Vaccine efficacy numbers, often reported as percentages, represent the reduction in disease risk among vaccinated individuals compared to those who are unvaccinated during clinical trials. For example, a vaccine with 95% efficacy means that vaccinated participants were 95% less likely to develop the disease than those who received a placebo. However, these numbers are not absolute guarantees of protection; they reflect the vaccine’s performance under controlled trial conditions. Real-world effectiveness can vary due to factors like virus mutations, population behavior, and individual immune responses. Additionally, efficacy may differ for preventing infection, severe illness, hospitalization, or death, so understanding the specific context of these numbers is crucial for interpreting their meaning and making informed decisions about vaccination.
| Characteristics | Values |
|---|---|
| Definition of Vaccine Efficacy | Percentage reduction in disease incidence in vaccinated group vs. placebo. |
| Absolute Risk Reduction (ARR) | Difference in disease risk between vaccinated and unvaccinated groups. |
| Relative Risk Reduction (RRR) | Percentage reduction in disease risk compared to unvaccinated group. |
| Number Needed to Vaccinate (NNV) | Number of individuals needing vaccination to prevent one case of disease. |
| Protection Against Severe Disease | Often higher than protection against mild or asymptomatic infection. |
| Waning Immunity | Efficacy may decrease over time, requiring booster doses. |
| Variant Impact | Efficacy can vary depending on the circulating virus variant. |
| Real-World vs. Clinical Trials | Real-world efficacy may differ from clinical trial results due to factors like population diversity and adherence. |
| Example (COVID-19 Pfizer Vaccine) | 95% efficacy in clinical trials (2020); real-world efficacy varies by variant and time since vaccination. |
| Public Health Impact | High efficacy reduces hospitalizations, deaths, and disease transmission. |
Explore related products






What You'll Learn
- Relative Risk Reduction: Percentage reduction in disease risk among vaccinated vs. unvaccinated groups
- Absolute Risk Reduction: Actual decrease in disease risk across the entire population
- Real-World vs. Clinical Trials: Efficacy differences between controlled trials and real-world settings
- Severity vs. Infection: Protection against severe disease vs. mild infection or transmission
- Duration of Efficacy: How long vaccine protection lasts post-immunization
![]()
Relative Risk Reduction: Percentage reduction in disease risk among vaccinated vs. unvaccinated groups
Vaccine efficacy numbers, particularly relative risk reduction (RRR), are often misunderstood. RRR measures the percentage by which the risk of disease is reduced in a vaccinated group compared to an unvaccinated group. For example, if a vaccine has a 90% RRR, it means vaccinated individuals are 90% less likely to develop the disease than those unvaccinated. This metric is crucial for understanding a vaccine’s impact on disease prevention but does not account for absolute risk differences or baseline disease rates.
To illustrate, consider a clinical trial where 1,000 participants are vaccinated and another 1,000 remain unvaccinated. If 100 unvaccinated individuals contract the disease and only 10 vaccinated individuals do, the RRR is calculated as [(100 - 10) / 100] × 100 = 90%. This means the vaccine reduces the risk of disease by 90% relative to the unvaccinated group. However, this figure alone doesn’t reveal the absolute number of cases prevented or the baseline risk in the population, which are equally important for context.
When interpreting RRR, it’s essential to consider the disease’s prevalence and severity. For instance, a 50% RRR for a rare but deadly disease may be less impactful than a 50% RRR for a common but mild illness. Public health decisions often weigh RRR alongside factors like vaccine availability, dosage requirements (e.g., single-dose vs. multi-dose regimens), and age-specific recommendations. For example, COVID-19 vaccines initially showed high RRR in clinical trials, but real-world efficacy varied based on factors like variants and waning immunity, necessitating booster doses for certain age groups, such as those over 65.
Practical tips for understanding RRR include comparing it with absolute risk reduction (ARR), which shows the actual decrease in disease incidence. For instance, if 2% of unvaccinated individuals get sick and 0.2% of vaccinated individuals do, the ARR is 1.8%. While RRR (90%) sounds more impressive, ARR provides a clearer picture of real-world impact. Additionally, consider the vaccine’s efficacy in specific populations—for example, flu vaccines often have lower RRR in older adults due to age-related immune decline, making adjuvanted doses (higher antigen content) a better choice for this group.
