Vaccination drugs, though often perceived as a single entity, encompass a diverse array of formulations tailored to specific pathogens and delivery methods. At their core, these drugs typically consist of a key component—the antigen—which can be a weakened or inactivated pathogen, a fragment of the pathogen, or a genetically engineered protein mimicking the pathogen. This antigen is often accompanied by adjuvants, substances that enhance the immune response, and stabilizers to maintain the vaccine’s efficacy during storage. Vaccines can take various physical forms, such as liquid solutions for injection, freeze-dried powders requiring reconstitution, or even oral formulations like drops or tablets. The appearance of a vaccination drug can thus range from clear or slightly cloudy vials to pre-filled syringes or small, dissolvable pills, each designed to ensure safe and effective delivery of the protective antigen into the body.
Explore related products






What You'll Learn
- Vaccine Formulations: Liquid, powder, or nasal spray forms for different administration methods
- Adjuvants in Vaccines: Enhance immune response, often included in vaccine compositions
- Antigen Types: Live, attenuated, inactivated, or subunit antigens in vaccines
- Vaccine Vials: Glass containers with rubber stoppers for storage and distribution
- Excipients in Vaccines: Stabilizers, preservatives, and buffers ensuring vaccine safety and efficacy
![]()
Vaccine Formulations: Liquid, powder, or nasal spray forms for different administration methods
Vaccines, the cornerstone of preventive medicine, come in various formulations tailored to specific administration methods and patient needs. The most common forms include liquids, powders, and nasal sprays, each designed to optimize efficacy, stability, and ease of use. Liquid vaccines, such as the measles-mumps-rubella (MMR) shot, are pre-filled in vials or syringes and administered via intramuscular or subcutaneous injection. These formulations often contain preservatives like thiomersal to maintain sterility and adjuvants like aluminum salts to enhance immune response. For instance, the influenza vaccine in liquid form typically requires a 0.5 mL dose for adults and a 0.25 mL dose for children aged 6 months to 3 years, highlighting the importance of precise dosing based on age.
Powdered vaccines, on the other hand, offer a unique advantage in terms of stability and storage, particularly in resource-limited settings. These vaccines are lyophilized (freeze-dried) and require reconstitution with a diluent before administration. The Bacillus Calmette-Guérin (BCG) vaccine for tuberculosis is a classic example, supplied as a freeze-dried pellet that is mixed with 0.1 mL of diluent for intradermal injection. This form is ideal for regions with unreliable refrigeration, as it can remain viable at room temperature for extended periods. However, healthcare providers must follow strict reconstitution protocols to ensure potency, such as using sterile water and avoiding shaking the vial to prevent denaturation of the vaccine components.
Nasal spray vaccines represent a non-invasive alternative, particularly for respiratory pathogens like influenza. The live attenuated influenza vaccine (LAIV), marketed as FluMist, is administered as a 0.2 mL dose (0.1 mL per nostril) for individuals aged 2 to 49 years. This method leverages the mucosal immune system, providing rapid protection against viral entry. However, it is contraindicated for pregnant individuals and those with weakened immune systems, underscoring the need for personalized vaccine selection. The spray’s ease of administration makes it a preferred choice for pediatric populations, reducing anxiety associated with needles.
Comparing these formulations reveals trade-offs in convenience, stability, and immunogenicity. Liquid vaccines offer immediate readiness but require cold chain maintenance, while powdered vaccines demand reconstitution but excel in durability. Nasal sprays eliminate needle phobia but have narrower indications. For instance, a study comparing intramuscular and intranasal influenza vaccines found that the latter elicited stronger mucosal immunity but was less effective in older adults due to age-related immune decline. This highlights the importance of matching formulation to target population and disease characteristics.
Practical considerations further dictate formulation choice. In mass vaccination campaigns, pre-filled liquid syringes streamline administration, reducing the risk of dosage errors. Powdered vaccines are ideal for remote areas, where refrigeration is scarce. Nasal sprays, while convenient, require careful technique to ensure proper delivery. For example, recipients of LAIV should avoid blowing their nose or sneezing immediately after administration to prevent expulsion of the vaccine. Understanding these nuances empowers healthcare providers to select the most appropriate formulation, ensuring optimal protection for diverse populations.
