All vaccines, regardless of their specific target or formulation, share a common purpose: to stimulate the immune system to recognize and combat pathogens without causing the disease itself. At their core, vaccines contain antigens—components derived from or resembling the disease-causing agent, such as weakened or inactivated viruses, bacteria, or specific proteins. These antigens trigger an immune response, prompting the body to produce antibodies and memory cells that provide future protection against the actual pathogen. Additionally, vaccines often include adjuvants to enhance the immune response and stabilizers to ensure their effectiveness during storage. This shared mechanism of action, combined with rigorous safety and efficacy testing, unites all vaccines in their goal of preventing infectious diseases and promoting public health.
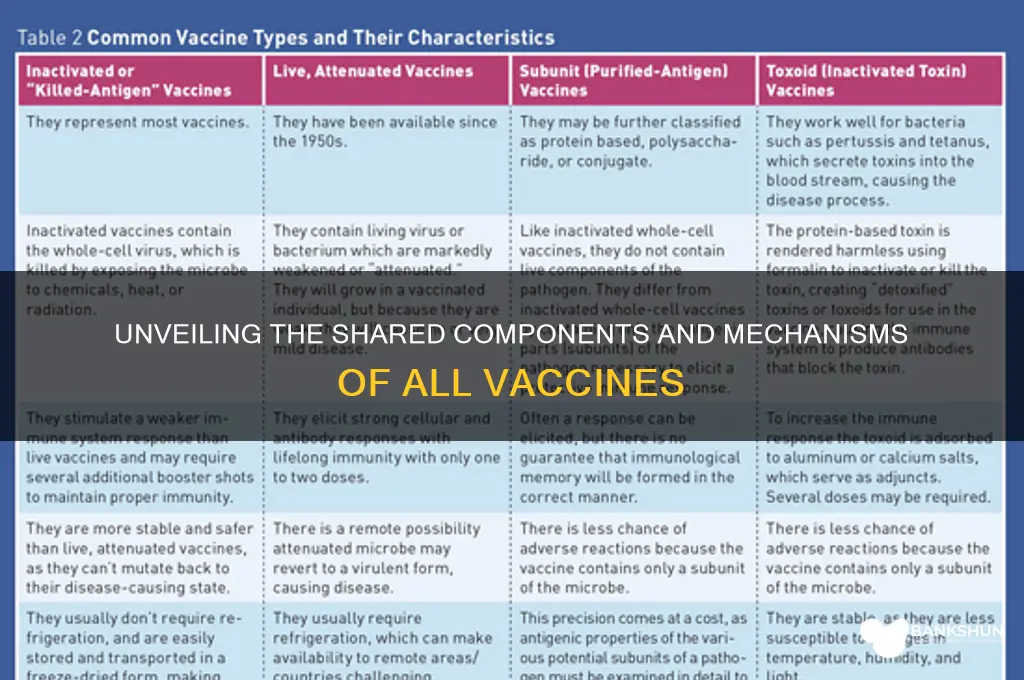
| Characteristics | Values |
|---|---|
| Purpose | Prevent or control diseases by inducing immunity |
| Active Ingredient | Antigen (weakened/killed pathogen, toxin, or component) |
| Adjuvants | Enhance immune response (e.g., aluminum salts, AS03) |
| Stabilizers | Maintain vaccine potency (e.g., sugars, amino acids) |
| Preservatives | Prevent contamination (e.g., thiomersal, phenol) |
| Administration Route | Intramuscular, subcutaneous, oral, or nasal |
| Dose Schedule | Requires one or more doses for full immunity |
| Immune Response | Stimulates production of antibodies and memory cells |
| Safety Testing | Rigorously tested in clinical trials (Phase I-III) |
| Regulatory Approval | Must be approved by health authorities (e.g., FDA, EMA) |
| Storage Requirements | Specific temperature and handling conditions (e.g., refrigeration) |
| Side Effects | Mild and temporary (e.g., soreness, fever, fatigue) |
| Efficacy | Reduces disease incidence and severity |
| Herd Immunity | Contributes to community protection when widely used |
| Continuous Monitoring | Post-approval surveillance for safety and efficacy |
Explore related products






What You'll Learn
- Active Ingredient: All vaccines contain antigens to trigger immune response against specific pathogens
- Adjuvants: Many include adjuvants to enhance immune system activation and vaccine effectiveness
- Preservatives: Some vaccines use preservatives to prevent contamination during storage and use
- Stabilizers: Stabilizers are added to maintain vaccine potency and stability over time
- Delivery Method: Vaccines are administered via injection, orally, or nasally for immune system access
![]()
Active Ingredient: All vaccines contain antigens to trigger immune response against specific pathogens
Vaccines are designed with a singular, non-negotiable purpose: to teach the immune system to recognize and combat specific pathogens. At the heart of every vaccine lies its active ingredient—the antigen. Whether it’s a weakened virus in the MMR vaccine, a fragment of bacterial protein in the tetanus shot, or a stabilized spike protein in mRNA COVID-19 vaccines, antigens are the molecular key that unlocks immune memory. Without them, vaccines would be inert, unable to provoke the protective response they’re engineered to deliver.
