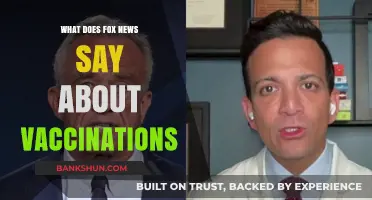
The efficacy rate of a vaccine is a critical measure that indicates how well it prevents disease in a controlled clinical trial setting. Expressed as a percentage, it compares the incidence of disease among vaccinated individuals to that of an unvaccinated or placebo group. For example, a vaccine with a 95% efficacy rate means that vaccinated participants were 95% less likely to develop the disease than those who were not vaccinated. This metric is essential for evaluating a vaccine’s performance and its potential impact on public health, though it is distinct from effectiveness, which measures real-world performance outside of clinical trials. Understanding efficacy rates helps policymakers, healthcare providers, and the public gauge the reliability and benefits of vaccination programs.
| Characteristics | Values |
|---|---|
| Definition | The percentage reduction in disease incidence in vaccinated individuals compared to unvaccinated individuals in a clinical trial. |
| Calculation Formula | Efficacy Rate = (1 - Risk Ratio) × 100, where Risk Ratio = (Disease Cases in Vaccinated Group) / (Disease Cases in Placebo Group). |
| Primary Endpoint | Typically measured as the prevention of symptomatic disease, severe disease, hospitalization, or death. |
| Duration of Measurement | Varies by trial design, often assessed over 6 months to 1 year post-vaccination. |
| Example Efficacy Rates | Pfizer-BioNTech: 95% (original strain), Moderna: 94.1% (original strain), AstraZeneca: 70-82% (depending on dosing interval). |
| Factors Affecting Efficacy | Virus variant, dosing interval, age of recipients, immune status, and trial population demographics. |
| Real-World vs. Clinical Trials | Real-world efficacy may differ due to population variability, vaccine rollout conditions, and emerging variants. |
| Efficacy vs. Effectiveness | Efficacy is measured in controlled trials, while effectiveness refers to real-world performance. |
| Minimum Threshold for Approval | Typically 50% or higher, as recommended by regulatory bodies like the FDA and WHO. |
| Waning Efficacy | Efficacy may decrease over time, necessitating booster doses for sustained protection. |
| Limitations | Does not measure prevention of infection or asymptomatic transmission unless specifically studied. |
Explore related products






What You'll Learn
- Understanding Efficacy vs. Effectiveness: Key differences in controlled trials versus real-world vaccine performance metrics
- Measuring Efficacy Rates: How vaccine trials calculate and report prevention of disease or infection
- Efficacy Rate Thresholds: What percentage is considered sufficient for public health approval and use
- Factors Affecting Efficacy: Role of variants, immune response, and population demographics in vaccine performance
- Efficacy vs. Severity Reduction: How vaccines may prevent illness, hospitalization, or death despite lower efficacy rates
![]()
Understanding Efficacy vs. Effectiveness: Key differences in controlled trials versus real-world vaccine performance metrics
Vaccine efficacy and effectiveness are often used interchangeably, but they measure different aspects of a vaccine’s performance. Efficacy refers to how well a vaccine works under ideal, controlled conditions, such as in a clinical trial. For example, the Pfizer-BioNTech COVID-19 vaccine demonstrated a 95% efficacy rate in its Phase 3 trial, meaning it reduced the risk of symptomatic infection by 95% among participants who received two doses spaced 21 days apart, compared to those who received a placebo. This metric is critical for regulatory approval, as it provides a clear, standardized measure of a vaccine’s potential impact.
Effectiveness, on the other hand, assesses how well a vaccine performs in the real world, outside the controlled environment of a trial. Factors like varying dosages, inconsistent administration, and diverse population health statuses can influence outcomes. For instance, a study published in *The Lancet* found that the effectiveness of the Pfizer vaccine dropped to 84% against symptomatic infection in a real-world Israeli population, where adherence to dosing schedules and storage conditions might differ from trial settings. This gap highlights why effectiveness is a more dynamic and context-dependent metric.