In summary, RRR is a powerful tool for assessing vaccine performance but requires context. It highlights the proportional benefit of vaccination but should be paired with absolute risk data, disease prevalence, and population-specific factors. By understanding RRR, individuals and policymakers can make informed decisions about vaccine use, dosage schedules, and targeted interventions to maximize public health benefits.
J&J Vaccine's Efficacy: How Well Does It Combat COVID Variants?
You may want to see also
Explore related products






![]()
Absolute Risk Reduction: Actual decrease in disease risk across the entire population
Vaccine efficacy numbers often grab headlines, but they don’t tell the whole story. While a 95% efficacy rate sounds impressive, it’s crucial to understand what it actually means for disease risk in the real world. This is where Absolute Risk Reduction (ARR) steps in—a metric that reveals the true impact of a vaccine by showing the actual decrease in disease risk across the entire population. Unlike relative risk reduction, which compares outcomes between vaccinated and unvaccinated groups, ARR focuses on the raw difference in risk, providing a clearer picture of a vaccine’s public health value.
Consider a hypothetical vaccine trial with 10,000 participants. In the unvaccinated group, 200 people develop the disease, representing a baseline risk of 2%. In the vaccinated group, only 10 people fall ill, resulting in a 0.1% risk. The ARR here is 1.9%—the difference between the two groups. While relative risk reduction might highlight a 95% decrease, ARR shows that the vaccine reduces the absolute risk by a modest but meaningful 1.9%. This distinction is vital, especially when baseline disease risk is low, as it prevents overestimation of a vaccine’s impact.
Calculating ARR is straightforward: subtract the incidence rate in the vaccinated group from the unvaccinated group. For instance, if a flu vaccine trial shows 3% of unvaccinated individuals get the flu versus 0.5% of vaccinated individuals, the ARR is 2.5%. This means the vaccine reduces the absolute risk of flu by 2.5 percentage points. Public health officials use ARR to decide which vaccines to prioritize, especially in populations with varying baseline risks, such as older adults or those with comorbidities.
Practical application of ARR is key. For example, a COVID-19 vaccine with an ARR of 1% in a low-transmission setting might not seem significant, but when applied to a population of millions, it translates to thousands of prevented cases. Conversely, in high-risk groups like the elderly, even a small ARR can justify widespread vaccination due to the potential severity of the disease. Clinicians and policymakers must weigh ARR alongside factors like vaccine availability, cost, and potential side effects to make informed decisions.
In summary, ARR bridges the gap between clinical trial data and real-world outcomes. It provides a tangible measure of a vaccine’s benefit, helping individuals and communities understand the actual reduction in disease risk. By focusing on ARR, we move beyond the allure of high efficacy numbers to a more nuanced appreciation of how vaccines protect populations. Whether you’re a healthcare provider, policymaker, or simply someone evaluating vaccine options, ARR is an essential tool for making evidence-based choices.
Banking on Safety: Exploring Cyber Security Policies in Financial Institutions
You may want to see also
Explore related products




![]()
Real-World vs. Clinical Trials: Efficacy differences between controlled trials and real-world settings
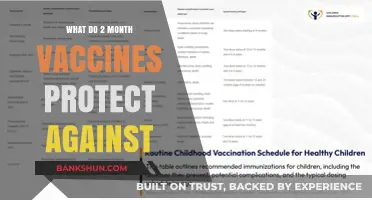
Vaccine efficacy numbers, often reported as percentages, can be misleading without context. A 95% efficacy rate in clinical trials doesn’t mean 5% of vaccinated individuals will get sick. Instead, it indicates that vaccinated participants were 95% less likely to develop the disease compared to the unvaccinated control group under specific conditions. These conditions—controlled environments, strict inclusion criteria, and adherence to protocols—rarely mirror real-world scenarios. For instance, the Pfizer-BioNTech COVID-19 vaccine’s 95% efficacy in trials was based on two doses administered 21 days apart, with participants monitored for symptoms and tested regularly. In contrast, real-world settings introduce variables like inconsistent dosing intervals, varying health statuses, and behavioral differences, which can alter outcomes.