Millstone to Red Bank: Distance, Travel Time, and Route Guide
You may want to see also
Explore related products






![]()
Adjuvants in Vaccines: Enhance immune response, often included in vaccine compositions
Vaccines are not just about the active ingredient that triggers an immune response; they often contain adjuvants, substances that enhance the body’s immune reaction to the antigen. Adjuvants are critical in modern vaccine formulations, particularly for vaccines targeting diseases like influenza, HPV, and COVID-19. For instance, aluminum salts (alum) have been used as adjuvants for nearly a century, appearing as a white, powdery substance when isolated but typically dissolved in liquid vaccine formulations. These compounds act by creating a depot effect, slowing the release of the antigen and prolonging immune system exposure, which amplifies the response. In vaccines like the hepatitis B shot, alum adjuvants ensure robust immunity even with a lower antigen dose, reducing side effects while maintaining efficacy.
Consider the role of adjuvants in pediatric vaccines, where the immune system is still maturing. Vaccines like DTaP (diphtheria, tetanus, pertussis) often include alum to ensure children as young as 2 months develop sufficient immunity. Dosage adjustments are crucial here; infants receive smaller volumes (0.5 mL) compared to adults (0.5–1 mL), but the adjuvant concentration remains consistent to standardize the immune boost. Newer adjuvants, such as AS04 (used in the HPV vaccine Cervarix), combine alum with MPL (monophosphoryl lipid A), a derivative of bacterial lipopolysaccharide. This combination not only strengthens the immune response but also shifts it toward a Th1-type response, critical for combating intracellular pathogens. Practical tip: Always verify the adjuvant type in a vaccine, as some individuals may experience localized reactions like redness or swelling, typically mild and short-lived.
The inclusion of adjuvants also addresses challenges in vaccine development for the elderly, whose immune systems often respond weakly to antigens. The shingles vaccine Shingrix, for example, uses a liposome-based adjuvant system (AS01B) containing MPL and a saponin extract called QS-21. This formulation boosts antibody production by 10–100 times compared to earlier vaccines without adjuvants. For adults over 50, the recommended two-dose series (0.5 mL each) achieves over 90% efficacy, a significant improvement over previous non-adjuvanted versions. Comparative analysis shows that adjuvants like AS01B not only enhance potency but also reduce the antigen load required, lowering production costs and increasing vaccine accessibility.
Persuasively, adjuvants are not just additives but essential components that tailor vaccines to specific populations and diseases. For instance, oil-in-water emulsions like MF59 (used in flu vaccines for seniors) mimic natural immune triggers, stimulating both humoral and cellular responses. Studies show that MF59-adjuvanted flu vaccines reduce influenza-related hospitalizations in adults over 65 by 20–30%, a critical benefit for a vulnerable demographic. However, caution is warranted: while adjuvants improve efficacy, they can also increase reactogenicity, such as injection site pain or fatigue. Healthcare providers should educate patients on these potential side effects, emphasizing their transient nature and the long-term benefits of enhanced immunity.
In conclusion, adjuvants transform vaccines from simple antigen carriers into sophisticated immunological tools. From alum’s time-tested reliability to cutting-edge systems like AS01B and MF59, these substances ensure vaccines meet the diverse needs of global populations. When examining a vaccine’s composition, look beyond the antigen—the adjuvant often holds the key to its effectiveness. Practical takeaway: Always consult vaccine package inserts for adjuvant details, especially when administering to immunocompromised or elderly patients, to optimize safety and efficacy.
Cayman Islands Banks: Exploring Their Presence in the Global Financial Landscape
You may want to see also
Explore related products

$28.99 $32.99





![]()
Antigen Types: Live, attenuated, inactivated, or subunit antigens in vaccines
Vaccines are not one-size-fits-all; they are tailored to the specific pathogen they target, and a key part of this customization is the type of antigen used. Antigens are the substances in vaccines that trigger the immune system to produce antibodies, preparing the body to fight off future infections. The choice of antigen type—live, attenuated, inactivated, or subunit—depends on factors like the pathogen's nature, the desired immune response, and safety considerations. Each type has unique characteristics, advantages, and limitations, shaping how vaccines are developed, administered, and stored.