Understanding these differences is crucial for interpreting vaccine data. Efficacy trials often exclude individuals with comorbidities or those outside specific age ranges (e.g., 16–85 years for Pfizer’s trial), creating a homogeneous study population. In contrast, real-world effectiveness studies include a broader demographic, such as elderly individuals or those with chronic conditions, who may respond differently to vaccination. For example, a CDC study showed that COVID-19 vaccine effectiveness was lower in adults aged 65 and older compared to younger populations, emphasizing the need for tailored public health strategies.
Practical tips for interpreting these metrics include recognizing that efficacy rates are aspirational benchmarks, while effectiveness rates provide actionable insights for policymakers. For instance, if a vaccine’s effectiveness against hospitalization drops below 70% in a specific population, booster doses or additional measures might be recommended. Additionally, consider the vaccine’s mechanism: mRNA vaccines like Moderna’s (94% efficacy in trials) may show higher initial efficacy but require specific storage (e.g., -20°C), whereas viral vector vaccines like AstraZeneca’s (70% efficacy) are more logistically flexible but may have lower effectiveness in preventing mild cases.
In summary, efficacy and effectiveness serve distinct purposes in evaluating vaccines. Efficacy provides a controlled, idealized measure, while effectiveness reflects real-world complexities. By understanding these differences, stakeholders can make informed decisions about vaccine deployment, dosing schedules, and population-specific interventions, ensuring maximum public health impact.
Is the Chicken Pox Vaccine Mandatory in Pennsylvania?
You may want to see also
Explore related products






![]()
Measuring Efficacy Rates: How vaccine trials calculate and report prevention of disease or infection
Vaccine efficacy rates are calculated through rigorously designed clinical trials that compare disease or infection rates between vaccinated and unvaccinated groups. In a typical Phase III trial, thousands of participants are randomly assigned to receive either the vaccine or a placebo. Researchers then monitor both groups over time, often through blood tests or symptom reporting, to determine how many individuals in each group contract the disease. The efficacy rate is derived from the difference in infection rates between the two groups, expressed as a percentage. For example, if 100 out of 10,000 unvaccinated participants contract a disease while only 10 out of 10,000 vaccinated participants do, the vaccine’s efficacy rate is calculated as 90% [(100 - 10) / 100 × 100].
One critical aspect of measuring efficacy is the trial’s endpoint, which defines what constitutes a "case" of the disease. Endpoints can vary—some trials focus on preventing symptomatic infection, while others aim to block severe disease or hospitalization. For instance, the Pfizer-BioNTech COVID-19 vaccine trial reported 95% efficacy in preventing symptomatic COVID-19, but its protection against asymptomatic infection or transmission was not initially measured. This distinction highlights why efficacy rates must be interpreted in the context of the trial’s specific goals and endpoints.
Another factor influencing efficacy rates is the population studied. Trials often stratify participants by age, health status, and geographic location to assess how these variables affect vaccine performance. For example, the influenza vaccine typically shows lower efficacy in older adults due to age-related immune decline. Similarly, the dengue vaccine Dengvaxia demonstrated higher efficacy in individuals with prior dengue exposure compared to those without. Such variations underscore the importance of reporting efficacy rates for specific subgroups, ensuring that public health decisions are tailored to diverse populations.
Practical considerations also play a role in calculating and reporting efficacy. Trials must account for adherence to the vaccine regimen, such as receiving the correct dosage and completing all required doses. For vaccines like the HPV vaccine, which requires two or three doses depending on age (e.g., two doses for those under 15 and three doses for older individuals), adherence is critical for achieving optimal efficacy. Additionally, real-world effectiveness may differ from trial results due to factors like vaccine storage, administration errors, or behavioral changes post-vaccination.
In conclusion, measuring vaccine efficacy rates involves meticulous trial design, clear endpoint definitions, and consideration of population variability. These rates provide a snapshot of a vaccine’s performance under controlled conditions but must be complemented by real-world surveillance to fully understand their impact. For individuals, knowing a vaccine’s efficacy helps set realistic expectations, while for policymakers, it guides allocation and prioritization strategies. By demystifying how efficacy rates are calculated and reported, stakeholders can make informed decisions about vaccine use and public health interventions.
Huntington Bank Hours: When Can You Bank?