Consider the influenza vaccine, which typically shows 40–60% efficacy in clinical trials but often performs lower in real-world populations. This discrepancy arises because trials exclude individuals with comorbidities, older adults, or those with weakened immune systems, who are more susceptible to infection. Real-world data from the CDC shows that flu vaccine effectiveness can drop to 20–30% in seasons with dominant strains not well-matched by the vaccine. Similarly, the COVID-19 vaccines’ efficacy against symptomatic infection has varied globally, with Israel reporting 94% effectiveness for Pfizer in early 2021, while South Africa, facing the Beta variant, saw efficacy drop to 75%. These differences highlight how viral variants, population immunity, and healthcare infrastructure influence real-world outcomes.
To bridge the gap between trials and reality, public health strategies must account for these variables. For example, booster doses have been recommended for COVID-19 vaccines to maintain protection against waning immunity and emerging variants. In the U.S., the CDC advises a second booster for individuals over 50 or immunocompromised, based on real-world data showing reduced hospitalization rates. Similarly, adjusting vaccine formulations annually, as done for the flu vaccine, ensures better alignment with circulating strains. Practical tips for individuals include adhering to recommended dosing schedules, staying updated on booster guidelines, and maintaining general health to optimize vaccine response.
The takeaway is that vaccine efficacy numbers are not absolute but reflect performance under ideal conditions. Real-world effectiveness depends on factors like population demographics, viral evolution, and healthcare access. Policymakers and individuals must interpret these numbers critically, using them as a baseline rather than a guarantee. For instance, a vaccine with 70% efficacy in trials may still prevent severe disease and death in 90% of real-world cases, making it a valuable tool despite lower headline numbers. Understanding this distinction ensures informed decision-making and realistic expectations in public health efforts.
Tide Bank's Customer Base: Unveiling the Number of Users in 2023
You may want to see also
Explore related products






![]()
Severity vs. Infection: Protection against severe disease vs. mild infection or transmission
Vaccine efficacy numbers often highlight a critical distinction: protection against severe disease versus protection against mild infection or transmission. For instance, the Pfizer-BioNTech COVID-19 vaccine demonstrated 95% efficacy in preventing symptomatic infection in clinical trials, but real-world data later showed its effectiveness against severe disease remained high (over 90%) even as protection against mild infection waned over time. This disparity underscores a fundamental truth: vaccines are primarily designed to prevent serious illness, hospitalization, and death, not necessarily to block every minor infection or transmission.
Consider the mechanism at play. Vaccines train the immune system to recognize and combat pathogens, but this training focuses on preventing the virus from causing severe harm rather than eliminating it entirely. For example, a vaccinated individual exposed to SARS-CoV-2 might still contract the virus and experience mild symptoms like a cough or fever, but their immune system is primed to prevent the virus from replicating uncontrollably, thus avoiding pneumonia or organ failure. This is why public health officials emphasize that "breakthrough infections" in vaccinated individuals are typically mild and rarely lead to hospitalization.
The distinction between severity and infection has practical implications for public health strategies. While vaccines reduce transmission to some extent, they are not foolproof in preventing spread, especially with highly contagious variants like Omicron. This is why additional measures, such as masking and testing, remain crucial in high-risk settings. For instance, a study in *The Lancet* found that vaccinated individuals with breakthrough infections had lower viral loads than unvaccinated individuals, reducing but not eliminating transmission risk. This highlights the need for layered protection, particularly in vulnerable populations like the elderly or immunocompromised.
From a personal health perspective, understanding this distinction empowers individuals to make informed decisions. For example, a 65-year-old with comorbidities should prioritize vaccination and boosters to minimize the risk of severe COVID-19, even if they might still catch a mild version of the virus. Conversely, a healthy 25-year-old might focus on reducing transmission by staying up-to-date on vaccines and taking precautions during outbreaks. Practical tips include monitoring local infection rates, wearing masks in crowded indoor spaces, and getting tested if symptoms arise, regardless of vaccination status.
In conclusion, vaccine efficacy numbers are not a binary measure of success or failure but a nuanced indicator of protection. They remind us that vaccines are a powerful tool against severe disease, even if they don’t entirely prevent infection or transmission. By focusing on this distinction, individuals and policymakers can tailor strategies to maximize public health benefits, ensuring that vaccines continue to save lives while acknowledging their limitations.