Live, attenuated vaccines contain a weakened version of the pathogen, which is still alive but unable to cause severe disease. Examples include the measles, mumps, and rubella (MMR) vaccine and the varicella (chickenpox) vaccine. These vaccines mimic a natural infection, prompting a robust and long-lasting immune response. A single dose often confers lifelong immunity, as seen with the yellow fever vaccine. However, live vaccines require careful handling, as they must be stored and transported at specific temperatures (typically 2–8°C) to maintain viability. They are generally not recommended for immunocompromised individuals or pregnant women due to the theoretical risk of the virus reverting to a virulent form. For instance, the MMR vaccine is administered as a 0.5 mL dose subcutaneously to children at 12–15 months, with a second dose at 4–6 years.
Inactivated vaccines, in contrast, use a killed version of the pathogen or its toxins. Examples include the injectable influenza vaccine and the polio vaccine (IPV). These vaccines are safer for immunocompromised individuals because there’s no risk of the pathogen causing disease. However, they often require multiple doses and adjuvants (e.g., aluminum salts) to enhance the immune response. For instance, the IPV is given as a 0.5 mL dose intramuscularly or subcutaneously, with a series of four doses starting at 2 months of age. Booster shots are typically needed to maintain immunity, such as the tetanus-diphtheria-pertussis (Tdap) vaccine, which is recommended every 10 years for adults.
Subunit vaccines take precision a step further by using only specific pieces of the pathogen, such as proteins or sugars, to stimulate immunity. The hepatitis B vaccine, which contains the virus’s surface antigen (HBsAg), and the human papillomavirus (HPV) vaccine, which uses virus-like particles, are prime examples. Subunit vaccines are highly safe because they cannot cause the disease, even in immunocompromised individuals. However, like inactivated vaccines, they often require adjuvants and multiple doses to achieve adequate protection. The HPV vaccine, for instance, is administered as a 0.5 mL dose intramuscularly, with a 2- or 3-dose schedule depending on the recipient’s age (2 doses for those under 15, 3 doses for those 15 and older).
Choosing the right antigen type is a delicate balance of efficacy, safety, and practicality. Live, attenuated vaccines offer strong immunity but come with storage and safety constraints. Inactivated vaccines are safer but may require boosters. Subunit vaccines are precise and safe but often need adjuvants to be effective. Understanding these differences empowers healthcare providers and patients to make informed decisions about vaccination, ensuring the best possible protection against infectious diseases. For example, travelers to regions with a high risk of yellow fever would benefit from the live, attenuated vaccine’s long-lasting immunity, while a pregnant woman might opt for the inactivated influenza vaccine to protect herself and her unborn child. Each antigen type plays a unique role in the global effort to prevent disease, highlighting the sophistication and diversity of modern vaccine design.
Step-by-Step Guide to Registering UPI on Axis Bank Account
You may want to see also
Explore related products
![Vaccines: Are They Really Safe and Effective? [VACCINES UPDATED AND REVIS -OS]](https://m.media-amazon.com/images/I/41yjhcd2-dL._AC_UY218_.jpg)





![]()
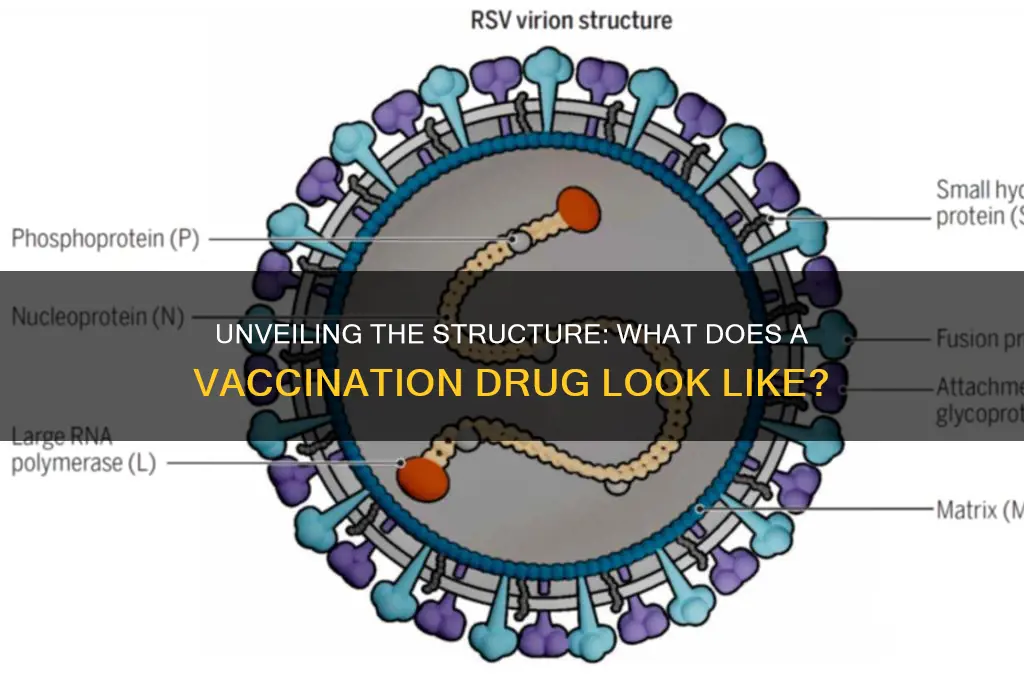
Vaccine Vials: Glass containers with rubber stoppers for storage and distribution
