Vaccines are biological preparations that provide active, acquired immunity to particular diseases by stimulating the immune system to recognize and combat pathogens. Vaccine I typically refers to the initial or primary dose administered to introduce the immune system to a specific antigen, laying the foundation for immune memory. Vaccine II represents the booster dose, given after the initial dose, to reinforce the immune response and enhance long-term protection. Vaccine III may denote a third dose, often used in certain vaccination schedules to ensure robust and sustained immunity, particularly against evolving pathogens or in immunocompromised individuals. Together, these doses form a comprehensive vaccination strategy to prevent disease and promote public health.
Explore related products




$11.93 $21.99


What You'll Learn
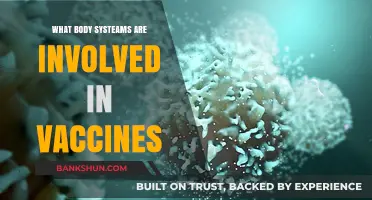
- Vaccine Types: Explains different vaccine categories like mRNA, viral vector, and protein subunit vaccines
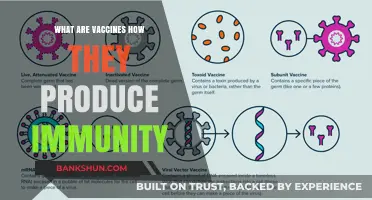
- Immunity Basics: How vaccines train the immune system to recognize and fight pathogens effectively
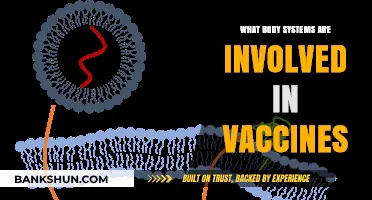
- Vaccine Development: Steps from research to approval, including trials and regulatory processes
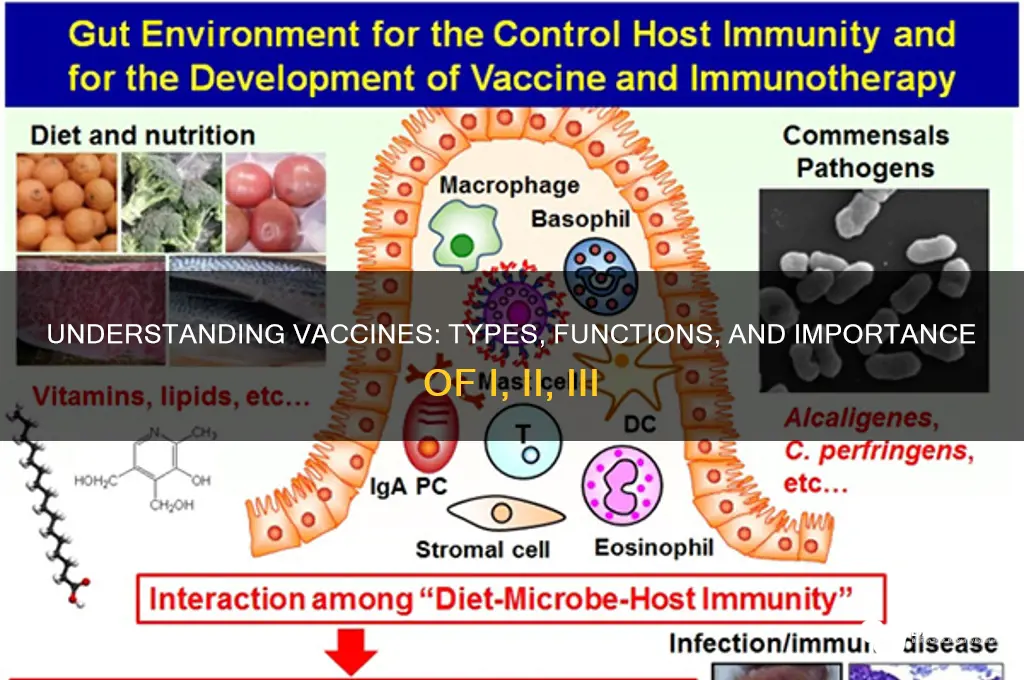
- Vaccine Efficacy: Measures of how well vaccines prevent disease and reduce severity
- Vaccine Safety: Monitoring side effects, myths, and ensuring public trust in vaccination programs
![]()
Vaccine Types: Explains different vaccine categories like mRNA, viral vector, and protein subunit vaccines
Vaccines are not one-size-fits-all. Modern advancements have led to the development of distinct categories, each with unique mechanisms and applications. Among these, mRNA, viral vector, and protein subunit vaccines stand out for their innovative approaches to triggering immune responses. Understanding these types is crucial for appreciating how they combat diseases like COVID-19, influenza, and others.