Consider the precision required in antigen selection. For instance, the influenza vaccine contains hemagglutinin and neuraminidase proteins, meticulously chosen because they’re critical to the virus’s function and highly recognizable to immune cells. Similarly, the HPV vaccine uses virus-like particles (VLPs) assembled from the L1 protein, mimicking the virus’s shell without containing infectious material. This strategic choice ensures robust immunity without the risk of disease. Dosage matters too: the hepatitis B vaccine delivers 10–20 micrograms of surface antigen per dose, calibrated to elicit a strong response in infants as young as 6 weeks, while the shingles vaccine (Shingrix) uses a higher dose of glycoprotein E antigen to overcome age-related immune decline in adults over 50.
The antigen’s form dictates the vaccine’s mechanism. Live-attenuated vaccines, like the measles component of the MMR shot, use weakened but intact viruses to trigger a response akin to natural infection. In contrast, subunit vaccines, such as the pertussis component of the DTaP shot, isolate specific proteins (e.g., pertactin, filamentous hemagglutinin) to minimize side effects while maintaining efficacy. mRNA vaccines, a newer category, deliver genetic instructions for cells to produce the antigen locally, as seen in the Pfizer-BioNTech COVID-19 vaccine’s 30-microgram dose of nucleoside-modified mRNA encoding the spike protein. Each approach leverages antigens in a way tailored to the pathogen’s biology and the host’s immune needs.
Practical considerations abound when administering antigen-based vaccines. Storage conditions, for example, are critical: mRNA vaccines require ultra-cold temperatures (-70°C for Pfizer’s, -20°C for Moderna’s) to stabilize the fragile RNA molecules, while traditional vaccines like the flu shot are stable in standard refrigeration. Timing matters too: the HPV vaccine’s three-dose series (0, 2, 6 months) ensures durable immunity in adolescents aged 9–14, while a two-dose schedule is sufficient for those vaccinated before age 15. Adverse reactions, though rare, are more likely with certain antigen types—live vaccines may cause mild fever, while adjuvanted vaccines (e.g., Shingrix’s AS01B adjuvant) often lead to localized pain and fatigue, signaling a vigorous immune response.
Ultimately, antigens are the linchpin of vaccine design, bridging the gap between pathogen and protection. Their selection, formulation, and delivery are governed by a delicate balance of immunology, chemistry, and clinical need. For the public, understanding this core component demystifies how vaccines work and underscores their safety and specificity. Whether you’re a parent scheduling a child’s immunizations or an adult weighing a new vaccine recommendation, knowing that antigens are the active ingredient—tailored, tested, and targeted—reinforces the science behind one of medicine’s most transformative tools.
