When a vaccine is administered, typically via intramuscular or subcutaneous injection, there is a rare but possible risk of the needle inadvertently hitting a nerve. This occurrence can lead to immediate pain, numbness, tingling, or weakness in the affected area, a condition known as nerve injury. While most cases resolve on their own with time, severe or persistent symptoms may require medical intervention, including physical therapy, pain management, or, in rare instances, surgical repair. Understanding the potential risks and proper injection techniques is crucial for healthcare providers to minimize the likelihood of nerve damage during vaccination.
Explore related products






What You'll Learn
- Nerve Damage Risks: Potential for nerve injury from improper injection technique or needle placement
- Symptoms of Injury: Pain, numbness, tingling, or weakness at the injection site
- Prevention Methods: Proper training, correct needle angle, and site selection to avoid nerves
- Treatment Options: Physical therapy, medication, or surgery for severe nerve damage cases
- Rarity of Occurrence: Extremely rare, with minimal documented cases in medical literature
![]()
Nerve Damage Risks: Potential for nerve injury from improper injection technique or needle placement
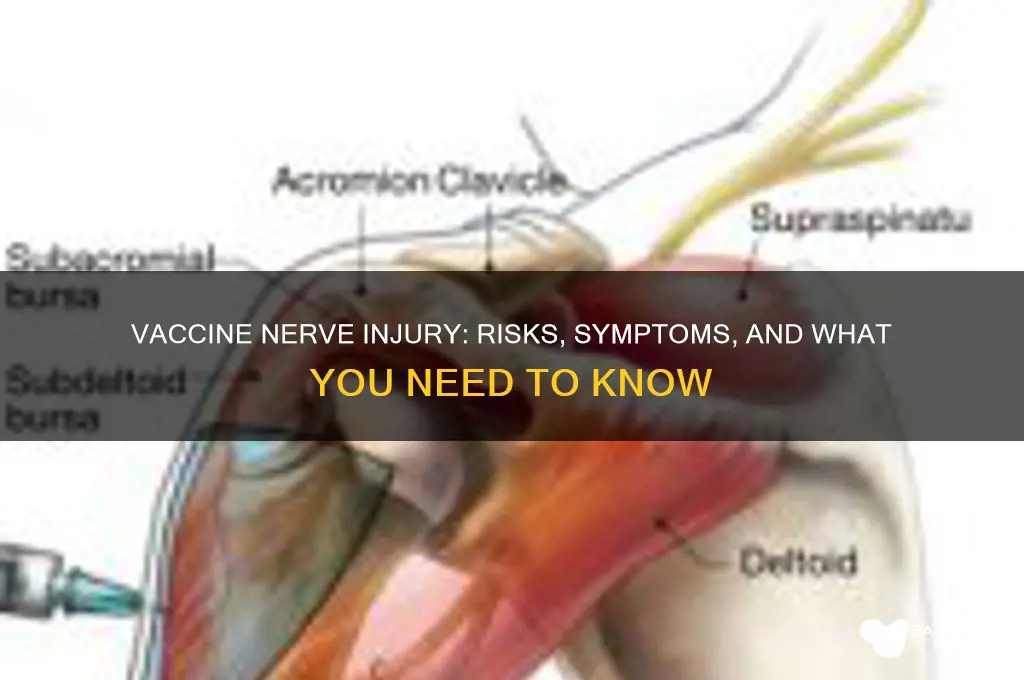
Improper injection technique or incorrect needle placement during vaccination can lead to nerve damage, a rare but serious complication. This risk is particularly associated with intramuscular injections, such as those administered in the deltoid muscle for flu or COVID-19 vaccines. The sciatic nerve, for instance, is vulnerable during injections in the gluteal region, though this site is now generally avoided for vaccinations due to higher risk. Nerve injury can occur if the needle directly traumatizes the nerve or if the injectate (vaccine solution) spreads along nerve pathways, causing inflammation or compression. Understanding the anatomy and adhering to proper injection protocols are critical to minimizing this risk.