Vaccine vials, typically made of glass with rubber stoppers, are the unsung heroes of immunization programs worldwide. These containers are designed to safeguard the potency of vaccines from manufacturing to administration. Glass is chosen for its inert nature, ensuring it doesn’t react with the vaccine, while the rubber stopper provides an airtight seal to prevent contamination. For instance, a standard 10-dose vial of the measles vaccine contains 0.5 mL per dose, with the stopper allowing for multiple needle punctures without compromising the vaccine’s integrity. This design is critical for vaccines that require reconstitution, such as the MMR vaccine, where a diluent is added to the vial just before use.
The manufacturing process of these vials is as precise as the vaccines they hold. Glass vials are formed under high temperatures and then treated to remove impurities, ensuring they meet stringent pharmaceutical standards. The rubber stoppers, often made of bromobutyl or chlorobutyl rubber, are coated with a lubricant to facilitate easy needle penetration while maintaining a secure seal. For vaccines like the influenza vaccine, which is distributed in both single-dose and multi-dose vials, the stopper’s durability is tested to withstand up to 20 punctures without leakage. This attention to detail ensures that vaccines remain stable during storage and transportation, even in challenging environments like remote clinics or during global health emergencies.
When handling vaccine vials, healthcare providers must follow specific protocols to maintain efficacy. For example, multi-dose vials of the COVID-19 vaccine, such as the Pfizer-BioNTech formulation, require careful management to prevent wastage. After the first puncture, the vial can be stored for up to 30 days in a refrigerator, but each subsequent use must adhere to aseptic techniques to avoid contamination. Single-dose vials, on the other hand, are discarded immediately after use, even if some vaccine remains. This distinction highlights the importance of understanding vial types and their handling requirements, especially in mass vaccination campaigns where efficiency and safety are paramount.
The design of vaccine vials also reflects considerations for global distribution. Glass vials are lightweight yet durable, making them suitable for transport to remote areas with limited infrastructure. However, their fragility poses challenges, particularly in regions with extreme temperatures or rough handling conditions. Innovations like prefilled syringes and plastic vials are emerging as alternatives, but glass remains the gold standard due to its proven reliability. For vaccines requiring ultra-cold storage, such as the mRNA COVID-19 vaccines, specialized vials with thicker glass walls are used to withstand freezing temperatures without cracking. These adaptations ensure that vaccines reach their intended recipients in optimal condition, regardless of the logistical hurdles.
In conclusion, vaccine vials are more than just containers; they are critical components of global health initiatives. Their design, from the inert glass to the resilient rubber stoppers, is tailored to protect vaccines from contamination, temperature fluctuations, and physical damage. Understanding their features and handling requirements empowers healthcare providers to administer vaccines safely and efficiently. As vaccination programs continue to evolve, the humble vial remains a cornerstone of their success, bridging the gap between production and protection.
