The concept of a bridge to efficacy in the context of pertussis vaccines refers to a regulatory and scientific approach that allows for the approval of new vaccines based on their ability to induce immune responses (immunobridging) rather than solely relying on clinical efficacy trials. Pertussis, commonly known as whooping cough, is a highly contagious respiratory disease caused by *Bordetella pertussis*, and vaccination remains the most effective preventive measure. However, conducting traditional efficacy trials for new pertussis vaccines can be challenging due to ethical and logistical constraints, such as the need for large study populations and the difficulty of exposing participants to the disease. The bridge to efficacy strategy leverages data from established vaccines to demonstrate that a new vaccine produces comparable or superior immune responses, thereby inferring its protective efficacy. This approach accelerates the development and approval of improved pertussis vaccines, ensuring broader access to effective immunization and reducing the global burden of this preventable disease.
| Characteristics | Values |
|---|---|
| Definition | A study design used to infer vaccine efficacy by bridging immunogenicity data from a new vaccine to a licensed vaccine with established clinical efficacy. |
| Purpose | To assess the effectiveness of a new pertussis vaccine without conducting large-scale efficacy trials. |
| Key Component | Immunogenicity (antibody response) as a surrogate marker for protection. |
| Target Disease | Pertussis (Whooping Cough) |
| Vaccine Types | Acellular Pertussis Vaccines (aP) |
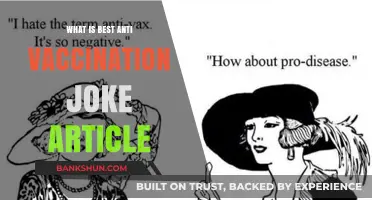
| Surrogate Endpoint | Antibody levels against pertussis antigens (e.g., PT, FHA, PRN, FIM) |
| Regulatory Acceptance | Widely accepted by regulatory agencies (e.g., FDA, EMA) for vaccine approval. |
| Advantages | Reduces need for large, costly efficacy trials; faster vaccine development. |
| Limitations | Relies on correlation between immunogenicity and clinical protection, which may not always be perfect. |
| Correlation Requirement | Strong correlation between antibody titers and clinical protection must be established. |
| Licensed Vaccines Used | Established pertussis vaccines with proven clinical efficacy. |
| Population Focus | Infants, children, adolescents, and adults, depending on vaccine target. |
| Recent Developments | Improved assays for measuring antibody responses; inclusion of additional pertussis antigens. |
| Challenges | Variability in immune responses; need for standardized assays. |
| Global Impact | Facilitates faster introduction of new pertussis vaccines, especially in low-resource settings. |
Explore related products






What You'll Learn
- Vaccine Development History: Evolution of pertussis vaccines from whole-cell to acellular formulations
- Immune Response Mechanisms: How pertussis vaccines stimulate immunity against Bordetella pertussis
- Efficacy in Different Populations: Vaccine effectiveness across age groups, including infants and adults
- Waning Immunity Challenges: Decline in vaccine protection over time and booster recommendations
- Global Vaccination Strategies: Efforts to reduce pertussis incidence through immunization programs
![]()
Vaccine Development History: Evolution of pertussis vaccines from whole-cell to acellular formulations
The pertussis vaccine's journey from whole-cell to acellular formulations is a testament to the iterative nature of medical science, driven by the need to balance efficacy with safety. Whole-cell pertussis (wP) vaccines, introduced in the 1940s, contained inactivated *Bordetella pertussis* bacteria, offering robust immunity but accompanied by fever, pain, and rare neurological events. By the 1990s, acellular pertussis (aP) vaccines emerged, using purified antigens like pertussis toxin and filamentous hemagglutinin. These reduced adverse reactions but required careful antigen selection and higher dosages (e.g., 20–25 µg of pertussis toxoid vs. whole-cell’s bacterial mass) to maintain efficacy. This evolution highlights the trade-offs in vaccine design and the critical role of antigen refinement in modern immunology.
Consider the practical implications for immunization schedules. Whole-cell vaccines were typically administered in a 3-dose primary series starting at 2 months of age, followed by boosters at 12–18 months and 4–6 years. Acellular vaccines, while safer, often require a 5-dose series (2, 4, 6, 15–18 months, and 4–6 years) due to their lower immunogenicity per dose. For adolescents and adults, a reduced antigen dose (e.g., 2.5 µg pertussis toxoid in Tdap) is used to minimize reactogenicity while boosting waning immunity. Clinicians must weigh these schedules against patient age, prior reactions, and local disease prevalence to optimize protection.
A comparative analysis reveals the "bridge to efficacy" concept in pertussis vaccines: how acellular formulations maintain protective immunity despite fewer antigens. Studies show that while wP induces broader immune responses (Th1/Th17 dominance), aP skews toward Th2 responses, correlating with reduced duration of protection. Bridging this gap involves adjuvant innovation (e.g., aluminum salts) and antigen stabilization, ensuring aP vaccines achieve ≥85% efficacy in clinical trials. For instance, the FDA’s 2018 guidance mandates non-inferiority trials for new aP vaccines, benchmarking against licensed products like DTaP-IPV-Hib-HepB.
Persuasively, the shift to acellular vaccines underscores the importance of public trust in vaccine safety. While wP’s adverse event rate (1 in 1,000 for fever >40.5°C) fueled hesitancy in the 1980s, aP’s 1 in 10,000 rate restored confidence, albeit with a resurgence of pertussis in some regions due to suboptimal durability. This paradox demands ongoing research into next-generation vaccines, such as live attenuated nasal sprays or toxoid-only formulations, which could combine safety with mucosal immunity. Policymakers must communicate these trade-offs transparently to sustain vaccination uptake.
In conclusion, the evolution from whole-cell to acellular pertussis vaccines exemplifies the delicate balance between immunogenicity, safety, and practicality. From dosage adjustments to antigen selection, each innovation reflects lessons learned from clinical experience and immunological research. As pertussis remains endemic globally, understanding this history equips healthcare providers and researchers to address current challenges, such as maternal Tdap timing (27–36 weeks’ gestation) or adolescent boosters, ensuring the bridge to efficacy remains sturdy in the face of evolving bacterial strains and immune escape.
2008 Financial Crisis: How Many US Banks Collapsed?
You may want to see also
Explore related products