MRNA Vaccines: The Genetic Instructors
MRNA vaccines, such as Pfizer-BioNTech and Moderna’s COVID-19 shots, operate by delivering genetic material (mRNA) that instructs cells to produce a harmless piece of the virus’s spike protein. The immune system recognizes this protein as foreign, prompting the production of antibodies and memory cells. Unlike traditional vaccines, mRNA vaccines do not use live viruses, reducing the risk of infection. Dosage typically involves two shots, 3–4 weeks apart, with booster recommendations varying by age and health status. For instance, individuals over 65 or immunocompromised may require additional doses for sustained protection. A key advantage is their rapid development potential, as seen during the pandemic, though storage at ultra-cold temperatures remains a logistical challenge.
Viral Vector Vaccines: The Trojan Horses
Viral vector vaccines, exemplified by Johnson & Johnson’s COVID-19 vaccine and AstraZeneca’s Vaxzevria, employ a modified, harmless virus (the vector) to deliver genetic instructions for producing viral proteins. Once inside cells, the vector releases its payload, triggering an immune response. These vaccines are versatile and can target multiple diseases, including Ebola and HIV. A single dose is often sufficient, making them logistically simpler than multi-dose regimens. However, rare side effects like thrombosis with thrombocytopenia syndrome (TTS) have been reported, particularly in younger adults. Despite this, their ease of storage (refrigerated temperatures) and proven efficacy in low-resource settings make them valuable tools in global health campaigns.
Protein Subunit Vaccines: The Precision Tools
Protein subunit vaccines, such as Novavax’s COVID-19 vaccine, contain purified pieces of the virus, typically proteins that mimic the pathogen’s structure. These fragments are incapable of causing disease but effectively stimulate the immune system. Adjuvants, like aluminum salts, are often added to enhance the immune response. This type is ideal for individuals with weakened immune systems or those who cannot receive live vaccines. Dosage usually involves two shots, 3–4 weeks apart, with minimal side effects such as soreness at the injection site. Their stability at standard refrigeration temperatures and long shelf life make them accessible for widespread distribution. Notably, protein subunit vaccines have been used for decades in vaccines like hepatitis B and HPV, underscoring their safety and reliability.
Comparative Takeaway: Choosing the Right Tool
Each vaccine type offers distinct advantages depending on the context. mRNA vaccines excel in rapid development and high efficacy but require stringent storage. Viral vector vaccines provide single-dose convenience and stability but carry rare risks. Protein subunit vaccines combine safety and accessibility, making them suitable for diverse populations. The choice depends on factors like disease prevalence, infrastructure, and individual health needs. For instance, mRNA vaccines are prioritized in regions with robust healthcare systems, while viral vector and protein subunit vaccines are favored in resource-limited settings. Understanding these differences empowers individuals and policymakers to make informed decisions, ensuring vaccines reach those who need them most.
Activate HDFC International Banking: A Step-by-Step Guide for Global Transactions
You may want to see also
Explore related products






![]()
Immunity Basics: How vaccines train the immune system to recognize and fight pathogens effectively
Vaccines are not just shots; they are sophisticated tools that teach the immune system to recognize and combat pathogens before they cause harm. At their core, vaccines introduce a harmless piece of a pathogen—such as a protein or a weakened virus—to trigger an immune response. This process mimics a natural infection but without the risk of severe illness. For instance, the measles vaccine contains a live but attenuated (weakened) virus that prompts the immune system to produce antibodies and memory cells, preparing it for future encounters with the actual virus. This foundational principle applies to all vaccines, whether they are classified as Type I (live-attenuated), Type II (inactivated), or Type III (subunit, recombinant, or conjugate).
