The varicella vaccine, which protects against chickenpox, is a critical public health tool, but its use during pregnancy requires careful consideration due to potential risks. Since the vaccine contains live attenuated virus, it is generally contraindicated in pregnant individuals to avoid any theoretical risk of transmission to the fetus. However, if a pregnant person is inadvertently vaccinated or exposed to varicella virus, close monitoring is essential. Studies suggest that the vaccine is unlikely to cause harm if administered unknowingly during early pregnancy, but it is still recommended to avoid it throughout gestation. Pregnant individuals who contract chickenpox face serious complications, including severe disease and potential fetal risks such as congenital varicella syndrome, underscoring the importance of vaccination before pregnancy or postpartum. Always consult healthcare providers for personalized advice regarding vaccination and pregnancy.
Explore related products






What You'll Learn
![]()
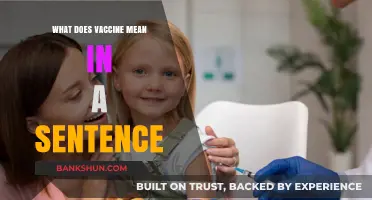
Safety of varicella vaccine during pregnancy
The varicella vaccine, commonly known as the chickenpox vaccine, is a live-attenuated virus vaccine that has been widely used to prevent chickenpox (varicella) in children and adults. However, its administration during pregnancy raises specific safety concerns due to the potential risks associated with live vaccines. Pregnant individuals are generally advised to avoid live vaccines because of theoretical risks to the developing fetus, but understanding the specific implications of the varicella vaccine is crucial for informed decision-making.
From an analytical perspective, the safety profile of the varicella vaccine during pregnancy is primarily based on its classification as a live-attenuated vaccine. Live vaccines carry a theoretical risk of causing infection in the fetus, although no confirmed cases of congenital varicella syndrome or fetal harm have been directly linked to the vaccine. The Centers for Disease Control and Prevention (CDC) and the American College of Obstetricians and Gynecologists (ACOG) recommend avoiding the varicella vaccine during pregnancy due to this theoretical risk. However, accidental vaccination during early pregnancy has not been shown to cause adverse fetal outcomes in reported cases, providing some reassurance.
Instructively, if a pregnant individual is inadvertently vaccinated with the varicella vaccine, specific steps should be followed. First, the pregnancy should be confirmed, and the gestational age noted. While there is no evidence of harm, monitoring the pregnancy closely is advised. Varicella-zoster immune globulin (VZIG) is not recommended post-vaccination, as the risk of fetal infection is considered extremely low. Pregnant individuals should also be counseled to avoid conception for at least 1 month after receiving the vaccine, as per CDC guidelines.
Persuasively, the risks of natural varicella infection during pregnancy far outweigh the theoretical risks of the vaccine. Chickenpox during pregnancy can lead to severe complications, including pneumonia in the mother and congenital varicella syndrome in the fetus, characterized by skin scarring, limb abnormalities, and neurological issues. While the vaccine is contraindicated during pregnancy, ensuring immunity through vaccination before pregnancy is a critical preventive measure. Non-immune individuals should receive two doses of the varicella vaccine, with a minimum interval of 4 weeks between doses, at least 1 month before conception.
Comparatively, the varicella vaccine’s safety during pregnancy contrasts with its proven benefits in non-pregnant populations. For example, the vaccine has a 97% efficacy rate in preventing severe chickenpox in healthy children and adults. This high efficacy underscores the importance of vaccination in eligible individuals, particularly women of childbearing age. By achieving immunity before pregnancy, the risks associated with both the vaccine and natural infection during pregnancy can be effectively mitigated.
Practically, healthcare providers play a key role in assessing varicella immunity in women planning pregnancy. Immunity can be confirmed through medical records of vaccination (two doses) or a blood test (varicella IgG antibody). If immunity is absent, vaccination should be prioritized, ensuring completion at least 1 month before conception. For those already pregnant and non-immune, the focus shifts to prevention of exposure to varicella and prompt treatment with VZIG and antiviral medications if exposure occurs. This proactive approach ensures the safety of both mother and fetus while addressing the unique challenges of varicella prevention during pregnancy.
