mRNA vaccines, such as those developed by Pfizer-BioNTech and Moderna for COVID-19, work by delivering genetic material (messenger RNA) into cells to instruct them to produce a harmless piece of the virus’s spike protein. This triggers an immune response, preparing the body to fight the actual virus. The primary cells targeted by mRNA vaccines are dendritic cells, a type of immune cell found in tissues throughout the body, particularly near injection sites like the deltoid muscle. Dendritic cells are highly efficient at taking up the mRNA, processing it, and presenting the spike protein to other immune cells, such as T cells and B cells, which then mount a robust immune response. While dendritic cells are the main targets, other cells, such as muscle cells or endothelial cells, may also take up the mRNA, though their role in the immune response is less significant. This targeted approach ensures efficient and effective immunization with minimal off-target effects.
| Characteristics | Values |
|---|---|
| Cell Type | Primarily targets antigen-presenting cells (APCs), including dendritic cells (DCs), macrophages, and B cells |
| Location | Delivered to muscle cells at the injection site, but primarily taken up by APCs in lymph nodes and other tissues |
| Uptake Mechanism | Endocytosis, facilitated by the lipid nanoparticle (LNP) delivery system |
| Intracellular Processing | mRNA is released into the cytoplasm, where it is translated into the encoded antigen (e.g., SARS-CoV-2 spike protein) |
| Antigen Presentation | APCs process and present antigen peptides on MHC class I and II molecules to activate CD8+ and CD4+ T cells, respectively |
| Immune Response | Induces both humoral (neutralizing antibodies by B cells) and cellular (cytotoxic T cells) immune responses |
| Tissue Specificity | Minimal targeting of non-immune cells; LNPs are designed to avoid off-target effects in organs like the liver or spleen |
| Duration of Expression | Transient; mRNA is degraded within days, limiting long-term antigen production |
| Safety Feature | Does not enter the cell nucleus, preventing integration into the host genome |
| Examples of Targeted Cells | Dendritic cells, macrophages, follicular B cells in germinal centers, and muscle cells (transiently at injection site) |
Explore related products


$454.47 $549.99




What You'll Learn
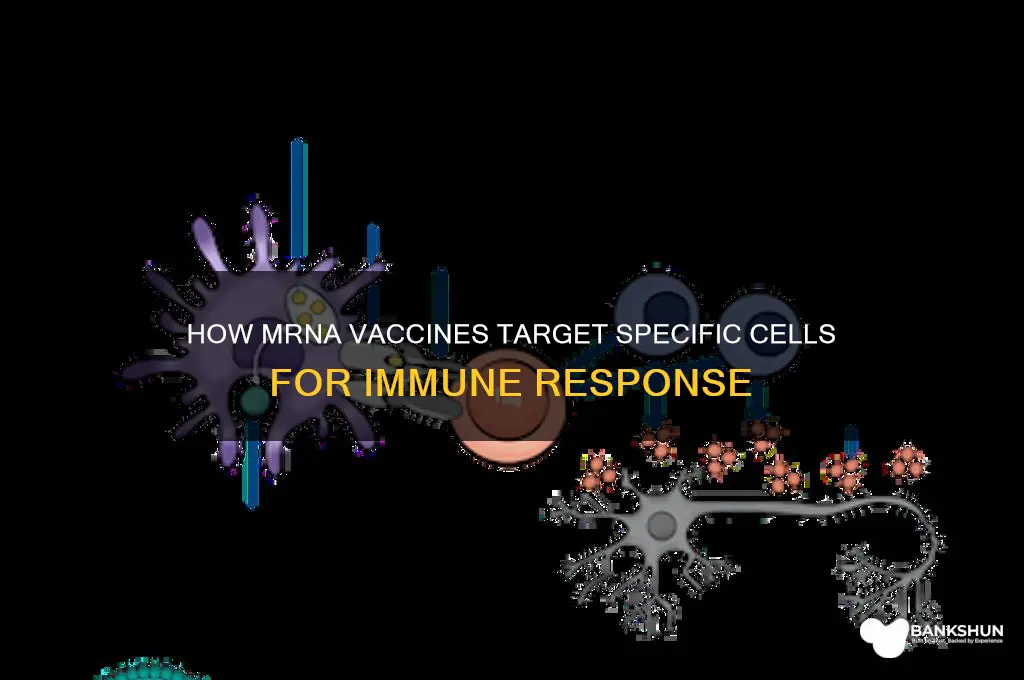
- Immune cells: mRNA vaccines primarily target dendritic cells and macrophages to initiate immune responses
- Antigen presentation: mRNA enters cells, producing proteins that activate T cells and B cells
- Muscle cells: Injection sites often involve muscle cells, which can take up mRNA temporarily
- Lymph node migration: Antigen-presenting cells migrate to lymph nodes to activate adaptive immunity
- Non-replicating nature: mRNA does not target cell nuclei, ensuring no genetic material integration
![]()
Immune cells: mRNA vaccines primarily target dendritic cells and macrophages to initiate immune responses
MRNA vaccines, such as those developed by Pfizer-BioNTech and Moderna for COVID-19, operate by delivering genetic material into cells to produce a harmless piece of the virus, triggering an immune response. Among the myriad of cells in the body, dendritic cells and macrophages are the primary targets of these vaccines due to their pivotal role in antigen presentation and immune activation. These cells act as sentinels, capturing the mRNA, translating it into viral proteins, and presenting these antigens to T cells, thereby initiating a robust immune response. Understanding this mechanism is crucial for appreciating how mRNA vaccines harness the body’s natural defenses.