Is Karnataka Bank Ltd a Nationalised Bank? Facts Revealed
You may want to see also
Explore related products






![]()
Duration of Efficacy: How long vaccine protection lasts post-immunization
Vaccine efficacy numbers often grab headlines, but they rarely tell the full story. One critical aspect frequently overlooked is the duration of efficacy—how long the protection offered by a vaccine actually lasts. Unlike a one-time shield, vaccine-induced immunity can wane over time, influenced by factors like the vaccine type, the pathogen it targets, and individual immune responses. For instance, the measles vaccine provides lifelong immunity after two doses, while the flu vaccine requires annual updates due to the virus’s rapid mutation. Understanding this temporal dimension is essential for both public health planning and personal decision-making.
Consider the COVID-19 vaccines, which have brought this issue into sharp focus. Initial studies showed efficacy rates of 90–95% for mRNA vaccines like Pfizer and Moderna, but these numbers were based on short-term data. Over time, protection against infection and mild illness has been observed to decline, particularly against new variants. However, the vaccines have maintained high efficacy against severe disease, hospitalization, and death, even months after the primary series. Booster doses, typically administered 6–12 months post-immunization, have proven effective in restoring and extending this protection. For older adults or immunocompromised individuals, whose immune systems may respond less robustly, more frequent boosters may be recommended.
The duration of efficacy also varies by vaccine mechanism. Live-attenuated vaccines, like the MMR (measles, mumps, rubella), often confer long-lasting immunity because they mimic natural infection, stimulating a robust and enduring immune memory. In contrast, inactivated or subunit vaccines, such as the hepatitis B vaccine, may require multiple doses and periodic boosters to maintain protection. For example, the tetanus vaccine’s efficacy typically lasts 10 years, necessitating regular booster shots to ensure ongoing immunity. Understanding these differences helps individuals and healthcare providers tailor vaccination schedules to specific needs.
Practical tips can maximize the duration of vaccine efficacy. First, adhere to the recommended dosing schedule—skipping or delaying doses can compromise immunity. Second, stay informed about booster recommendations, especially for vaccines like COVID-19 or flu, where guidance evolves with new data. Third, maintain a healthy lifestyle; factors like adequate sleep, nutrition, and exercise can support immune function. Finally, keep vaccination records handy, as they provide critical information for healthcare providers to assess your immunity status and recommend appropriate actions.
In conclusion, the duration of vaccine efficacy is a dynamic and vaccine-specific metric that requires ongoing attention. While some vaccines offer decades-long protection, others demand periodic reinforcement. By understanding these nuances and taking proactive steps, individuals can ensure they remain protected against preventable diseases. Public health systems, too, must account for waning immunity in their strategies, balancing the need for boosters with resource allocation and accessibility. Ultimately, the goal is not just to achieve immunity but to sustain it—a task that demands both scientific rigor and individual vigilance.
How to Join a Staff Bank: A Step-by-Step Guide
You may want to see also
Frequently asked questions
The percentage in vaccine efficacy numbers represents the reduction in disease risk among vaccinated individuals compared to unvaccinated individuals in a clinical trial. For example, 95% efficacy means vaccinated people had 95% less risk of getting the disease than those who weren’t vaccinated.
No, 95% efficacy doesn’t mean 5% of vaccinated people will get sick. It means the vaccine reduced the overall risk of disease by 95% in the study population. The actual number of vaccinated people who get sick depends on the disease’s prevalence and other factors.
Vaccine efficacy numbers can vary due to differences in study design, population demographics, circulating virus variants, and the prevalence of the disease in the study area. Real-world effectiveness may also differ from clinical trial results due to these factors.
Vaccine efficacy refers to how well a vaccine performs under controlled conditions, like in a clinical trial. Vaccine effectiveness measures how well it works in the real world, where conditions are less controlled and more variable.
No, a vaccine with 70% efficacy is still highly valuable. It means the vaccine reduces the risk of disease by 70%, which can significantly lower hospitalizations, severe illness, and deaths, even if it doesn’t prevent all cases. Public health benefits are still substantial.