Understanding the Critical Phases of Vaccine Development and Approval
You may want to see also
Explore related products






![]()
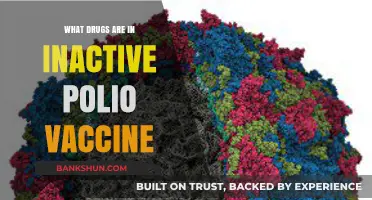
Risks of chickenpox in pregnant women
Chickenpox during pregnancy poses significant risks to both the mother and the developing fetus, making it a critical concern for expectant women and healthcare providers alike. The varicella-zoster virus, which causes chickenpox, can lead to severe complications, particularly if contracted during the first or second trimester. One of the most alarming risks is the potential for congenital varicella syndrome (CVS), a rare but serious condition affecting the fetus. CVS can result in a range of birth defects, including skin scarring, limb abnormalities, eye damage, and neurological issues. The risk of CVS is highest when chickenpox occurs during weeks 13 to 20 of pregnancy, with an estimated occurrence rate of 0.4% to 2% of cases.
For pregnant women, the dangers extend beyond fetal complications. Chickenpox in adulthood often presents more severely than in childhood, increasing the likelihood of pneumonia, a life-threatening complication. Pregnant women with varicella are also at higher risk of developing varicella pneumonia, which has a mortality rate of up to 40% if untreated. Symptoms such as high fever, cough, and difficulty breathing require immediate medical attention. Additionally, secondary bacterial infections, such as skin infections, can further complicate the illness, necessitating prompt antibiotic treatment.
Preventing chickenpox during pregnancy is paramount, and the varicella vaccine plays a crucial role in this effort. However, the vaccine itself is contraindicated in pregnant women due to its live attenuated nature, which could theoretically pose a risk to the fetus. Instead, prevention relies on immunity status assessment early in pregnancy. Women who are non-immune should avoid exposure to chickenpox and consider vaccination postpartum. For those exposed during pregnancy, varicella-zoster immune globulin (VZIG) can be administered within 96 hours to reduce symptom severity, though it does not eliminate all risks.
Practical steps for pregnant women include avoiding contact with individuals who have chickenpox or shingles, as the latter can also transmit the varicella-zoster virus. If exposure occurs, immediate consultation with a healthcare provider is essential. Monitoring for symptoms and early intervention are key to managing potential complications. While the risks are substantial, awareness and proactive measures can significantly mitigate the dangers of chickenpox during pregnancy, safeguarding both maternal and fetal health.
Starting a Bank: Essential Steps to Obtain Your ABA Routing Number
You may want to see also
Explore related products






![]()
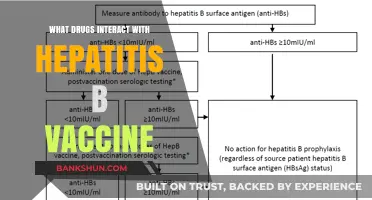
Vaccine timing and pregnancy stages
The varicella vaccine, designed to protect against chickenpox, is a live-attenuated virus vaccine, which raises specific considerations for its administration during pregnancy. Its timing is critical, as the vaccine’s interaction with fetal development varies by trimester. In the first trimester, the vaccine is generally contraindicated due to theoretical risks associated with live vaccines, though no definitive evidence of harm exists. The second trimester is considered safer, though still not recommended unless the benefits outweigh the risks. The third trimester poses the lowest theoretical risk, but vaccination is typically deferred until postpartum to avoid any potential complications. Understanding these distinctions ensures informed decision-making for both maternal and fetal health.
From an analytical perspective, the timing of varicella vaccination during pregnancy hinges on balancing risk and necessity. Pregnant individuals without immunity to chickenpox face severe complications, including pneumonia and congenital varicella syndrome, which can cause fetal abnormalities. However, the vaccine’s live nature prompts caution. Studies suggest that if administered inadvertently during early pregnancy, the risk of fetal harm is low but not zero. Postpartum vaccination is the safest option, providing protection before future pregnancies. For those planning pregnancy, vaccination should occur at least one month prior to conception, ensuring immunity without exposure to the live virus during critical developmental stages.
Instructively, healthcare providers should follow clear guidelines when addressing varicella vaccination in pregnancy. First, confirm immunity through medical history or serologic testing. If non-immune, advise against pregnancy-related vaccination but emphasize postpartum immunization. For accidental vaccination during pregnancy, reassure patients that no intervention is needed, as evidence of harm is lacking. Encourage avoidance of pregnancy for 1 month post-vaccination if administered outside of pregnancy. Practical tips include scheduling preconception checkups to assess immunity and discussing risks with obstetricians to align care plans.
Comparatively, the varicella vaccine’s timing contrasts with other vaccines like Tdap or influenza, which are actively recommended during pregnancy. Unlike these inactivated vaccines, the varicella vaccine’s live component necessitates stricter timing considerations. For instance, Tdap is administered in the third trimester to maximize maternal antibody transfer to the fetus, while influenza vaccination is encouraged anytime during pregnancy to protect both mother and newborn. This comparison highlights the unique challenges of live vaccines and underscores the importance of tailored recommendations based on vaccine type and pregnancy stage.
Descriptively, the stages of pregnancy create a dynamic landscape for vaccine timing. The first trimester, marked by organogenesis, is the most vulnerable period for fetal development, making live vaccines a theoretical concern. The second trimester, characterized by rapid growth, offers slightly more flexibility but remains a cautious window. The third trimester, focused on fetal maturation, presents the least risk but is often bypassed in favor of postpartum vaccination. This progression illustrates why vaccine timing must align with the physiological changes of pregnancy, ensuring safety without compromising long-term protection.
Building a Large Battery Bank: Essential Steps for Reliable Energy Storage
You may want to see also
Explore related products






![]()
Potential side effects for mother and fetus
The varicella vaccine, commonly known as the chickenpox vaccine, is generally not recommended for pregnant women due to potential risks. This live-attenuated vaccine contains a weakened form of the varicella-zoster virus, which, while safe for most individuals, poses theoretical concerns during pregnancy. The primary worry is the possibility of the vaccine virus crossing the placenta and affecting the developing fetus, although no confirmed cases of congenital varicella syndrome have been directly linked to the vaccine. However, the precautionary principle guides medical advice, emphasizing avoidance during pregnancy unless the risk of chickenpox outweighs potential vaccine risks.
For the mother, receiving the varicella vaccine during pregnancy could theoretically lead to a mild vaccine-related chickenpox infection. Symptoms might include a localized rash, fever, or malaise, typically appearing 10–21 days post-vaccination. While these effects are generally mild, they can be concerning, especially if mistaken for a natural infection. Pregnant women who inadvertently receive the vaccine are advised to monitor for symptoms and consult their healthcare provider immediately. Importantly, the vaccine does not contain preservatives like thimerosal or adjuvants that could pose additional risks, but its live nature remains the critical factor.
Fetal risks, though unproven, are a significant consideration. The concern stems from the vaccine’s live virus, which could, in theory, affect fetal development. Studies on accidental vaccinations during pregnancy have not shown a clear link to congenital anomalies, but data is limited. The CDC and WHO recommend waiting 4 weeks after vaccination before attempting pregnancy to minimize any hypothetical risk. For women who receive the vaccine during early pregnancy, ultrasound monitoring may be offered, though evidence does not currently support routine intervention.
Practical advice for pregnant women focuses on prevention and education. Avoiding exposure to chickenpox is critical, as natural infection during pregnancy can cause severe complications, including pneumonia in the mother and congenital varicella syndrome in the fetus. Women should verify their immunity status before pregnancy; those non-immune should receive the two-dose vaccine series (0.5 mL subcutaneously, 4–8 weeks apart) and wait 3 months before conceiving. Post-exposure prophylaxis with varicella-zoster immune globulin (VZIG) is an alternative for pregnant women exposed to chickenpox, offering passive immunity without the risks of live vaccination.
In summary, while the varicella vaccine’s side effects in pregnancy are largely theoretical, the precautionary approach dominates clinical guidance. Mothers may experience mild vaccine-related symptoms, while fetal risks remain unproven but cannot be entirely dismissed. Prioritizing pre-pregnancy vaccination and avoiding exposure during pregnancy are the most effective strategies. For those accidentally vaccinated or exposed, prompt medical consultation and monitoring are essential to ensure the best possible outcomes for both mother and fetus.
Webster Bank in Florida: Locations, Services, and Availability Explained
You may want to see also
Explore related products






![]()
Post-exposure prophylaxis options for pregnant women
Pregnant women exposed to varicella-zoster virus (VZV), the cause of chickenpox, face unique risks due to potential complications for both mother and fetus. Post-exposure prophylaxis (PEP) is critical in these cases to mitigate severe outcomes. The primary options include varicella-zoster immune globulin (VZIG) and antiviral therapy, each with specific indications and limitations. VZIG, derived from pooled human plasma with high titers of anti-VZV antibodies, is the preferred choice for susceptible pregnant women exposed to chickenpox. It must be administered within 96 hours of exposure, ideally within 48 hours, to maximize efficacy. The standard dose is 125 units for susceptible adults, administered intramuscularly. However, VZIG is not always readily available, and its use is reserved for high-risk exposures, such as household or prolonged contact with an infected individual.
Antiviral therapy with acyclovir or its prodrug valacyclovir is an alternative PEP option, particularly when VZIG is unavailable or contraindicated. Acyclovir, given orally at 800 mg five times daily for 7–10 days, or valacyclovir at 1 g three times daily, can reduce the severity and duration of varicella if initiated within 24 hours of rash onset. While data on fetal safety are limited, acyclovir is classified as pregnancy category B, indicating no evidence of risk in animal studies. However, it is generally reserved for severe exposures or when VZIG cannot be used, as its efficacy in preventing congenital varicella syndrome is less established compared to VZIG. Pregnant women should consult their healthcare provider immediately after exposure to determine the most appropriate PEP strategy.
A comparative analysis of VZIG and antiviral therapy highlights their distinct roles in PEP. VZIG acts passively by providing immediate antibodies, offering a direct defense against VZV replication. Its efficacy is well-documented, particularly in preventing severe maternal disease and congenital varicella syndrome. In contrast, antiviral therapy works by inhibiting viral replication but relies on the body’s immune response to clear the infection. While antivirals are more accessible and easier to administer, their effectiveness in PEP is secondary to VZIG. The choice between the two depends on factors such as timing of exposure, availability of VZIG, and the severity of potential outcomes.
Practical considerations for pregnant women include prompt assessment of exposure risk and immune status. Susceptibility to VZV can be determined through medical history or serologic testing, though delays in testing may necessitate presumptive treatment. Women should avoid contact with individuals infected with chickenpox or shingles and notify healthcare providers immediately if exposure occurs. Additionally, pregnant women should be counseled on the signs and symptoms of varicella, such as fever and rash, to seek timely medical intervention. While PEP options exist, prevention through vaccination before pregnancy remains the most effective strategy, as live varicella vaccine is contraindicated during pregnancy.
In conclusion, post-exposure prophylaxis for pregnant women exposed to VZV is a critical intervention to prevent severe complications. VZIG is the first-line option for susceptible individuals, provided it is administered within the narrow window of 96 hours post-exposure. Antiviral therapy serves as a secondary option, particularly in resource-limited settings or when VZIG is unavailable. Timely assessment, accurate risk stratification, and immediate consultation with healthcare providers are essential to optimize outcomes. While PEP is effective, it underscores the importance of pre-pregnancy vaccination and awareness of varicella risks during pregnancy.
Easy Steps to Schedule Your J&J Vaccine Appointment Today
You may want to see also
Frequently asked questions
The varicella vaccine (chickenpox vaccine) is not recommended during pregnancy because it is a live attenuated virus vaccine, which could pose a theoretical risk to the fetus. Pregnant individuals should avoid the vaccine and wait until after delivery to receive it.
If you receive the varicella vaccine and then find out you are pregnant, there is no evidence that the vaccine causes harm to the fetus. However, it is recommended to avoid pregnancy for 1 month after vaccination. Consult your healthcare provider for further guidance.
Yes, but it is advised to wait 1 month after receiving the varicella vaccine before trying to conceive. This precaution ensures there is no theoretical risk to the pregnancy, as the vaccine contains live attenuated virus.





![International Certificate of Vaccination with Vinyl Document Holder - World Health Organization Bilingual Version [cards] World Health Organization [Jan 01, 2007]](https://m.media-amazon.com/images/I/61SHjBP1VYL._AC_UL320_.jpg)