Consider the process as a relay race: dendritic cells and macrophages are the first runners, receiving the mRNA "baton" via lipid nanoparticles. Once inside these cells, the mRNA is translated into viral proteins, which are then fragmented and displayed on the cell surface using MHC molecules. This presentation signals T cells and B cells to spring into action, with T cells coordinating the immune response and B cells producing antibodies. The efficiency of this process is why mRNA vaccines often require lower doses (e.g., 30 µg for Pfizer and 100 µg for Moderna) compared to traditional vaccines, as they directly engage these potent immune cells.
Practical implications of this targeting are significant, especially for vulnerable populations like the elderly or immunocompromised. Since dendritic cells and macrophages are present in various tissues, including the skin, lymph nodes, and lungs, mRNA vaccines can be administered via intramuscular injection, ensuring widespread immune activation. However, this also underscores the importance of proper injection technique to maximize uptake by these cells. For instance, healthcare providers should adhere to guidelines such as injecting into the deltoid muscle for adults and the vastus lateralis muscle for infants, ensuring optimal delivery to the target cells.
A comparative analysis highlights the advantage of mRNA vaccines over traditional platforms. Unlike inactivated or live-attenuated vaccines, which rely on direct antigen injection, mRNA vaccines co-opt dendritic cells and macrophages to produce antigens internally. This mimics natural infection more closely, leading to stronger and more durable immunity. For example, studies show that mRNA vaccines elicit higher neutralizing antibody titers and robust T cell responses compared to adenovirus-vectored vaccines, a testament to the effectiveness of targeting these immune cells.
In conclusion, the success of mRNA vaccines hinges on their ability to precisely target dendritic cells and macrophages, leveraging their role as immune orchestrators. This strategy not only ensures potent and rapid immune responses but also opens avenues for future vaccine development against other diseases. For individuals, understanding this mechanism reinforces the importance of vaccination, while for healthcare providers, it emphasizes the need for precise administration techniques to maximize vaccine efficacy. By focusing on these cells, mRNA vaccines represent a paradigm shift in immunology, blending innovation with the body’s innate defense mechanisms.
Easy Steps to Add a Biller in Corporation Bank Online
You may want to see also
Explore related products






![]()
Antigen presentation: mRNA enters cells, producing proteins that activate T cells and B cells
MRNA vaccines, such as those developed by Pfizer-BioNTech and Moderna, operate by introducing a genetic blueprint into cells, instructing them to produce a specific protein—typically the spike protein of a virus like SARS-CoV-2. This process hinges on antigen presentation, a critical step in the immune response. Once the mRNA enters cells, it is translated into the target protein, which is then displayed on the cell surface via MHC (Major Histocompatibility Complex) molecules. This presentation acts as a red flag, signaling to immune cells that something foreign is present and requires action.
The cells primarily targeted by mRNA vaccines are antigen-presenting cells (APCs), including dendritic cells, macrophages, and B cells. Dendritic cells, in particular, play a pivotal role due to their efficiency in processing and presenting antigens. When an mRNA vaccine is administered, typically via intramuscular injection, muscle cells and local APCs take up the mRNA. However, it’s the dendritic cells that migrate to lymph nodes, where they present the antigen to T cells and B cells, initiating a robust immune response. This process is dose-dependent; for instance, the Pfizer-BioNTech vaccine delivers 30 micrograms of mRNA per dose, optimized to ensure sufficient protein production without overwhelming the system.
The activation of T cells and B cells is a two-pronged defense mechanism. Helper T cells (CD4+) recognize the antigen presented by APCs and release cytokines, which act as chemical messengers to amplify the immune response. Simultaneously, cytotoxic T cells (CD8+) are primed to identify and destroy cells displaying the foreign protein. B cells, on the other hand, differentiate into plasma cells that produce antibodies specific to the antigen. This dual activation ensures both immediate and long-term immunity. For practical application, individuals aged 12 and older typically receive two doses, spaced 3–4 weeks apart, to maximize this immune orchestration.