When to Vaccinate for Mumps: Age Guidelines and Recommendations
You may want to see also
Explore related products






![]()
Excipients in Vaccines: Stabilizers, preservatives, and buffers ensuring vaccine safety and efficacy
Vaccines are not just about the active ingredient that triggers an immune response; they are complex formulations where every component plays a critical role. Excipients—stabilizers, preservatives, and buffers—are the unsung heroes that ensure vaccines remain safe, effective, and functional from manufacturing to administration. Without these additives, vaccines could degrade, lose potency, or become contaminated, rendering them ineffective or even harmful. Understanding their role is essential for appreciating the meticulous science behind every vial.
Consider stabilizers, which act as molecular guardians, protecting the vaccine’s active components from environmental stresses like heat, light, and freezing. Common stabilizers include sugars such as sucrose or lactose, which form a protective matrix around the antigen, preventing structural damage during storage and transport. For example, mRNA vaccines like Pfizer-BioNTech’s COVID-19 vaccine use lipid nanoparticles encased in a sugar-based stabilizer to maintain their integrity at ultra-low temperatures. Without these stabilizers, the delicate mRNA strands would degrade, rendering the vaccine ineffective. This is why storage conditions, such as the -70°C requirement for Pfizer’s vaccine, are so critical—they work in tandem with stabilizers to preserve efficacy.
Preservatives, on the other hand, are the sentinels against microbial contamination, ensuring that multi-dose vials remain sterile after repeated needle insertions. Thimerosal, a mercury-based preservative, has been used for decades in vaccines like influenza shots, typically at a concentration of 0.01% (1 part per 10,000). Despite misconceptions about its safety, extensive research confirms that the ethylmercury in thimerosal is rapidly excreted by the body and does not accumulate like its toxic cousin, methylmercury. For those still concerned, single-dose vials are available, which eliminate the need for preservatives altogether. This flexibility ensures that vaccines remain accessible and safe for all populations, including infants and pregnant individuals.
Buffers are the pH regulators, maintaining the vaccine’s chemical environment within a narrow, optimal range. A slight deviation in pH can denature proteins or disrupt the vaccine’s structure, compromising its effectiveness. Phosphate buffers, for instance, are commonly used in vaccines like DTaP (diphtheria, tetanus, and pertussis) to keep the pH stable around 7.0–7.4, mimicking the body’s natural conditions. This stability is particularly crucial during lyophilization (freeze-drying), a process used for vaccines like the MMR (measles, mumps, rubella) vaccine, where buffers prevent pH shifts that could occur during reconstitution with diluents.
In practice, excipients are carefully selected and tested to ensure they do not interfere with the vaccine’s immunogenicity or cause adverse reactions. For example, aluminum salts (alum), used as adjuvants in vaccines like hepatitis B, also act as stabilizers by binding to antigens and preventing their rapid degradation. However, their use is strictly regulated, with maximum allowable doses (e.g., 0.85 mg of aluminum per dose in pediatric vaccines) to minimize the risk of local reactions like redness or swelling. Parents and caregivers can take comfort in knowing that these additives are rigorously evaluated for safety across all age groups, from newborns to the elderly.
In conclusion, excipients are the backbone of vaccine formulation, ensuring that every dose delivered is as potent and safe as the day it was manufactured. From stabilizers that shield against environmental damage to preservatives that guard against contamination and buffers that maintain chemical balance, these components work in harmony to support the vaccine’s primary purpose: protecting public health. Next time you receive a vaccine, remember that its effectiveness is not just about the antigen—it’s about the entire formulation, meticulously designed to safeguard your well-being.
Associated Bank ATM Fees: Where to Find Free Withdrawals
You may want to see also
Frequently asked questions
A vaccination drug usually appears as a clear or slightly cloudy liquid in a small glass or plastic vial, often ranging in size from 1 to 10 milliliters.
No, vaccination drugs can vary in color depending on the specific vaccine. Some are colorless or clear, while others may have a slight tint, such as pale yellow or pink, due to their formulation.
Vaccination drugs are typically packaged in sterile vials or pre-filled syringes, often accompanied by a box or label containing information about the vaccine, dosage, and expiration date.
Most vaccination drugs are administered as liquids, either pre-mixed or requiring reconstitution from a powdered form. Rarely, some vaccines may come in other forms, such as freeze-dried powders that need to be mixed with a diluent before use.