Top Irish Banks Offering Equity Release Options in Ireland
You may want to see also
Explore related products






![]()
Adjuvants: Many include adjuvants to enhance immune system activation and vaccine effectiveness
Adjuvants are the unsung heroes of vaccines, quietly amplifying their power to protect. These substances, often minerals like aluminum salts (e.g., aluminum hydroxide or phosphate) or newer compounds like monophosphoryl lipid A (MPL), are added in microgram quantities to vaccines. Their role? To provoke a stronger immune response, ensuring the body not only recognizes the pathogen but also mounts a robust defense. Without adjuvants, many vaccines would require higher antigen doses or additional boosters, complicating their administration and increasing costs. For instance, the hepatitis B vaccine contains 0.5 mg of aluminum hydroxide per dose, a tiny amount that significantly boosts its efficacy without causing harm.
Consider the mechanism: adjuvants mimic infection signals, triggering the immune system’s danger sensors. They stimulate dendritic cells, the body’s antigen presenters, to activate T cells and B cells more effectively. This process is particularly crucial for subunit, recombinant, or conjugate vaccines, which contain only fragments of a pathogen rather than the whole organism. For example, the HPV vaccine uses an aluminum hydroxyphosphate sulfate adjuvant to enhance immunity against viral proteins, providing long-lasting protection with just a three-dose series, typically administered between ages 9 and 45.
However, adjuvants are not one-size-fits-all. Their selection depends on the vaccine type, target population, and desired immune response. While aluminum salts are safe and widely used, newer adjuvants like AS04 (found in the HPV and herpes zoster vaccines) combine aluminum with MPL to stimulate both antibody and cell-mediated immunity. This dual action is especially beneficial for older adults, whose immune systems may be less responsive. For instance, the shingles vaccine (Shingrix) uses AS04, achieving over 90% efficacy in adults over 50, a group often underserved by traditional vaccines.
Practical considerations matter too. Adjuvants can sometimes cause mild side effects, such as localized pain or swelling at the injection site, but these are transient and far outweighed by the benefits. Parents and caregivers should know that adjuvanted vaccines are rigorously tested for safety, with dosages carefully calibrated to maximize efficacy while minimizing risks. For example, the DTaP vaccine for children contains aluminum adjuvants in amounts well below the FDA’s safety limits, ensuring protection against diphtheria, tetanus, and pertussis without adverse effects.
In conclusion, adjuvants are a cornerstone of modern vaccinology, enabling precise, potent, and cost-effective immunization. Their inclusion transforms vaccines from mere antigen carriers into powerful immune trainers, capable of conferring lifelong protection. As vaccine technology evolves, so too will adjuvants, offering tailored solutions for diverse populations and emerging pathogens. Understanding their role empowers individuals to appreciate the science behind their shots and make informed decisions about their health.
Understanding Bank Bands: Which Bills Are Wrapped in 1,000 Straps?
You may want to see also
Explore related products






![]()
Preservatives: Some vaccines use preservatives to prevent contamination during storage and use
Vaccines, like any biological products, must remain sterile and stable from production to administration. Preservatives play a critical role in achieving this by inhibiting microbial growth that could otherwise render the vaccine ineffective or harmful. Commonly used preservatives include thiomersal (a mercury-containing compound) and phenoxyethanol, though their application varies depending on the vaccine type and intended population. For instance, multi-dose vials often contain preservatives to prevent contamination when repeated needle insertions are necessary, whereas single-dose vials typically omit them to minimize additional ingredients.
Consider the influenza vaccine, which is often distributed in multi-dose vials to healthcare providers. Thiomersal, present at a concentration of approximately 25 micrograms per dose, ensures the vaccine remains uncontaminated even after multiple punctures. This is particularly crucial in settings where rapid vaccination of large populations is necessary, such as during flu season. However, thiomersal’s inclusion has sparked controversy due to its mercury content, despite extensive research confirming its safety at these levels. As a result, preservative-free alternatives are increasingly available, especially for pediatric populations.
The choice of preservative is not arbitrary but guided by stringent regulatory standards. Phenoxyethanol, for example, is used in vaccines like the DTap (diphtheria, tetanus, and pertussis) vaccine at concentrations up to 0.005%. This preservative is favored for its effectiveness against bacteria and fungi while maintaining a favorable safety profile. Parents and caregivers should note that preservatives are rigorously tested to ensure they do not compromise the vaccine’s efficacy or pose health risks, particularly for infants and young children whose immune systems are still developing.