You may want to see also
Explore related products






![]()
Efficacy Rate Thresholds: What percentage is considered sufficient for public health approval and use
Vaccine efficacy rates are a critical measure of how well a vaccine prevents disease under ideal conditions, but what percentage is good enough for public health approval? Regulatory bodies like the World Health Organization (WHO) and the U.S. Food and Drug Administration (FDA) generally require vaccines to demonstrate at least 50% efficacy to be considered for approval. This threshold is based on the principle that even a moderately effective vaccine can significantly reduce disease burden when widely administered. For instance, the FDA’s guidance during the COVID-19 pandemic set a minimum efficacy benchmark of 50% for emergency use authorization, recognizing that a vaccine offering this level of protection could still save lives and reduce hospitalizations.
However, the 50% threshold is not a one-size-fits-all standard. Context matters—the severity of the disease, the availability of alternative treatments, and the urgency of the public health crisis all influence what efficacy rate is deemed sufficient. For example, seasonal flu vaccines typically have efficacy rates between 40% and 60%, yet they are widely used because influenza, while serious, is manageable with antivirals and supportive care. In contrast, vaccines for life-threatening diseases like measles require much higher efficacy rates, often exceeding 90%, to ensure robust herd immunity and prevent outbreaks.
Setting efficacy thresholds also involves balancing risks and benefits. A vaccine with 70% efficacy might be approved if the disease it prevents is highly contagious and deadly, even if it falls short of the ideal 90% mark. For example, the Ebola vaccine Ervebo received approval with an efficacy rate of around 97.5% in clinical trials, but such high efficacy is rare and not always necessary. Public health officials must weigh the potential impact of a vaccine against the urgency of deployment, especially during pandemics.
Practical considerations further complicate the picture. Vaccines must be effective across diverse populations, including vulnerable groups like the elderly or immunocompromised individuals. For instance, COVID-19 vaccines initially showed lower efficacy in older adults, prompting booster doses to enhance protection. Additionally, real-world efficacy often differs from clinical trial results due to factors like variant evolution and adherence to dosing schedules. A vaccine with 80% efficacy in trials might drop to 60% in the field, underscoring the need for ongoing monitoring and adaptive strategies.
Ultimately, the question of what efficacy rate is sufficient hinges on a delicate calculus of science, ethics, and practicality. While higher efficacy is always preferable, the goal of public health is to maximize benefit with available tools. Vaccines with modest efficacy rates can still play a vital role in controlling disease spread, reducing severe outcomes, and buying time for further research and development. As new vaccines emerge, regulators and health officials must remain agile, adjusting thresholds to meet the evolving demands of global health.
People's Bank of America Hours: How Late Are They Open?
You may want to see also
Explore related products






![]()
Factors Affecting Efficacy: Role of variants, immune response, and population demographics in vaccine performance
Vaccine efficacy rates are not set in stone; they are dynamic metrics influenced by a complex interplay of factors. Among these, the emergence of viral variants stands as a formidable challenge. Consider the COVID-19 vaccines: initial trials reported efficacy rates of 95% for the Pfizer-BioNTech and Moderna vaccines against the original strain. However, the Delta variant reduced efficacy against symptomatic infection to approximately 64-88%, while the Omicron variant further diminished protection, particularly against mild cases. This highlights the critical role of viral evolution in shaping vaccine performance, necessitating updated formulations like bivalent boosters to restore efficacy.
Beyond variants, the human immune response plays a pivotal role in determining vaccine efficacy. Age, for instance, is a significant factor; older adults often exhibit weaker immune responses due to immunosenescence. For example, the influenza vaccine is typically 40-60% effective in healthy adults but drops to 17-53% in individuals over 65. To counteract this, high-dose formulations, such as Fluzone High-Dose, containing 4x the antigen (120 µg vs. 30 µg), have been developed to enhance immune stimulation in this demographic. Similarly, underlying health conditions like diabetes or HIV can impair immune function, reducing vaccine efficacy. Tailored dosing strategies and adjuvants are increasingly being explored to optimize responses in these populations.
Population demographics further complicate the efficacy landscape. Socioeconomic factors, such as access to healthcare and vaccine hesitancy, can skew efficacy data. For instance, a vaccine might show lower real-world effectiveness in underserved communities due to delayed second doses or incomplete vaccination series. Geographic location also matters; vaccines may perform differently in regions with distinct co-circulating pathogens or nutritional deficiencies. The rotavirus vaccine, for example, has an efficacy of 98% in high-income countries but drops to 49-77% in low-income settings, likely due to higher rates of malnutrition and gut inflammation.