A critical takeaway is that mRNA vaccines do not target all cells indiscriminately. Instead, they leverage the body’s natural antigen presentation pathways, focusing on APCs to trigger a precise and effective immune response. This specificity minimizes off-target effects, making mRNA vaccines both safe and highly efficient. For optimal results, recipients should adhere to the recommended dosing schedule and avoid immunosuppressants, which could hinder the activation of T and B cells. Understanding this process underscores the elegance of mRNA technology in harnessing the body’s own machinery to combat pathogens.
How to Withdraw Funds from CoinEx to Your Bank Account
You may want to see also
Explore related products






![]()
Muscle cells: Injection sites often involve muscle cells, which can take up mRNA temporarily
Muscle cells play a pivotal role in the delivery and temporary uptake of mRNA vaccines, particularly when administered via intramuscular injection. This method, commonly used for vaccines like Pfizer-BioNTech and Moderna’s COVID-19 shots, targets the deltoid muscle in the upper arm for adults or the vastus lateralis muscle in the thigh for infants and young children. Upon injection, the mRNA molecules encased in lipid nanoparticles are rapidly taken up by muscle cells, where they remain transiently. This uptake is not permanent; the mRNA degrades within days, ensuring it does not alter the cell’s DNA. The process leverages the muscle cell’s machinery to produce spike proteins, triggering an immune response without long-term cellular changes.
The choice of muscle cells as injection sites is strategic. Muscle tissue is highly vascularized, meaning it has a rich blood supply that facilitates rapid distribution of the vaccine components to lymph nodes and other immune organs. Additionally, muscle cells are efficient at endocytosis, the process by which they engulf and internalize the lipid nanoparticles containing mRNA. This efficiency ensures that even a small dose—typically 30 micrograms for Pfizer or 100 micrograms for Moderna—can elicit a robust immune response. However, the temporary nature of mRNA uptake in muscle cells is a critical safety feature, as it minimizes the risk of off-target effects or prolonged protein production.
While muscle cells are the primary target, it’s important to note that not all injected mRNA reaches them. Some may be taken up by other cell types, such as dendritic cells or macrophages, which also contribute to immune activation. Nonetheless, muscle cells remain central to the vaccine’s mechanism due to their accessibility and capacity for protein synthesis. For optimal results, healthcare providers are instructed to administer the injection deep into the muscle tissue, avoiding subcutaneous delivery, which could reduce efficacy. Patients are advised to relax the arm during injection to minimize discomfort and ensure proper needle placement.
Practical considerations for mRNA vaccines involving muscle cells include dosage adjustments for specific age groups. For instance, children aged 6 months to 5 years receive a lower dose (e.g., 10 micrograms for Pfizer) to account for their smaller muscle mass and immune system differences. Post-injection, mild muscle pain or swelling at the site is common, reflecting the localized immune activity. Applying a cold compress and keeping the arm active can alleviate discomfort. Understanding the role of muscle cells in this process underscores the precision and safety of mRNA vaccine design, making it a cornerstone of modern immunization strategies.
Karur Vysya Bank: Understanding Its Government or Private Ownership Status
You may want to see also
Explore related products





![]()
Lymph node migration: Antigen-presenting cells migrate to lymph nodes to activate adaptive immunity
The journey of an mRNA vaccine begins with a targeted delivery to specific cells, but its true power unfolds in the lymph nodes. Here, a critical process known as lymph node migration takes center stage. Antigen-presenting cells (APCs), primarily dendritic cells, act as the vaccine's messengers, migrating from the injection site to the lymph nodes, where they activate the adaptive immune system. This migration is a pivotal step, transforming a local immune response into a systemic defense mechanism.
The Migration Process: A Delicate Dance
Imagine a relay race where the baton is crucial information about the pathogen. APCs, upon encountering the mRNA vaccine, internalize the genetic material and begin their journey to the lymph nodes. This migration is not random; it's a highly regulated process guided by chemokines, signaling molecules that act as homing beacons. The lymphatic system, a network of vessels and nodes, facilitates this movement, ensuring APCs reach their destination efficiently. Typically, this migration occurs within 24-48 hours after vaccination, with the speed and efficiency influenced by factors like the vaccine's formulation and the individual's immune status.
Activating the Adaptive Immunity: A Strategic Meeting
Upon arrival at the lymph nodes, APCs present the processed antigen to naïve T cells, initiating a cascade of events. This interaction is akin to a strategic meeting where the immune system's generals (T cells) are briefed on the enemy (the pathogen). The APCs, now mature and activated, display the antigen on their surface, bound to major histocompatibility complex (MHC) molecules. This presentation triggers T cell differentiation into effector cells, including helper T cells and cytotoxic T cells, each with distinct roles in combating the pathogen. For instance, helper T cells secrete cytokines, signaling molecules that orchestrate the immune response, while cytotoxic T cells directly target and eliminate infected cells.