Consider the immune system as a security team that learns on the job. When a vaccine is administered, it acts like a training drill, exposing the team to a safe version of the threat. For example, the mRNA vaccines (Type III) for COVID-19 provide genetic instructions for cells to produce a harmless spike protein found on the virus. The immune system identifies this protein as foreign, generates antibodies, and creates memory cells. If the real virus invades later, the immune system is primed to respond swiftly, often preventing infection or reducing its severity. This training is particularly critical for vulnerable populations, such as infants and the elderly, who may not mount an effective response without vaccination.
The effectiveness of vaccines hinges on their ability to mimic pathogens closely enough to provoke a robust immune response but safely. Live-attenuated vaccines (Type I), like the MMR (measles, mumps, rubella) vaccine, offer long-lasting immunity with just one or two doses because they replicate mildly in the body, closely resembling a natural infection. In contrast, inactivated vaccines (Type II), such as the injectable flu shot, require multiple doses and sometimes adjuvants to enhance the immune response since they cannot replicate. Subunit vaccines (Type III) are highly targeted, using only specific pathogen components, making them ideal for individuals with weakened immune systems. For example, the hepatitis B vaccine, a Type III recombinant vaccine, is administered in a series of three doses over six months to ensure full immunity.
Practical considerations are key to maximizing vaccine efficacy. Timing and dosage matter—infants receive the DTaP vaccine (a Type III conjugate vaccine) in five doses starting at 2 months to build immunity against diphtheria, tetanus, and pertussis. Booster shots, like the Tdap vaccine for adolescents and adults, reinforce this protection. Storage and handling are equally critical; mRNA vaccines must be stored at ultra-cold temperatures to maintain stability, while traditional vaccines often require refrigeration. Adhering to these guidelines ensures the immune system receives the intended training, minimizing the risk of outbreaks and complications from vaccine-preventable diseases.
Ultimately, vaccines are a testament to the immune system’s adaptability and the power of preventive medicine. By understanding how different vaccine types train the body—whether through live pathogens, inactivated versions, or specific components—individuals can make informed decisions about their health. Vaccines not only protect the vaccinated but also contribute to herd immunity, shielding those who cannot be immunized due to medical reasons. This dual benefit underscores the importance of vaccination as a cornerstone of public health, turning the immune system into a well-prepared defense force against pathogens.
Exploring Benidorm: Is There a Barclays Bank in the City?
You may want to see also
Explore related products

$18.59 $19.95





![]()
Vaccine Development: Steps from research to approval, including trials and regulatory processes
Vaccine development is a rigorous, multi-stage process that ensures safety, efficacy, and quality before a vaccine reaches the public. It begins with exploratory research, where scientists identify antigens—substances that trigger an immune response—and potential vaccine platforms. For instance, mRNA technology, used in COVID-19 vaccines like Pfizer-BioNTech and Moderna, was developed over decades before its rapid deployment during the pandemic. This phase involves laboratory studies and animal testing to assess initial safety and immunogenicity, often taking 2–5 years.
Once a candidate is identified, it advances to preclinical testing, where researchers refine the vaccine’s formulation and dosage. For example, the HPV vaccine Gardasil underwent extensive preclinical trials to determine its optimal dose (0.5 mL) and administration schedule (three doses over 6 months). This stage also includes toxicity studies in animals to ensure the vaccine does not cause harm. If successful, the vaccine proceeds to clinical trials, a three-phase process involving humans. Phase I trials focus on safety and dosage in small groups (20–100 volunteers), while Phase II expands to hundreds to evaluate efficacy and side effects. Phase III trials involve thousands to tens of thousands of participants, often across multiple countries, to confirm effectiveness and monitor rare adverse events. For instance, the Pfizer COVID-19 vaccine’s Phase III trial included 44,000 participants, demonstrating 95% efficacy.