To mitigate nerve damage risks, healthcare providers must follow precise guidelines for needle placement and injection technique. For deltoid injections, the needle should be inserted at a 90-degree angle, approximately 1–2 cm below the acromion process, with the arm relaxed. The needle length should be appropriate for the patient’s age and body mass; for adults, a 1-inch (25 mm) needle is typically used, while children and thin adults may require a 5/8-inch (16 mm) needle. Aspiration before injection, though debated, can help ensure the needle is not in a blood vessel, reducing the risk of nerve injury from inadvertent vascular injection. Patients should also be instructed to remain still during the procedure to prevent sudden movements that could alter needle position.
Comparatively, nerve damage from vaccinations is far less common than other injection-related complications, such as pain or swelling at the injection site. However, when it does occur, the consequences can be severe, including persistent pain, numbness, or weakness in the affected limb. For example, radial nerve injury from improper deltoid injections can lead to wrist drop, while sciatic nerve damage from gluteal injections (though rare today) can cause foot drop. These outcomes underscore the importance of training healthcare providers in proper injection techniques and selecting appropriate injection sites based on patient anatomy and vaccine type.
Practically, patients can take steps to reduce their risk of nerve injury during vaccination. Wearing loose-fitting clothing to easily expose the injection site and relaxing the arm or leg during the procedure can help ensure proper needle placement. After vaccination, monitoring for unusual symptoms such as persistent pain, tingling, or loss of function is essential. If these symptoms occur, prompt medical evaluation is necessary to assess for nerve damage and initiate appropriate treatment, which may include physical therapy, pain management, or, in rare cases, surgical intervention. Awareness and proactive measures by both providers and patients are key to preventing this avoidable complication.
How to Register ASBA in Union Bank: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Symptoms of Injury: Pain, numbness, tingling, or weakness at the injection site
Vaccine administration, when it inadvertently affects a nerve, can lead to localized symptoms that are both immediate and concerning. Pain at the injection site is often the first indicator, described as sharp or burning, and may radiate along the nerve pathway. This occurs because nerves are highly sensitive structures, and even slight trauma from a needle can trigger nociceptors—specialized nerve endings that detect tissue damage. For instance, in deltoid injections, hitting the radial or axillary nerve can cause pain extending down the arm, sometimes mistaken for a muscle strain. Recognizing this distinction is crucial, as nerve-related pain typically follows a specific dermatome pattern rather than generalized soreness.
Numbness and tingling, often referred to as paresthesia, are hallmark symptoms of nerve involvement. These sensations arise when the nerve’s ability to transmit signals is disrupted, either due to direct injury or inflammation. For example, a sciatic nerve injury from a poorly placed gluteal injection can result in numbness or "pins and needles" in the leg, foot, or toes. Such symptoms may appear minutes to hours after vaccination and can persist for days or weeks, depending on the severity of the injury. Patients often describe it as a "foot falling asleep," which, while alarming, is usually temporary if addressed promptly.
Weakness at the injection site or in the affected limb is a more severe symptom, indicating potential nerve damage. This occurs when motor nerves, responsible for muscle control, are compromised. For instance, damage to the brachial plexus from an improperly administered shoulder injection can lead to difficulty lifting the arm or gripping objects. Unlike pain or paresthesia, weakness suggests a deeper level of impairment and warrants immediate medical attention. Physical therapy or nerve conduction studies may be recommended to assess the extent of the damage and guide recovery.
To minimize the risk of nerve injury, healthcare providers adhere to specific guidelines, such as using the correct needle length and angle for the patient’s age and body mass index. For adults, a 1-inch needle is typically used for deltoid injections, while children may require shorter needles to avoid deeper tissue penetration. Aspirating before injecting can also confirm the needle is not in a blood vessel, reducing the risk of nerve compression from hematoma formation. Patients experiencing persistent or worsening symptoms should seek evaluation, as early intervention—such as corticosteroids for inflammation or nerve blocks for pain—can significantly improve outcomes.