Practical Implications and Optimization
Understanding lymph node migration has practical implications for vaccine design and administration. Researchers are exploring ways to enhance this process, such as incorporating adjuvants that improve APC activation and migration. For example, the addition of toll-like receptor (TLR) agonists can boost APC maturation, leading to a more robust immune response. Moreover, the route of administration matters; intramuscular injections, commonly used for mRNA vaccines, are optimized to target muscle-resident APCs, which then migrate to the draining lymph nodes. This knowledge informs dosage strategies, with typical mRNA vaccine doses ranging from 30 to 100 micrograms, balanced to ensure sufficient APC activation without excessive inflammation.
A Comparative Perspective: Natural vs. Vaccine-Induced Immunity
Comparing lymph node migration in natural infection versus vaccination highlights the elegance of mRNA technology. In natural infections, APCs capture pathogens directly, leading to a more diverse antigen presentation. Vaccines, however, deliver a carefully selected antigen, focusing the immune response. This targeted approach reduces the risk of overwhelming the immune system while still providing robust protection. For instance, the Pfizer-BioNTech and Moderna mRNA vaccines encode for the SARS-CoV-2 spike protein, ensuring that APCs present this critical antigen to T cells, thereby generating a highly specific immune memory. This precision is particularly beneficial for vulnerable populations, such as the elderly or immunocompromised, where a controlled immune response is essential.
In essence, lymph node migration is the bridge between local vaccine administration and systemic immunity. By understanding and optimizing this process, scientists can refine mRNA vaccines, ensuring they provide effective protection across diverse age groups and health statuses. Practical tips, such as maintaining a healthy lymphatic system through regular exercise and hydration, can further support this critical immune function, making the most of the vaccine's potential.
Is Chickenpox Vaccine Mandatory in Ontario? What Parents Need to Know
You may want to see also
Explore related products





![]()
Non-replicating nature: mRNA does not target cell nuclei, ensuring no genetic material integration
One of the most critical safety features of mRNA vaccines lies in their non-replicating nature. Unlike traditional vaccines that use weakened or inactivated viruses, mRNA vaccines deliver a temporary set of instructions to cells, specifically immune cells like dendritic cells and macrophages. These cells act as sentinels, processing the mRNA and presenting its encoded antigen to T cells and B cells, which then mount a targeted immune response. Crucially, mRNA does not enter the cell nucleus, the cellular compartment housing DNA. This design ensures that the vaccine’s genetic material never integrates into the host’s genome, eliminating the risk of altering human DNA.
Consider the process in practical terms: when an mRNA vaccine, such as Pfizer-BioNTech’s Comirnaty (dosage: 30 µg for ages 12 and up, 10 µg for children 5–11), is administered intramuscularly, the mRNA molecules are encased in lipid nanoparticles to protect them from degradation. Once inside the cell cytoplasm, ribosomes translate the mRNA into the viral spike protein. This protein is then degraded after triggering an immune response, and the mRNA itself breaks down within days, leaving no trace in the cell. This transient presence underscores the vaccine’s safety profile, particularly for those concerned about long-term effects.
Comparatively, DNA-based vaccines or viral vector vaccines, such as Johnson & Johnson’s Janssen vaccine, introduce genetic material that must enter the nucleus to function. While these platforms are also designed to prevent genomic integration, mRNA vaccines offer a more straightforward mechanism by bypassing the nucleus entirely. This distinction is particularly reassuring for pregnant individuals or those planning to conceive, as it eliminates theoretical risks of genetic interference with fetal development.
For healthcare providers and educators, emphasizing this non-replicating nature can address vaccine hesitancy. Practical tips include explaining that mRNA’s instability outside the cell ensures it cannot persist or replicate, unlike live-attenuated vaccines. Additionally, highlighting real-world data—such as the billions of doses administered globally with no evidence of DNA integration—can reinforce trust in the technology. In summary, the non-replicating, nucleus-avoiding design of mRNA vaccines is a cornerstone of their safety, offering robust protection without compromising genetic integrity.
Capital One Cafés: Banking and Coffee
You may want to see also
Frequently asked questions
mRNA vaccines primarily target dendritic cells and other antigen-presenting cells (APCs) in the body. These cells take up the mRNA, translate it into the viral protein (e.g., the spike protein of SARS-CoV-2), and then present it to the immune system to trigger an immune response.
No, mRNA vaccines do not enter all cells in the body. They are typically administered intramuscularly, where they are taken up by local cells, primarily dendritic cells and muscle cells. However, their primary action occurs in antigen-presenting cells to stimulate an immune response.
No, mRNA vaccines do not target reproductive cells (sperm or egg cells) and cannot alter DNA. The mRNA in the vaccine remains in the cytoplasm of cells and is degraded after the protein is produced. It does not enter the nucleus, where DNA is located, and does not integrate into the genome.