Following clinical trials, vaccine developers submit their data to regulatory authorities like the FDA or EMA for approval. These agencies scrutinize the evidence, inspecting manufacturing facilities to ensure compliance with Good Manufacturing Practices (GMP). Emergency Use Authorization (EUA), as granted for COVID-19 vaccines, allows faster approval during public health crises but still requires robust safety and efficacy data. Full approval follows after additional long-term data is collected. For example, the Pfizer vaccine received full FDA approval in August 2021 after months of real-world use in millions of individuals.
Even after approval, post-market surveillance continues through systems like the Vaccine Adverse Event Reporting System (VAERS) in the U.S. This phase monitors rare side effects that may not have appeared in clinical trials. For instance, the rare link between the Johnson & Johnson COVID-19 vaccine and thrombosis with thrombocytopenia syndrome (TTS) was identified post-approval, leading to updated guidelines. Additionally, vaccines often require phase IV trials to study long-term effects and efficacy in specific populations, such as pregnant women or immunocompromised individuals.
In summary, vaccine development is a meticulous journey from lab to market, balancing speed with safety. Each step—from exploratory research to post-market surveillance—is critical to ensuring vaccines protect public health effectively. Understanding this process fosters trust and highlights the scientific rigor behind every dose administered.
Concealed Carry in Banks: Legal or Illegal? Understanding the Laws
You may want to see also
Explore related products






![]()
Vaccine Efficacy: Measures of how well vaccines prevent disease and reduce severity
Vaccine efficacy is a critical metric that quantifies how effectively a vaccine prevents disease and reduces its severity in a vaccinated population compared to an unvaccinated one. It is typically expressed as a percentage, calculated from clinical trials by comparing the incidence of disease in vaccinated versus control groups. For example, the Pfizer-BioNTech COVID-19 vaccine demonstrated 95% efficacy in preventing symptomatic infection in its Phase 3 trial, meaning vaccinated individuals were 95% less likely to develop the disease than those who received a placebo. This measure is essential for public health decision-making, as it directly informs vaccine approval, distribution, and policy recommendations.
While vaccine efficacy is a powerful indicator, it is not the only measure of a vaccine’s impact. Vaccine effectiveness (VE) assesses real-world performance, accounting for factors like varying dosage adherence, population immunity, and virus mutations. For instance, the flu vaccine’s VE often ranges between 40–60%, lower than its clinical efficacy due to annual strain mismatches and waning immunity. Another critical measure is reduction in disease severity, which evaluates how well a vaccine prevents hospitalization, severe illness, or death, even if it doesn’t entirely block infection. The COVID-19 vaccines, for example, have consistently shown high efficacy in preventing severe outcomes, with studies indicating over 90% protection against hospitalization across age groups, including the elderly.
Understanding vaccine efficacy requires considering its limitations and nuances. No vaccine is 100% effective, and efficacy can vary by demographic factors such as age, underlying health conditions, and immune status. For instance, the shingles vaccine Shingrix has an efficacy of over 90% in adults aged 50–69 but drops to 70–80% in those over 70 due to age-related immune decline. Additionally, efficacy is disease-specific; a vaccine designed for one pathogen may not protect against related strains or variants. Practical tips for maximizing vaccine efficacy include adhering to recommended dosages (e.g., two doses of mRNA COVID-19 vaccines spaced 3–4 weeks apart) and staying updated with booster shots to maintain immunity.
Finally, vaccine efficacy plays a pivotal role in herd immunity, the indirect protection that occurs when a large portion of a population is immune to a disease. For highly contagious diseases like measles, which has a basic reproduction number (R0) of 12–18, a vaccine with 95% efficacy must achieve at least 93–95% population coverage to interrupt transmission. In contrast, diseases with lower transmissibility, such as polio (R0 of 5–7), require lower coverage rates. Public health strategies must therefore balance vaccine efficacy with accessibility and uptake to achieve herd immunity, particularly in vulnerable communities. By understanding and communicating these measures effectively, policymakers and healthcare providers can build trust and ensure vaccines are used to their fullest potential.