Woodforest Bank ATM Fee-Free Options: Where to Withdraw Cash Free
You may want to see also
Explore related products




$219.99


![]()
Prevention Methods: Proper training, correct needle angle, and site selection to avoid nerves
Injecting a vaccine into a nerve can cause immediate pain, nerve damage, or prolonged neurological symptoms, making prevention critical. Proper training is the cornerstone of avoiding such incidents. Healthcare providers must understand the anatomy of injection sites, such as the deltoid muscle for most adults, where nerves like the axillary or radial nerves lie nearby. Training should include hands-on practice with anatomical models or simulations to ensure precision. For instance, the CDC recommends a 90-degree needle angle for intramuscular injections in adults, but this may vary for children or specific vaccines. Without adequate training, even experienced providers risk misjudging depth or location, increasing the likelihood of nerve injury.
The correct needle angle is equally vital to minimize nerve damage. For adults receiving vaccines like the flu shot or COVID-19 vaccine, a 90-degree angle ensures the needle penetrates the muscle without reaching deeper tissues where nerves are more exposed. However, for infants and young children, a 45-degree angle is often used due to less muscle mass. Deviating from these angles can increase the risk of hitting a nerve, particularly in areas like the upper arm or thigh. For example, a needle inserted too deeply in the deltoid region might damage the radial nerve, leading to symptoms like weakness or numbness in the hand. Adhering to recommended angles based on age and injection site is a simple yet effective preventive measure.
Site selection plays a pivotal role in avoiding nerves during vaccination. The deltoid muscle is preferred for adults due to its accessibility and lower risk of nerve injury compared to other sites. However, for individuals with low body mass or atrophied muscles, the anterolateral thigh may be a safer alternative. Vaccinators must also consider the patient’s anatomy and any pre-existing conditions, such as muscle atrophy or previous injuries, that might alter nerve positioning. For children under 3 years, the mid-thigh is often chosen to avoid the smaller, more delicate arm muscles. Proper site selection, combined with knowledge of nerve pathways, significantly reduces the risk of complications, ensuring the vaccine is delivered safely and effectively.
In practice, combining these prevention methods requires vigilance and adaptability. For instance, a healthcare provider administering a 0.5 mL dose of a vaccine to a frail elderly patient might opt for the thigh instead of the arm, using a 45-degree angle to avoid nerves. Similarly, during mass vaccination campaigns, quick assessments of patient anatomy and adherence to guidelines are essential. Practical tips include palpating the injection site to confirm muscle location and using smaller needles for pediatric populations. By prioritizing proper training, precise needle angles, and thoughtful site selection, vaccinators can minimize the risk of nerve injury, ensuring patient safety and maintaining trust in vaccination programs.
Is Your BVN Secure with Kuda Bank? Safety Concerns Explained
You may want to see also
Explore related products






![]()
Treatment Options: Physical therapy, medication, or surgery for severe nerve damage cases
Nerve damage from a vaccine, though rare, can manifest as pain, weakness, or numbness, often due to needle misplacement or individual sensitivity. When symptoms persist or worsen, targeted treatment becomes essential to restore function and alleviate discomfort. The approach—physical therapy, medication, or surgery—depends on the severity and location of the injury, with each option offering distinct benefits and considerations.
Physical therapy stands as the first line of defense for mild to moderate cases. A tailored program may include stretching exercises to improve flexibility, strength training to rebuild muscle support, and manual therapy to reduce scar tissue formation. For instance, a patient with radial nerve injury might perform wrist extensions with a 1-pound weight, gradually increasing to 3 pounds over six weeks. Caution is advised to avoid overexertion, as this can exacerbate inflammation. Consistency is key; daily sessions of 20–30 minutes yield better outcomes than sporadic efforts.
Medication serves as a complementary or primary treatment for managing pain and inflammation. Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen (400–800 mg every 6–8 hours) can reduce swelling, while corticosteroids, such as prednisone (20–60 mg daily for 1–2 weeks), may be prescribed for acute cases. For neuropathic pain, gabapentin (300 mg three times daily, titrated up to 1800 mg) or pregabalin (75–150 mg twice daily) can modulate nerve signals. However, long-term use of these medications requires monitoring for side effects like dizziness or gastrointestinal issues.
