A cancer vaccine is a type of immunotherapy designed to harness the body's immune system to prevent or treat cancer. Unlike traditional vaccines that protect against infectious diseases, cancer vaccines target specific antigens or proteins unique to cancer cells. These vaccines can be prophylactic, preventing cancers caused by viruses like HPV or hepatitis B, or therapeutic, aimed at treating existing cancers by stimulating the immune system to recognize and destroy tumor cells. Key components of a cancer vaccine often include tumor-associated antigens, adjuvants to enhance immune response, and delivery systems like nanoparticles or viral vectors. By tailoring the immune response to cancer-specific markers, these vaccines offer a promising approach to personalized and targeted cancer therapy.
| Characteristics | Values |
|---|---|
| Type of Vaccine | Therapeutic (aims to treat existing cancer) or prophylactic (prevents cancer) |
| Target Antigens | Tumor-specific antigens (e.g., neoantigens, cancer-testis antigens) or tumor-associated antigens (e.g., HER2, MUC1) |
| Delivery Methods | Viral vectors, mRNA, DNA, peptide-based, dendritic cell vaccines, or protein-based |
| Adjuvants | Added to enhance immune response (e.g., TLR agonists, cytokines like GM-CSF) |
| Immune Mechanism | Activates cytotoxic T cells, natural killer cells, or antibodies to target cancer cells |
| Personalization | Often tailored to individual patient's tumor mutations (e.g., neoantigen vaccines) |
| Administration Route | Intramuscular, subcutaneous, intradermal, or intravenous |
| Combination Therapies | Often used with checkpoint inhibitors, chemotherapy, or radiation for enhanced efficacy |
| Examples | Provenge (sipuleucel-T), mRNA-based vaccines (e.g., BioNTech/Moderna trials), viral vector vaccines (e.g., T-VEC) |
| Challenges | Tumor heterogeneity, immune evasion by cancer cells, and manufacturing complexity |
| Current Research Focus | Improving antigen delivery, enhancing immune response, and reducing side effects |
Explore related products






What You'll Learn
- Antigens: Specific cancer markers targeted by the vaccine to trigger immune response
- Adjuvants: Substances added to enhance vaccine effectiveness and immune activation
- Delivery Systems: Methods like nanoparticles or viral vectors to transport vaccine components
- Personalized Vaccines: Tailored treatments based on individual tumor mutations or neoantigens
- Immune Checkpoint Inhibitors: Combined therapies to boost vaccine-induced immune responses against cancer
![]()
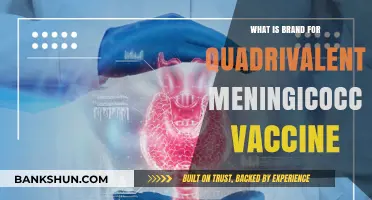
Antigens: Specific cancer markers targeted by the vaccine to trigger immune response
Cancer vaccines rely on antigens—unique markers found on cancer cells—to provoke a targeted immune response. These antigens, often proteins or peptides, act as red flags, signaling the immune system to attack and destroy malignant cells. Unlike traditional vaccines that prevent diseases, cancer vaccines aim to treat existing cancers or prevent recurrence by training the immune system to recognize and eliminate tumor-specific or tumor-associated antigens (TAAs). Examples include human papillomavirus (HPV) antigens in cervical cancer vaccines and mutated KRAS proteins in pancreatic cancer therapies.
Identifying the right antigen is critical for vaccine efficacy. Tumor-specific antigens, like neoantigens arising from somatic mutations, are ideal because they are exclusive to cancer cells, minimizing off-target effects. Tumor-associated antigens, such as HER2/neu in breast cancer, are also targeted but require careful design to avoid harming healthy cells. Advances in genomics and bioinformatics now enable personalized antigen selection, tailoring vaccines to an individual’s tumor mutational profile. For instance, mRNA-based vaccines can encode multiple neoantigens, offering a highly customized approach.