Practical steps can mitigate these challenges. For individuals, adhering to recommended dosing schedules and staying updated with booster shots is crucial. Healthcare providers should prioritize equitable vaccine distribution and educate communities on the importance of timely vaccination. Policymakers must invest in surveillance systems to monitor variant emergence and adjust vaccine formulations accordingly. By addressing these factors, we can maximize vaccine efficacy and ensure broader protection across diverse populations. The goal is not just to achieve high efficacy rates in trials but to sustain them in the ever-changing real world.
Instant Cash Transfers: How to Send Money Quickly via US Banks
You may want to see also
Explore related products






![]()
Efficacy vs. Severity Reduction: How vaccines may prevent illness, hospitalization, or death despite lower efficacy rates
Vaccine efficacy rates, often spotlighted in clinical trials, measure a vaccine’s ability to prevent disease under ideal conditions. For instance, the Pfizer-BioNTech COVID-19 vaccine demonstrated a 95% efficacy rate in trials, meaning vaccinated individuals were 95% less likely to develop symptomatic COVID-19 compared to the unvaccinated. However, efficacy rates don’t tell the whole story. A vaccine with lower efficacy—say, 60%—can still significantly reduce illness severity, hospitalizations, and deaths, even if it doesn’t prevent infection entirely. This distinction is critical for understanding a vaccine’s real-world impact.
Consider the flu vaccine, which typically has an efficacy rate between 40% and 60%, depending on the season’s dominant strains. While it may not prevent all flu cases, it consistently reduces the risk of severe complications, particularly in high-risk groups like the elderly, pregnant individuals, and those with chronic conditions. For example, a 2018 CDC study found that flu vaccination reduced the risk of ICU admission by 82% among adults. This highlights how vaccines can act as a buffer, transforming a potentially life-threatening illness into a manageable one.
The mechanism behind severity reduction lies in how vaccines train the immune system. Even if a vaccine doesn’t block infection entirely, it primes the body to recognize and respond to the pathogen more efficiently. This rapid immune response can limit viral replication, reduce tissue damage, and prevent the disease from progressing to severe stages. For instance, COVID-19 vaccines have been shown to reduce the risk of hospitalization and death by over 90% in fully vaccinated individuals, despite waning efficacy against infection over time. This underscores the vaccine’s ability to mitigate harm, even when it doesn’t prevent illness altogether.
Practical tips for maximizing a vaccine’s protective benefits include staying up-to-date with booster doses, especially for vaccines like COVID-19 and flu, where immunity wanes over time. For example, a COVID-19 booster increases neutralizing antibodies by 20- to 30-fold, enhancing protection against severe outcomes. Additionally, combining vaccination with non-pharmaceutical interventions—such as masking in crowded spaces and maintaining good hand hygiene—can further reduce the risk of infection and severe disease. Understanding the dual role of vaccines in preventing illness and reducing severity empowers individuals to make informed decisions about their health.
In summary, while efficacy rates are a crucial metric, they don’t capture a vaccine’s full potential to save lives. A vaccine’s ability to reduce severity, hospitalizations, and deaths is a vital measure of its success, particularly in the context of global health. By focusing on both efficacy and severity reduction, we can better appreciate the transformative impact of vaccines on public health, even when their efficacy rates fall short of 100%.
California Banks Embracing Cannabis: Which One is 420 Friendly?
You may want to see also
Frequently asked questions
Efficacy rate refers to the percentage reduction in disease incidence in a vaccinated group compared to an unvaccinated group during clinical trials, under ideal conditions.
Vaccine efficacy is calculated using the formula: (Risk of disease in unvaccinated group - Risk of disease in vaccinated group) / Risk of disease in unvaccinated group, then multiplied by 100 to get a percentage.
No, a 95% efficacy rate means there is a 95% reduction in disease incidence in the vaccinated group compared to the unvaccinated group, not that 5% of vaccinated individuals will get sick.
Efficacy is measured in controlled clinical trials, while effectiveness refers to how well a vaccine performs in real-world settings, accounting for factors like varying populations and conditions.