Surgery is reserved for severe cases where conservative measures fail, such as when nerve compression or transection is evident. Decompression surgery, for example, involves removing scar tissue or relocating structures pressing on the nerve. In cases of complete nerve division, grafting or nerve transfer may be necessary. Postoperative recovery includes immobilization for 2–4 weeks, followed by physical therapy to retrain nerve pathways. Success rates vary; a 2021 study reported 70% functional recovery in patients undergoing ulnar nerve decompression within six months of injury.
Choosing the right treatment requires a nuanced understanding of the patient’s condition, age, and overall health. While physical therapy and medication offer noninvasive solutions, surgery provides hope for complex injuries. Early intervention, regardless of the method, significantly improves outcomes, underscoring the importance of prompt evaluation and personalized care.
Understanding Republic Bank & Trust: Services, History, and Financial Offerings
You may want to see also
Explore related products






![]()
Rarity of Occurrence: Extremely rare, with minimal documented cases in medical literature
Vaccine administration, when performed correctly, is a safe and routine procedure. However, concerns about potential nerve damage arise from rare instances where the needle may inadvertently penetrate a nerve during injection. These cases are exceptionally uncommon, with medical literature documenting only a handful of occurrences. For example, a review of vaccine-related nerve injuries in the *Journal of Immunology Research* identified fewer than 100 cases globally over several decades, despite billions of doses administered annually. This underscores the rarity of such events, emphasizing that the risk is statistically negligible compared to the vast number of vaccinations given each year.
To contextualize this rarity, consider the precision required for a nerve injury to occur. Most vaccines, such as the influenza or COVID-19 vaccines, are administered intramuscularly into the deltoid muscle of the upper arm. Nerves in this area, like the radial or axillary nerves, are deep beneath the skin and muscle, making accidental contact highly improbable. Proper technique, including correct needle length (typically 1–1.5 inches for adults) and angle (90 degrees for most intramuscular injections), further minimizes risk. Healthcare providers are trained to avoid anatomical landmarks where nerves are more superficial, such as the shoulder or lower arm, reducing the likelihood of injury even further.
From a practical standpoint, individuals can take steps to ensure safe vaccine administration. For instance, informing the healthcare provider of any prior injuries or surgeries in the injection area can help them adjust the technique accordingly. Parents of young children, who may receive vaccines in the thigh muscle, should ensure the provider uses the correct needle size (typically 5/8 inch for infants) to avoid deeper tissue penetration. While these precautions are largely precautionary, they highlight the meticulous care taken to prevent rare complications.
Comparatively, the risks associated with forgoing vaccination far outweigh the minuscule chance of nerve injury. Vaccine-preventable diseases, such as measles or tetanus, can cause severe neurological damage, paralysis, or even death. For example, tetanus toxin directly attacks the nervous system, leading to excruciating muscle spasms and respiratory failure. In contrast, the few documented cases of vaccine-related nerve injuries typically resolve with conservative treatment, such as physical therapy or anti-inflammatory medications. This stark contrast underscores the importance of vaccination as a critical public health measure.
In conclusion, while the idea of a vaccine hitting a nerve may provoke anxiety, the reality is that such events are extraordinarily rare. Medical literature provides minimal evidence of these occurrences, and when they do happen, they are often manageable. By adhering to proper injection techniques and understanding the negligible risk, individuals can approach vaccination with confidence, focusing on its life-saving benefits rather than unfounded fears.
Maximize Your Key Bank Rewards: Easy Steps to Redeem Points
You may want to see also
Frequently asked questions
If a vaccine injection accidentally hits a nerve, it can cause immediate pain, tingling, or numbness at the injection site. This is rare but can occur if the needle comes into direct contact with a nerve. Most symptoms are temporary and resolve on their own within a few hours to days.
While hitting a nerve during vaccination can cause discomfort, long-term damage is extremely rare. Most cases result in temporary symptoms like pain or numbness. If symptoms persist or worsen, it’s important to consult a healthcare provider for evaluation.
Signs that a vaccine injection may have hit a nerve include sharp, shooting pain, tingling, or numbness at the injection site immediately after the shot. These symptoms typically appear right away and can radiate along the affected nerve pathway. If unsure, consult a healthcare professional for assessment.