The delivery of antigens to the immune system is equally important. Adjuvants, such as toll-like receptor agonists or cytokines, are often included to enhance immune activation. Dosage and scheduling vary by vaccine type; for example, the Provenge (sipuleucel-T) vaccine for prostate cancer requires three infusions over one month, each prepared from the patient’s own immune cells primed with the antigen prostatic acid phosphatase (PAP). Clinical trials for neoantigen vaccines typically administer 1–3 doses, with immune response monitoring to optimize timing.
Practical considerations include patient selection and combination therapies. Cancer vaccines are most effective in early-stage cancers or minimal residual disease, where the tumor burden is low. Combining vaccines with checkpoint inhibitors, such as pembrolizumab, can amplify immune responses by overcoming tumor-induced suppression. For instance, a melanoma vaccine targeting gp100 showed improved outcomes when paired with ipilimumab. Patients should discuss potential side effects, such as injection site reactions or flu-like symptoms, with their oncologist, as these are generally mild but can impact quality of life.
The future of antigen-based cancer vaccines lies in precision medicine and innovative platforms. mRNA and viral vector technologies, proven in COVID-19 vaccines, are now being adapted for cancer, offering rapid and scalable production. Early-phase trials of personalized neoantigen vaccines report durable responses in up to 40% of patients with advanced cancers. As research progresses, antigen selection will become more refined, leveraging machine learning to predict immunogenicity and prioritize targets. For patients and clinicians, staying informed about emerging trials and FDA approvals is key to accessing these cutting-edge treatments.
Do Banks Dispense Rare $500 Bills?
You may want to see also
Explore related products



$11.93 $21.99



![]()
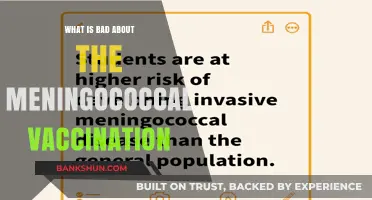
Adjuvants: Substances added to enhance vaccine effectiveness and immune activation
Adjuvants are the unsung heroes of cancer vaccines, acting as catalysts that amplify the immune system's response to tumor-specific antigens. Without them, many vaccines would fail to elicit a robust enough reaction to combat cancer cells effectively. These substances work by mimicking the natural immune triggers that occur during an infection, ensuring the body recognizes the vaccine as a threat worth fighting. For instance, aluminum salts, one of the most common adjuvants, have been used for decades in vaccines like those for hepatitis and HPV, creating a depot effect that slowly releases antigens to prolong immune stimulation. In cancer vaccines, adjuvants like monophosphoryl lipid A (MPL) derived from bacterial cell walls are often employed to stimulate toll-like receptors, which are crucial for initiating immune responses.
Consider the role of adjuvants in personalized cancer vaccines, where precision is paramount. Here, adjuvants like CpG oligodeoxynucleotides (CpG ODN) are paired with neoantigens—unique proteins found on cancer cells. CpG ODN mimics bacterial DNA, triggering dendritic cells to mature and present antigens to T cells more efficiently. Clinical trials have shown that combining CpG ODN with neoantigen vaccines can increase the frequency of tumor-infiltrating lymphocytes by up to 40%, significantly improving patient outcomes. However, the dosage is critical; too little adjuvant may result in insufficient immune activation, while too much can lead to toxicity. For adults, a typical dose of CpG ODN ranges from 1 to 5 mg per injection, administered intramuscularly or intradermally.
Not all adjuvants are created equal, and their selection depends on the vaccine’s mechanism and the patient’s immune status. For example, saponin-based adjuvants like QS-21, derived from the bark of the Chilean soapbark tree, are potent stimulators of both humoral and cellular immunity. They are particularly effective in cancer vaccines targeting solid tumors, where a strong T-cell response is essential. However, their high cost and potential for local reactions, such as pain and swelling, limit their widespread use. In contrast, emulsions like MF59, an oil-in-water adjuvant, are milder and have been used in influenza vaccines for elderly populations, demonstrating safety in immunocompromised individuals. For cancer vaccines, MF59 is often combined with peptide-based antigens to enhance their immunogenicity without overwhelming the immune system.
