicella (chickenpox) vaccines may pose risks and are generally avoided in severely immunocompromised patients.
When vaccinating immunocompromised individuals, timing and dosage adjustments are crucial. For example, those undergoing chemotherapy may need to delay vaccination until their immune system recovers, typically 3–6 months post-treatment. In some cases, additional doses or higher concentrations of vaccines may be recommended to ensure adequate immunity. For instance, individuals with chronic kidney disease or on dialysis often require higher doses of the influenza vaccine or more frequent boosters. Healthcare providers must carefully assess each patient’s condition to tailor vaccination strategies effectively.
A comparative analysis reveals that inactivated vaccines, such as the COVID-19 mRNA vaccines (Pfizer-BioNTech and Moderna) or the hepatitis B vaccine, are generally safe and effective for immunocompromised individuals. These vaccines do not contain live viruses and thus pose minimal risk of infection. However, the immune response may be suboptimal. Studies show that transplant recipients, for example, often produce lower antibody levels after COVID-19 vaccination compared to immunocompetent individuals. This underscores the importance of additional precautions, such as masking, social distancing, and close monitoring for symptoms, even after vaccination.
Practical tips for immunocompromised individuals include maintaining open communication with healthcare providers to stay updated on vaccine recommendations. Keeping a vaccination record is essential, especially for those who require multiple doses or frequent boosters. Additionally, caregivers and close contacts should ensure they are up to date on their own vaccinations to create a protective "cocoon" around the immunocompromised individual. For example, household members of someone with leukemia should receive the Tdap (tetanus, diphtheria, pertussis) vaccine to reduce the risk of transmitting pertussis, which can be life-threatening for the immunocompromised.
In conclusion, prioritizing immunocompromised individuals for vaccination is a critical public health strategy. While vaccination protocols must be carefully tailored to their unique needs, the benefits of protection far outweigh the risks. By understanding the specific challenges and adjustments required, healthcare providers and patients can work together to maximize immunity and minimize vulnerability. This targeted approach not only safeguards immunocompromised individuals but also contributes to broader community health by reducing the spread of infectious diseases.
Does US Bank Fund Dakota Access Pipeline? Uncovering Financial Ties
You may want to see also
Explore related products






![]()
Geographic Considerations: High-risk areas or outbreak zones may influence eligibility criteria
In regions grappling with active disease outbreaks, vaccine eligibility often prioritizes individuals residing in or frequently visiting high-risk zones. For instance, during a measles outbreak in a densely populated urban area, public health officials might expand eligibility to include all residents aged 6 months and older, regardless of prior vaccination status. This strategy, known as a "ring vaccination" approach, aims to create a buffer of immunity around the outbreak epicenter. In such scenarios, geographic location becomes a critical determinant of eligibility, superseding other factors like age or underlying health conditions.
Consider the 2019 Ebola outbreak in the Democratic Republic of Congo, where the rVSV-ZEBOV vaccine was administered in a targeted manner. Eligibility was initially restricted to frontline healthcare workers and individuals with confirmed exposure in high-incidence areas. As the outbreak intensified, eligibility expanded to include entire communities in affected districts, with a focus on individuals aged 1 year and older. This geographic targeting ensured that limited vaccine supplies were deployed where they could have the greatest impact, slowing transmission in high-risk zones.
When implementing geographic-based eligibility criteria, public health officials must balance urgency with equity. For example, during the COVID-19 pandemic, some regions prioritized residents of long-term care facilities or densely populated neighborhoods with high transmission rates. However, this approach risked overlooking vulnerable populations in lower-risk areas. To mitigate this, officials often paired geographic criteria with other risk factors, such as age (e.g., individuals 65 and older) or occupation (e.g., essential workers). This hybrid approach ensured that vaccine distribution addressed both immediate outbreak containment and broader population protection.
Practical implementation of geographic eligibility requires clear communication and logistical planning. For instance, during a flu outbreak in a specific county, health departments might issue temporary eligibility guidelines for local residents, accompanied by mobile vaccination clinics in high-traffic areas. Clear messaging—such as "Residents of [County X] aged 12+ are now eligible for an additional flu vaccine dose"—helps prevent confusion and ensures high-risk zones receive prioritized access. Additionally, leveraging geotagged data and digital tools can streamline identification of eligible individuals, ensuring rapid response in outbreak zones.
Ultimately, geographic considerations in vaccine eligibility serve as a dynamic tool for outbreak management, adapting to real-time disease spread patterns. By focusing resources on high-risk areas, public health systems can disrupt transmission chains more effectively. However, this approach must be continually reassessed as outbreak zones shift, ensuring eligibility criteria remain responsive to evolving epidemiological data. For policymakers, the key takeaway is clear: geographic targeting is not a one-size-fits-all solution but a strategic lever that, when combined with other eligibility factors, can maximize the impact of limited vaccine supplies.
Covishield: Vaccine or Immunity Booster? Understanding Its Role in COVID-19 Protection
You may want to see also
Frequently asked questions
Underlying conditions such as heart disease, diabetes, chronic lung disease, cancer, obesity, and immunocompromised states often make individuals eligible for priority vaccination or additional doses.
Yes, autoimmune disorders like rheumatoid arthritis, lupus, or inflammatory bowel disease often qualify, especially if the individual is on immunosuppressive medications.
Yes, moderate to severe asthma is typically considered an underlying condition, making individuals eligible for priority vaccination or booster shots.
Yes, pregnancy is considered a high-risk condition, and pregnant individuals are often prioritized for vaccines, including COVID-19 and flu vaccines.
Mental health conditions alone are not typically included, but if they are accompanied by physical health issues or immunocompromising factors, they may contribute to eligibility.