Activate Bank Feeds in QuickBooks: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Vaccine Safety: Monitoring side effects, myths, and ensuring public trust in vaccination programs
Vaccines are meticulously designed to prevent diseases, but their success hinges on public trust, which is fragile and often undermined by misinformation. Ensuring vaccine safety is a cornerstone of maintaining this trust, requiring robust systems to monitor side effects, debunk myths, and communicate transparently. For instance, the Vaccine Adverse Event Reporting System (VAERS) in the U.S. allows healthcare providers and individuals to report adverse reactions, enabling rapid investigation of potential safety concerns. Similarly, the Global Advisory Committee on Vaccine Safety (GACVS) provides independent, authoritative assessments of vaccine safety issues. These systems are not just bureaucratic tools; they are the backbone of public confidence, demonstrating that safety is continuously monitored and prioritized.
Monitoring side effects is both a science and an art. While clinical trials provide initial safety data, rare side effects may only emerge once vaccines are administered to millions. Take the case of the mRNA COVID-19 vaccines, where rare cases of myocarditis (heart inflammation) were detected post-authorization, primarily in adolescent males after the second dose. Health authorities responded by updating guidelines, recommending longer intervals between doses and advising close monitoring. This example underscores the importance of post-market surveillance and adaptive strategies. Parents and caregivers should be aware of common side effects, such as fever or soreness, and seek medical advice if symptoms persist or worsen. Practical tips include administering acetaminophen for discomfort and ensuring hydration, but always consult a healthcare provider before giving medications to children under 2 years old.
Myths about vaccines are pervasive and dangerous, often exploiting fears about safety. One persistent myth is that vaccines cause autism, a claim thoroughly debunked by numerous studies involving millions of children. Another is the belief that natural immunity is superior to vaccine-induced immunity, ignoring the risks of severe illness or death from preventable diseases. Combatting these myths requires clear, evidence-based communication. For example, explaining that vaccines contain only tiny amounts of antigens—far fewer than what the immune system encounters daily—can demystify their composition. Public health campaigns should leverage trusted figures, such as local doctors or community leaders, to deliver messages in culturally sensitive ways. Parents hesitant about vaccinating their children should be engaged with empathy, not judgment, and provided with reliable resources like the CDC’s vaccine information sheets.
Ensuring public trust in vaccination programs demands transparency and inclusivity. When safety concerns arise, swift acknowledgment and action are critical. For instance, the temporary pause of the Johnson & Johnson COVID-19 vaccine in 2021 to investigate rare blood clots demonstrated a commitment to safety, even at the cost of short-term disruption. This transparency builds credibility, showing that systems are in place to protect the public. Additionally, involving communities in vaccine development and rollout can address historical mistrust, particularly in marginalized groups. For example, the FDA’s Patient Representative Program includes diverse voices in regulatory decisions, ensuring vaccines meet the needs of all populations. Practical steps for healthcare providers include actively listening to patient concerns, addressing questions directly, and avoiding dismissive language. By fostering trust through action and communication, vaccination programs can remain a cornerstone of public health.
Resilient Recovery: How Banks Rebounded Post-Financial Crisis
You may want to see also
Frequently asked questions
Vaccines are biological preparations that provide active, acquired immunity to particular diseases. They typically contain a weakened or inactivated form of the disease-causing organism or its toxins, which stimulate the body's immune system to recognize and fight the pathogen without causing the disease.
Vaccines can be categorized into three main types:
I. Live-attenuated vaccines - These contain a weakened (attenuated) form of the live virus or bacteria, which still replicates in the body but does not cause disease in healthy individuals (e.g., measles, mumps, rubella (MMR) vaccine).
II. Inactivated vaccines - These use a killed version of the germ, which cannot replicate but still triggers an immune response (e.g., polio (IPV) and hepatitis A vaccines).
III. Subunit, recombinant, polysaccharide, and conjugate vaccines - These use specific pieces of the pathogen, such as proteins or sugars, rather than the entire organism (e.g., HPV, hepatitis B, and pneumococcal conjugate vaccines).
A: