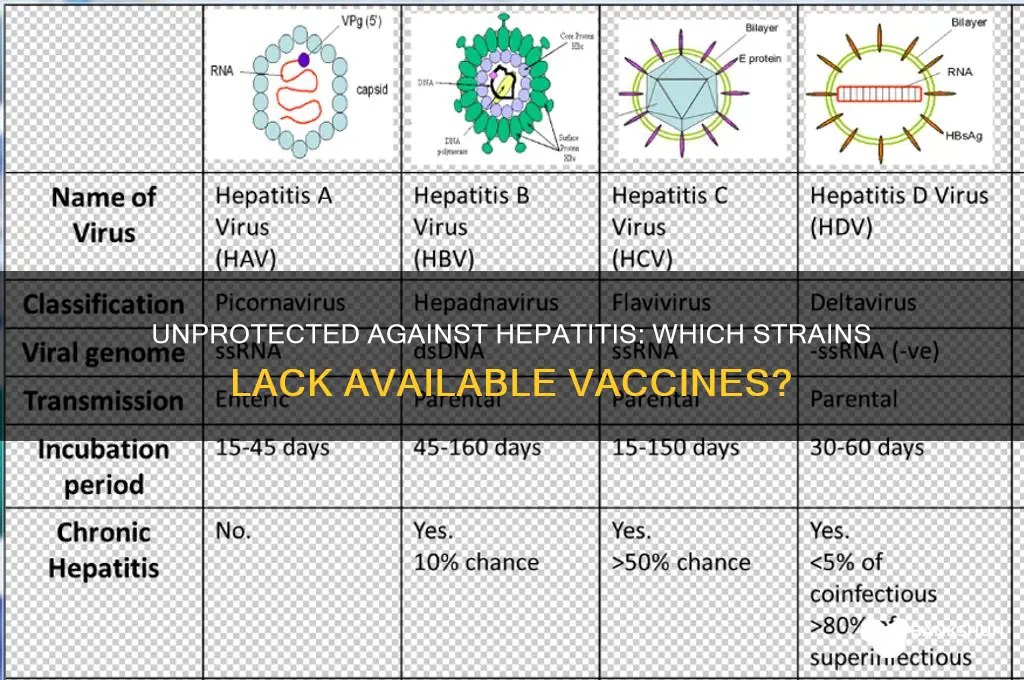
Hepatitis, an inflammation of the liver, is caused by various factors including viruses, toxins, and autoimmune conditions. Among the viral forms, Hepatitis A, B, and D have available vaccines, offering protection against these specific strains. However, Hepatitis C and E currently have no approved vaccines, despite ongoing research efforts. Hepatitis C, in particular, is a significant global health concern due to its potential to cause chronic liver disease, cirrhosis, and liver cancer. The absence of a vaccine for Hepatitis C underscores the importance of prevention through safe practices, early detection, and antiviral treatments to manage the infection effectively.
Explore related products






What You'll Learn
- Hepatitis A: Vaccine available, highly effective, prevents infection, essential for travelers, recommended for at-risk groups
- Hepatitis B: Vaccine exists, prevents chronic infection, reduces liver cancer risk, administered in multiple doses
- Hepatitis C: No vaccine available, transmitted via blood, treated with antivirals, screening is crucial
- Hepatitis D: No vaccine, depends on Hepatitis B, occurs as co-infection, causes severe liver disease
- Hepatitis E: No vaccine in most countries, self-limiting, severe in pregnant women, transmitted via contaminated water
![]()
Hepatitis A: Vaccine available, highly effective, prevents infection, essential for travelers, recommended for at-risk groups
Hepatitis A stands out as a preventable liver infection, thanks to a highly effective vaccine that has been a game-changer in public health. Unlike other forms of hepatitis, such as Hepatitis B, C, D, and E, which either have limited vaccine options or none at all, Hepatitis A offers a clear path to protection. The vaccine is administered in two doses, typically 6 to 18 months apart, and provides long-term immunity, often lasting a lifetime. This makes it a cornerstone of prevention strategies, particularly for those at higher risk of exposure.
For travelers, the Hepatitis A vaccine is not just recommended—it’s essential. The virus is commonly transmitted through contaminated food and water, making it a significant risk in regions with poor sanitation. Countries in Africa, Asia, Central and South America, and Eastern Europe are particularly high-risk areas. Travelers should receive the first dose at least two weeks before departure to ensure partial protection, with the second dose completing the series for long-term immunity. Even last-minute travelers can benefit, as a single dose provides immediate, though temporary, protection.
At-risk groups within the general population also stand to gain significantly from this vaccine. These include individuals with chronic liver disease, men who have sex with men, people who use drugs (both injection and non-injection), and those experiencing homelessness. For children, the Centers for Disease Control and Prevention (CDC) recommends the first dose at age 12–23 months, but it can be administered as early as 6 months for those traveling to high-risk areas. Adults who were not vaccinated as children should also consider getting the vaccine, especially if they fall into any of the high-risk categories.
The vaccine’s effectiveness is well-documented, with studies showing nearly 100% protection against Hepatitis A after the full series. Side effects are generally mild, such as soreness at the injection site or a low-grade fever, and serious reactions are extremely rare. This safety profile, combined with its efficacy, underscores its importance as a public health tool. By preventing infection, the vaccine not only protects individuals but also reduces the spread of the virus within communities.
In practical terms, getting vaccinated is a straightforward process. Most pharmacies and healthcare providers offer the vaccine, and it’s often covered by insurance plans. For those without insurance, public health clinics may provide it at a reduced cost. It’s a small step that yields significant benefits, particularly for those planning international travel or belonging to at-risk groups. In a world where many hepatitis forms remain vaccine-elusive, Hepatitis A serves as a reminder of the power of prevention when a vaccine is available.
Choosing the Perfect Vintage PO Box Bank: A Collector's Guide
You may want to see also
Explore related products





![]()
Hepatitis B: Vaccine exists, prevents chronic infection, reduces liver cancer risk, administered in multiple doses
Hepatitis B stands apart from other forms of hepatitis because a highly effective vaccine exists, offering robust protection against chronic infection and its severe complications. Unlike hepatitis C, D, and E, which lack vaccines, hepatitis B can be prevented through a series of inoculations that stimulate the immune system to produce protective antibodies. This vaccine is a cornerstone of public health, significantly reducing the global burden of liver disease and cancer.
Administered in multiple doses, the hepatitis B vaccine is typically given in a series of three shots over six months. The standard schedule includes an initial dose, followed by a second dose one month later, and a third dose five months after the second. For infants, the vaccine is often given at birth, with subsequent doses at one and six months of age. Adults and adolescents may follow a similar schedule, though accelerated options are available in certain situations. It’s crucial to complete the full series, as partial vaccination may not provide adequate immunity.
One of the vaccine’s most significant benefits is its ability to prevent chronic hepatitis B infection, which occurs when the virus persists in the body long-term. Chronic infection is a leading cause of cirrhosis and liver cancer, making the vaccine a powerful tool in reducing these life-threatening conditions. Studies show that the vaccine is 95% effective in preventing infection and its chronic consequences when administered correctly. This makes it a critical intervention for high-risk groups, including healthcare workers, individuals with multiple sexual partners, and those living in regions with high hepatitis B prevalence.
Practical tips for ensuring successful vaccination include scheduling reminders for follow-up doses, as adherence is key to efficacy. Side effects are generally mild, such as soreness at the injection site or low-grade fever, and rarely interfere with daily activities. For travelers to endemic areas, verifying vaccination status and completing the series before departure is essential. Additionally, combining the hepatitis B vaccine with other immunizations, such as hepatitis A, can streamline protection against multiple liver diseases.
In contrast to hepatitis forms without vaccines, hepatitis B’s preventable nature underscores the importance of global vaccination efforts. While hepatitis C relies on costly antiviral treatments and hepatitis D requires prior hepatitis B infection for prevention, hepatitis B’s vaccine offers a straightforward, cost-effective solution. By prioritizing vaccination, individuals and communities can dramatically reduce the risk of chronic liver disease and cancer, highlighting the vaccine’s role as a public health triumph.
Is Bank of Scotland Reliable? A Comprehensive Review of Its Services
You may want to see also
Explore related products






![]()
Hepatitis C: No vaccine available, transmitted via blood, treated with antivirals, screening is crucial
Hepatitis C stands out among the hepatitis viruses because, unlike Hepatitis A and B, there is no vaccine to prevent it. This virus, primarily transmitted through blood-to-blood contact, poses a significant health risk, especially for those unaware of their exposure. While advancements in antiviral treatments have transformed Hepatitis C from a chronic condition to a curable one, the absence of a vaccine underscores the critical importance of prevention and early detection.
Understanding the transmission routes of Hepatitis C is key to avoiding infection. The virus spreads through contact with infected blood, most commonly through sharing needles or other drug paraphernalia. Less frequently, it can be transmitted through sexual contact, particularly among individuals with multiple partners or those engaging in high-risk behaviors. Healthcare workers are also at risk due to accidental needle sticks. Unlike Hepatitis A, which is often foodborne, or Hepatitis B, which can spread through bodily fluids, Hepatitis C’s reliance on blood contact narrows its transmission but heightens its risk in specific contexts.
Treatment for Hepatitis C has seen remarkable progress with the development of direct-acting antiviral (DAA) medications. These drugs, taken orally for 8 to 12 weeks, cure over 95% of cases, often with minimal side effects. Common DAAs include sofosbuvir/ledipasvir (Harvoni), glecaprevir/pibrentasvir (Mavyret), and daclatasvir (Daklinza). The simplicity of the regimen—typically one pill daily—makes adherence manageable for most patients. However, access to these medications remains a challenge in some regions due to cost and healthcare infrastructure limitations.
Screening for Hepatitis C is crucial because the virus often presents no symptoms in its early stages, allowing it to silently damage the liver over years or decades. The CDC recommends screening for all adults at least once and for all pregnant women during each pregnancy. High-risk individuals, including those born between 1945 and 1965, people with a history of injection drug use, and recipients of blood transfusions before 1992, should be tested regularly. A simple blood test checks for antibodies to the virus, followed by a confirmatory RNA test if positive.
Without a vaccine, prevention hinges on behavioral changes and public health initiatives. Harm reduction programs, such as needle exchange services, play a vital role in curbing transmission among people who use drugs. Educating at-risk populations about safe practices, such as using sterile equipment and avoiding sharing personal items like razors or toothbrushes, is equally important. For healthcare settings, strict adherence to infection control protocols minimizes occupational exposure. While a Hepatitis C vaccine remains elusive, combining treatment advancements with proactive screening and prevention strategies offers the best defense against this persistent virus.
Umb Bank vs. UBS: Unraveling the Differences and Similarities
You may want to see also
Explore related products






![]()
Hepatitis D: No vaccine, depends on Hepatitis B, occurs as co-infection, causes severe liver disease
Hepatitis D, a lesser-known but formidable virus, stands out as the only form of hepatitis with no vaccine. Unlike its counterparts, Hepatitis A, B, and C, which have preventive vaccines or cures, Hepatitis D remains a silent threat, lurking in the shadow of Hepatitis B. This virus cannot exist independently; it requires the presence of Hepatitis B to replicate and cause infection. This unique dependency makes it both a co-infection and a superinfection, significantly complicating its management and prevention.
To understand the gravity of Hepatitis D, consider its impact on the liver. When Hepatitis D co-infects with Hepatitis B, the risk of severe liver disease escalates dramatically. Studies show that individuals with both viruses are more likely to develop cirrhosis, liver failure, or hepatocellular carcinoma compared to those with Hepatitis B alone. The synergy between these viruses creates a perfect storm, accelerating liver damage at an alarming rate. For instance, chronic Hepatitis D infection can lead to cirrhosis in 70–80% of cases within 5–10 years, a stark contrast to the 15–30% cirrhosis rate in chronic Hepatitis B alone.
Preventing Hepatitis D hinges on one critical factor: avoiding Hepatitis B infection. Since Hepatitis D relies on Hepatitis B to thrive, vaccination against Hepatitis B is the most effective preventive measure. The Hepatitis B vaccine, typically administered in a series of three doses over 6 months, provides robust protection. For adults, the standard dosage is 20 micrograms per injection, while children receive age-appropriate lower doses. High-risk groups, such as healthcare workers, intravenous drug users, and individuals with multiple sexual partners, should prioritize vaccination. However, if Hepatitis B infection occurs, the risk of Hepatitis D remains a looming danger.
Managing Hepatitis D is challenging due to its resistance to conventional antiviral treatments. Pegylated interferon-alpha is the only approved therapy, but its efficacy is limited, with only 25–30% of patients achieving sustained virological response. Treatment often spans 48 weeks, requiring careful monitoring for side effects like depression, flu-like symptoms, and hematologic abnormalities. For those with advanced liver disease, liver transplantation may be the last resort, though recurrence of Hepatitis D post-transplant is a significant concern. Practical tips for patients include adhering strictly to treatment regimens, avoiding alcohol, and maintaining a liver-friendly diet rich in fruits, vegetables, and lean proteins.
In conclusion, Hepatitis D’s lack of a vaccine and its dependence on Hepatitis B underscore the urgency of global Hepatitis B vaccination efforts. While treatment options are limited, prevention remains the cornerstone of combating this severe form of liver disease. Awareness, vaccination, and early detection of Hepatitis B are critical steps in halting the spread of Hepatitis D and mitigating its devastating effects on liver health.
Step-by-Step Guide to Applying for a Bank Teller Position
You may want to see also
Explore related products




![]()
Hepatitis E: No vaccine in most countries, self-limiting, severe in pregnant women, transmitted via contaminated water
Hepatitis E stands out among viral hepatitis types because, despite its global presence, most countries lack access to a vaccine. This contrasts sharply with Hepatitis A and B, where vaccines are widely available and recommended. The absence of a universally accessible Hepatitis E vaccine leaves populations vulnerable, particularly in regions with poor water sanitation, where the virus thrives.
Consider the transmission route: contaminated water. Unlike Hepatitis B and C, which spread through blood or bodily fluids, Hepatitis E is primarily waterborne. This makes it a silent threat in areas with inadequate sanitation or during outbreaks linked to contaminated water sources. Travelers to endemic regions, such as parts of Asia, Africa, and Central America, face heightened risk, especially if they consume untreated water or undercooked meat, particularly pork.
While Hepatitis E is typically self-limiting, meaning most healthy individuals recover without treatment within 4–6 weeks, it poses a severe risk to pregnant women. Studies show that infection during pregnancy, especially in the second or third trimester, can lead to acute liver failure, fetal loss, or maternal mortality rates as high as 20–25%. This stark disparity highlights the need for targeted prevention strategies in at-risk populations.
Practical prevention hinges on water safety. Travelers and residents in endemic areas should prioritize drinking bottled or boiled water, avoid raw or undercooked meat, and practice rigorous hand hygiene. For pregnant women in high-risk regions, healthcare providers should emphasize these measures and monitor closely for symptoms like jaundice, fatigue, or abdominal pain. While a vaccine exists in China and has been approved in the EU, its limited availability underscores the urgency for global health initiatives to address this gap.
In summary, Hepatitis E’s lack of widespread vaccination, coupled with its severe impact on pregnant women, demands attention. Until vaccines become globally accessible, prevention through water safety and hygiene remains the cornerstone of protection. Understanding this unique profile—self-limiting yet potentially devastating—is critical for mitigating its impact, especially in vulnerable populations.
Easy Steps to Access Kotak 811 Net Banking Login Securely
You may want to see also
Frequently asked questions
Hepatitis E is the most common form of hepatitis with no widely available vaccine, though a vaccine exists in some countries like China.
No, there is currently no vaccine for hepatitis C, though research is ongoing to develop one.
Hepatitis A does have a vaccine, so it is not the form of hepatitis with no vaccine.
Yes, hepatitis D (Delta hepatitis) has no vaccine, and it requires the presence of hepatitis B to cause infection.