Practical considerations for adjuvant use in cancer vaccines extend beyond efficacy to include storage, stability, and administration. Adjuvants like alum are stable at room temperature, making them ideal for vaccines distributed in resource-limited settings. Conversely, lipid-based adjuvants like AS01 (used in the shingles vaccine) require cold chain storage to maintain their integrity. Clinicians must also be mindful of patient-specific factors, such as pre-existing autoimmune conditions, which may contraindicate the use of certain adjuvants. For instance, patients with systemic lupus erythematosus should avoid vaccines containing CpG ODN due to the risk of exacerbating autoimmune activity.
In conclusion, adjuvants are not merely additives but strategic components that dictate the success of cancer vaccines. Their selection, dosage, and formulation must be tailored to the vaccine’s target and the patient’s immune landscape. As research advances, novel adjuvants like polymeric nanoparticles and stimulator of interferon genes (STING) agonists are being explored to further enhance vaccine efficacy. By understanding and optimizing adjuvant use, we can unlock the full potential of cancer vaccines, turning them into powerful tools in the fight against this complex disease.
Shared Banking Made Easy: Steps to Open a Joint Bank Account
You may want to see also
Explore related products






![]()
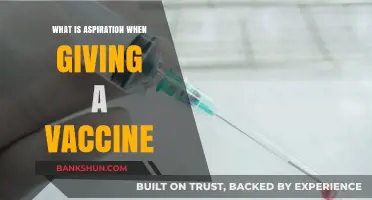
Delivery Systems: Methods like nanoparticles or viral vectors to transport vaccine components
Effective delivery of cancer vaccine components is critical for eliciting a robust immune response against tumor cells. Nanoparticles and viral vectors have emerged as leading methods to transport antigens, adjuvants, and genetic material directly to immune cells, enhancing both safety and efficacy. Nanoparticles, often composed of lipids, polymers, or inorganic materials, encapsulate vaccine components, protecting them from degradation and facilitating targeted release. For instance, lipid nanoparticles, similar to those used in mRNA COVID-19 vaccines, have been adapted for cancer vaccines, enabling precise delivery of mRNA encoding tumor-associated antigens. These nanoparticles can be engineered to accumulate in lymph nodes, where they prime dendritic cells to activate T cells, a key step in anti-tumor immunity.
Viral vectors, on the other hand, leverage the natural ability of viruses to infect cells and deliver genetic material. Modified adenoviruses, lentiviruses, and vaccinia viruses are commonly used to transport genes encoding cancer antigens into immune cells. For example, the TALIMOGEN LAHERPAREVEC (T-VEC), the first FDA-approved viral vector-based cancer vaccine, uses a genetically modified herpes simplex virus to deliver granulocyte-macrophage colony-stimulating factor (GM-CSF) directly into tumors, enhancing immune infiltration and destruction of cancer cells. While viral vectors offer high transduction efficiency, they can provoke immune responses against the vector itself, potentially limiting repeat dosing.
Comparing these systems, nanoparticles offer versatility in cargo type (proteins, mRNA, DNA) and surface modification for targeted delivery, making them suitable for personalized cancer vaccines. Viral vectors, however, excel in delivering genetic material into hard-to-transfect cells, such as dendritic cells, but their immunogenicity and manufacturing complexity pose challenges. For optimal outcomes, the choice of delivery system depends on the vaccine’s mechanism of action, the patient’s immune status, and the tumor microenvironment.
Practical considerations include dosage and administration. Nanoparticle-based vaccines typically require lower antigen doses (e.g., 10–100 µg of mRNA) compared to traditional protein vaccines, as they enhance antigen presentation. Viral vectors, however, often necessitate higher titers (e.g., 10^9–10^11 viral particles) to ensure sufficient transduction. Both systems can be administered intramuscularly, intradermally, or directly into tumors, with the latter showing promise in localized cancers like melanoma. Clinicians must also monitor for adverse reactions, such as injection site inflammation or vector-induced immune responses, and adjust dosing schedules accordingly.
In conclusion, delivery systems like nanoparticles and viral vectors are transformative tools in cancer vaccinology, addressing longstanding challenges in antigen delivery and immune activation. By tailoring these methods to specific cancer types and patient profiles, researchers can maximize the therapeutic potential of vaccines, moving closer to effective immunotherapies for a broader range of malignancies.
Understanding FATCA: What It Means for Global Banking Compliance
You may want to see also
Explore related products






![]()
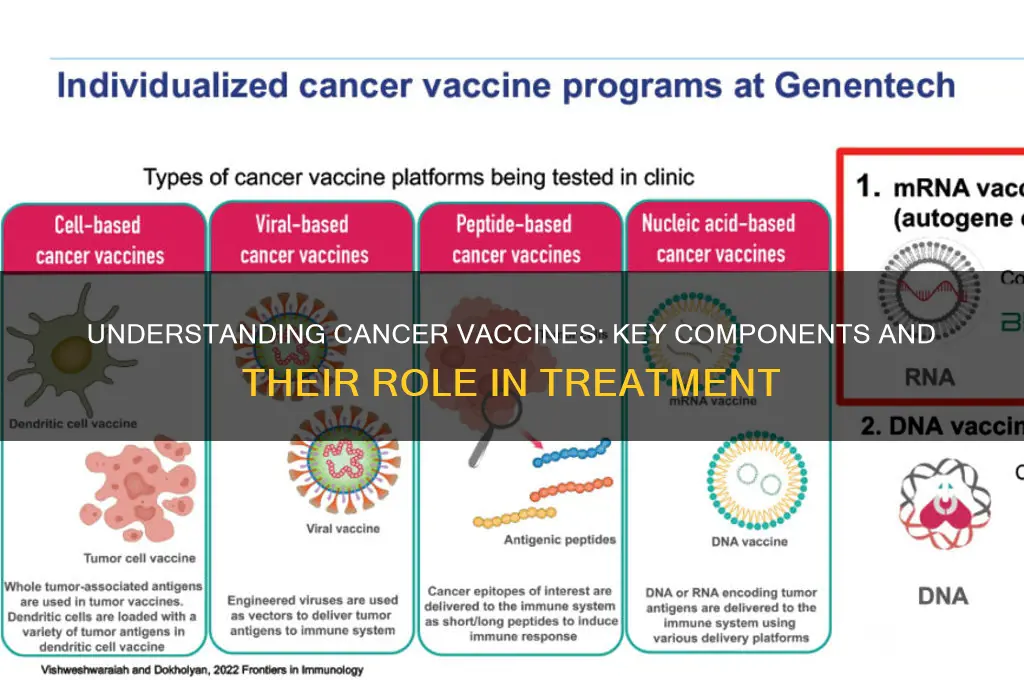
Personalized Vaccines: Tailored treatments based on individual tumor mutations or neoantigens
Cancer vaccines have traditionally aimed at broad immune stimulation, but personalized vaccines represent a paradigm shift by targeting unique tumor mutations, known as neoantigens. These neoantigens arise from genetic alterations specific to an individual’s cancer, making them distinct from normal cells and ideal targets for precise immune attack. Unlike off-the-shelf treatments, personalized vaccines are custom-designed using genomic sequencing of a patient’s tumor and healthy tissue to identify these mutations. This approach ensures the immune system is trained to recognize and destroy cancer cells while sparing healthy ones, minimizing side effects and maximizing efficacy.
Creating a personalized vaccine begins with a biopsy of the tumor, followed by advanced DNA sequencing to map its genetic profile. Bioinformatics tools then predict which neoantigens are most likely to provoke a strong immune response. These selected neoantigens are synthesized into a vaccine, often delivered via mRNA or peptide-based platforms, and administered in a series of doses, typically ranging from 3 to 6 injections over several weeks. Clinical trials have shown that personalized vaccines can induce robust T-cell responses in patients with melanoma, glioblastoma, and other cancers, with some studies reporting durable remissions in up to 30% of cases.
One of the most compelling aspects of personalized vaccines is their adaptability. As tumors evolve and develop resistance, new mutations can be identified and incorporated into updated vaccine formulations, ensuring ongoing relevance of the treatment. However, this approach is not without challenges. The process is time-consuming, requiring 8–12 weeks from biopsy to vaccine production, which may delay treatment for rapidly progressing cancers. Additionally, the cost of genomic sequencing and custom manufacturing remains high, though advancements in technology are gradually reducing expenses.