Practical considerations for healthcare providers include proper storage and handling of vaccines containing preservatives. Multi-dose vials should be discarded 28 days after first use, even if stored under refrigeration, to prevent potential contamination. Additionally, providers must verify the preservative content of each vaccine, especially when administering to individuals with known sensitivities. For instance, thiomersal-sensitive patients can safely receive preservative-free formulations, which are now widely available for most routine immunizations.
In summary, preservatives are a vital yet often overlooked component of vaccine formulation, ensuring safety and efficacy from manufacturing to administration. While their inclusion has been a subject of debate, regulatory bodies and scientific evidence affirm their necessity and safety in appropriate doses. Understanding their role empowers both healthcare providers and recipients to make informed decisions, fostering trust in vaccination programs and public health initiatives.
Citizens Bank: Simplify Rent Payments with Electronic Options
You may want to see also
Explore related products






![]()
Stabilizers: Stabilizers are added to maintain vaccine potency and stability over time
Vaccines are complex biological products that require careful formulation to ensure they remain effective from the manufacturing plant to the patient's arm. One critical component often overlooked is stabilizers, which play a pivotal role in maintaining vaccine potency and stability over time. Without these additives, vaccines could degrade during storage or transportation, rendering them ineffective or even harmful. Stabilizers act as guardians, preserving the integrity of the vaccine's active ingredients, whether they are live attenuated viruses, inactivated pathogens, or recombinant proteins.
Consider the measles, mumps, and rubella (MMR) vaccine, a staple in childhood immunization schedules. This vaccine contains sucrose as a stabilizer, which helps protect the live attenuated viruses from temperature fluctuations and physical stress. Sucrose forms a protective matrix around the viruses, preventing them from losing their structure or infectivity. Similarly, aluminum salts, commonly used in vaccines like DTaP (diphtheria, tetanus, and pertussis), serve a dual purpose: they enhance the immune response as adjuvants and stabilize the vaccine formulation. These stabilizers are particularly crucial for vaccines stored in liquid form, as they minimize the risk of aggregation or degradation during their shelf life, typically ranging from 12 to 24 months.
Not all stabilizers are created equal, and their selection depends on the vaccine’s composition and intended storage conditions. For instance, lyophilized (freeze-dried) vaccines, such as the smallpox vaccine, often contain lactose or mannitol. These stabilizers protect the vaccine during the freeze-drying process and ensure it remains stable in powder form until reconstitution. In contrast, mRNA vaccines like Pfizer-BioNTech’s COVID-19 vaccine rely on lipid nanoparticles and sucrose to protect the fragile mRNA molecules. The sucrose acts as a cryoprotectant, preventing damage during the ultra-cold storage required for these vaccines, typically at -70°C.
Practical considerations for healthcare providers and patients underscore the importance of stabilizers. Vaccines must be stored and handled according to manufacturer guidelines to preserve the stabilizers’ effectiveness. For example, exposing a vaccine to temperatures outside its recommended range can cause stabilizers to fail, leading to potency loss. Parents should ensure their child’s vaccines are administered from properly stored vials, while adults receiving vaccines like the annual flu shot should inquire about storage conditions if concerned. Understanding stabilizers also highlights why some vaccines require refrigeration while others can be stored at room temperature—a detail that impacts global vaccination efforts, especially in resource-limited settings.
In conclusion, stabilizers are unsung heroes in vaccine formulation, ensuring that life-saving immunizations remain reliable from production to administration. Their role extends beyond mere preservation, influencing vaccine accessibility, distribution, and efficacy. As vaccine technology advances, so too will the science of stabilizers, adapting to meet the demands of new formulations and storage challenges. Whether it’s sucrose in the MMR vaccine or lipids in mRNA vaccines, these additives are a testament to the precision and innovation behind modern immunizations.