For patients considering personalized vaccines, it’s essential to understand that eligibility depends on tumor type, mutation burden, and overall health. Melanoma and non-small cell lung cancer patients, for instance, are often ideal candidates due to their high mutation rates. Practical tips include discussing genomic testing with your oncologist early in the treatment journey and exploring clinical trials, as personalized vaccines are not yet widely available outside research settings. While still experimental, this approach holds immense promise, offering a glimpse into a future where cancer treatment is as unique as the individual fighting it.
Banks Near University of Indianapolis: Convenient Financial Options for Students
You may want to see also
Explore related products






![]()
Immune Checkpoint Inhibitors: Combined therapies to boost vaccine-induced immune responses against cancer
Cancer vaccines aim to harness the immune system's power to recognize and destroy cancer cells. However, tumors often employ cunning strategies to evade immune detection, including exploiting immune checkpoint pathways. These pathways, designed to prevent autoimmune reactions, can be hijacked by cancer cells to suppress immune responses. Immune checkpoint inhibitors (ICIs) are a revolutionary class of drugs that counteract this suppression, essentially releasing the brakes on the immune system.
When combined with cancer vaccines, ICIs offer a potent one-two punch. The vaccine primes the immune system by presenting tumor-specific antigens, while ICIs unleash the activated immune cells to attack the cancer with renewed vigor. This combination therapy holds immense promise for enhancing the efficacy of cancer vaccines, particularly in cancers with high mutational burdens, such as melanoma and non-small cell lung cancer.
Consider the example of ipilimumab, a CTLA-4 inhibitor, combined with a gp100 peptide vaccine in advanced melanoma. Clinical trials demonstrated a significant improvement in overall survival compared to ipilimumab alone, highlighting the synergistic effect of this combined approach. Similarly, nivolumab, a PD-1 inhibitor, has shown promising results when paired with personalized neoantigen vaccines in various cancer types.
The optimal sequencing and dosing of ICIs and cancer vaccines remain areas of active research. Some studies suggest administering the vaccine first to prime the immune system, followed by ICI treatment to amplify the response. Others explore concurrent administration for a more synchronized attack. Dosage adjustments are crucial, as combining therapies can increase the risk of immune-related adverse events, such as colitis and pneumonitis. Careful monitoring and management of these side effects are essential for patient safety.
While the potential of combining ICIs with cancer vaccines is undeniable, challenges remain. Patient selection is critical, as not all tumors express the checkpoint molecules targeted by ICIs. Additionally, the high cost of these therapies and the need for personalized vaccine development pose significant hurdles to widespread adoption. Despite these challenges, the future of cancer treatment is undoubtedly moving towards personalized, immunomodulatory approaches, with ICIs playing a pivotal role in boosting vaccine-induced immune responses against cancer.
Annual Bank Stress Test Frequency: How Many Are Conducted Yearly?
You may want to see also
Frequently asked questions
A cancer vaccine is a type of immunotherapy designed to stimulate the body’s immune system to recognize and attack cancer cells. It can be preventive (to prevent certain cancers) or therapeutic (to treat existing cancer).
A cancer vaccine works by introducing antigens (substances found on cancer cells) to the immune system, training it to identify and destroy cancer cells. It may also boost the immune response to better target tumors.
A cancer vaccine often includes antigens (e.g., tumor-specific proteins or peptides), adjuvants (to enhance immune response), and sometimes delivery systems like nanoparticles or viral vectors to improve efficacy.
Eligibility depends on the type of cancer vaccine. Preventive vaccines (e.g., HPV vaccine) are for individuals at risk of certain cancers, while therapeutic vaccines are typically for cancer patients as part of their treatment plan.
While some cancer vaccines (e.g., HPV and hepatitis B vaccines) are widely available for prevention, therapeutic cancer vaccines are still in development and are primarily accessible through clinical trials or specific approvals for certain cancers.