Is PNC Bank Located in New Harmony, Indiana? Find Out Here
You may want to see also
Explore related products






![]()
Delivery Method: Vaccines are administered via injection, orally, or nasally for immune system access
Vaccines, regardless of their target disease, share a fundamental requirement: they must reach the immune system to trigger a protective response. This critical interaction is facilitated through specific delivery methods—injection, oral administration, or nasal sprays—each designed to optimize immune engagement. Injections, the most common method, deliver vaccines directly into muscle tissue (intramuscular) or just beneath the skin (subcutaneous), ensuring rapid uptake by immune cells. Oral vaccines, such as the rotavirus vaccine, are ingested and absorbed through the gastrointestinal tract, leveraging gut-associated lymphoid tissue to initiate immunity. Nasal sprays, like the live attenuated influenza vaccine (LAIV), deposit antigens in the mucosal lining of the nose, mimicking natural infection pathways and stimulating local immune defenses.
Consider the intramuscular injection, a method used for vaccines like the COVID-19 mRNA vaccines or the seasonal flu shot. Administered into the deltoid muscle for adults or the vastus lateralis muscle in infants, these vaccines typically require a dosage of 0.5 mL for adults and 0.25 mL for children. Proper technique is crucial: the needle should be inserted at a 90-degree angle, and the site should be rotated with each subsequent dose to prevent tissue damage. For oral vaccines, such as the Sabin polio vaccine, adherence to cold chain storage and administration on an empty stomach ensures efficacy. Nasal sprays, like LAIV, require careful insertion of the nozzle into one nostril at a time, with half the dose delivered to each side, particularly in children aged 2–8 years.
The choice of delivery method is not arbitrary but tailored to the vaccine’s formulation and the immune response desired. Injected vaccines often elicit systemic immunity, preparing the body to combat pathogens in the bloodstream. Oral and nasal vaccines, however, excel at inducing mucosal immunity, crucial for blocking pathogens at their primary entry points—the mouth, nose, and digestive tract. For instance, the oral cholera vaccine stimulates production of IgA antibodies in the gut, while nasal influenza vaccines prime the respiratory tract to fend off viral invaders. This strategic alignment of delivery method and immune pathway underscores the precision behind vaccine design.
Practical considerations also influence delivery method selection. Injections, while effective, require trained personnel and sterile equipment, making them less feasible in resource-limited settings. Oral vaccines offer convenience but may be compromised by factors like gastric acidity or poor absorption. Nasal sprays, though non-invasive, can provoke mild discomfort or require patient cooperation, particularly in young children. For caregivers and healthcare providers, understanding these nuances is essential for ensuring proper administration and maximizing vaccine efficacy. For example, parents administering LAIV should ensure the child inhales gently to draw the vaccine into the nasal passages, while oral vaccines should be stored at 2–8°C to maintain potency.
Ultimately, the delivery method is a bridge between vaccine and immune system, each route engineered to overcome unique challenges and harness specific immune mechanisms. Whether through the precision of an injection, the accessibility of an oral dose, or the ingenuity of a nasal spray, these methods share a singular goal: to safely and effectively prepare the body to defend against disease. By mastering their application, healthcare providers and recipients alike contribute to the global success of vaccination campaigns, one dose at a time.
Launching Your Small Bank: Essential Steps for Success
You may want to see also
Frequently asked questions
The primary purpose of all vaccines is to stimulate the immune system to recognize and combat specific pathogens, such as viruses or bacteria, thereby preventing or reducing the severity of diseases.
No, not all vaccines contain the same ingredients, but they often share common components like antigens (to trigger an immune response), adjuvants (to enhance the immune response), stabilizers, and preservatives.
All vaccines work by introducing a harmless form of a pathogen (or its components) to the immune system, training it to recognize and respond to the real pathogen if encountered in the future.
No, vaccines can be administered in different ways, such as injections (intramuscular or subcutaneous), orally, or nasally, depending on the vaccine type and its intended target in the body.
All vaccines undergo rigorous testing and clinical trials to ensure safety and efficacy before being approved for public use by regulatory authorities like the FDA or WHO.