![]()
Immune Response Mechanisms: How pertussis vaccines stimulate immunity against Bordetella pertussis
Pertussis vaccines, whether whole-cell (wP) or acellular (aP), harness the immune system’s adaptive machinery to protect against *Bordetella pertussis*. The key lies in antigen presentation: wP vaccines introduce inactivated bacteria, exposing the immune system to a broad array of bacterial components, while aP vaccines target specific antigens like pertussis toxin (PT), filamentous hemagglutinin (FHA), pertactin (PRN), and fimbriae. These antigens are recognized by antigen-presenting cells (APCs), which process and display them to T cells, initiating a cascade of immune responses. For instance, aP vaccines typically contain 5–20 µg of PT and 5–20 µg of FHA per dose, calibrated to elicit robust immunity without overwhelming the system.
The immune response to pertussis vaccines is both humoral and cell-mediated. Humoral immunity involves B cells producing antibodies, primarily IgG, which neutralize bacterial toxins and opsonize bacterial cells for phagocytosis. PT, a major virulence factor, is a prime target for neutralization. Studies show that anti-PT antibodies correlate strongly with protection, making it a critical component in aP vaccines. Cell-mediated immunity, driven by T helper cells (Th1 and Th2), is equally vital. Th1 cells activate macrophages to destroy intracellular bacteria, while Th2 cells support B cell antibody production. This dual mechanism ensures a comprehensive defense against *B. pertussis* colonization and toxin-mediated damage.
A critical challenge in pertussis vaccination is the waning immunity observed over time, particularly with aP vaccines. Unlike natural infection, which confers longer-lasting immunity, vaccine-induced responses decline within 5–10 years. This is partly due to the absence of certain bacterial components in aP vaccines and the lack of mucosal immune stimulation. Booster doses, such as the Tdap vaccine (10 µg PT, 5 µg FHA, 3 µg PRN), are recommended for adolescents and adults to maintain protective antibody levels. Practical tips include scheduling boosters every 10 years and ensuring timely vaccination of pregnant women (27–36 weeks gestation) to confer passive immunity to newborns.
Comparing wP and aP vaccines highlights their distinct immune profiles. wP vaccines, while highly effective, are associated with more adverse reactions due to their complex antigen composition. aP vaccines, introduced to improve safety, have a narrower antigen focus, which may contribute to their reduced efficacy over time. Research into next-generation vaccines, such as live attenuated or nasally administered formulations, aims to bridge this efficacy gap by mimicking natural infection and stimulating mucosal immunity. For example, a live attenuated vaccine candidate has shown promise in preclinical trials by inducing both systemic and mucosal immune responses, potentially offering longer-lasting protection.
In conclusion, pertussis vaccines stimulate immunity through a carefully orchestrated interplay of antigen presentation, humoral, and cell-mediated responses. Understanding these mechanisms underscores the importance of vaccine design and dosing strategies. While current vaccines provide substantial protection, ongoing innovations seek to enhance efficacy and durability. Practical steps, such as adhering to booster schedules and exploring novel vaccine platforms, are essential to combat the resurgence of pertussis and protect vulnerable populations.
BCP Bank's Global Reach: Exploring Its Extensive Network of Locations
You may want to see also
Explore related products




![]()
Efficacy in Different Populations: Vaccine effectiveness across age groups, including infants and adults
The pertussis vaccine's efficacy varies significantly across age groups, a critical factor in public health strategies. Infants, particularly those under 6 months, are at highest risk for severe complications, yet they cannot complete the full vaccination series during this vulnerable period. The bridge to efficacy here relies on maternal vaccination during pregnancy, which transfers protective antibodies to the fetus. This strategy has been shown to reduce pertussis cases in newborns by up to 91%, according to the CDC. However, this protection wanes by 2–3 months, emphasizing the urgency of initiating the infant DTaP series at 2 months, with subsequent doses at 4 and 6 months, followed by boosters at 15–18 months and 4–6 years.
In contrast, adolescents and adults often experience waning immunity years after their last Tdap dose, contributing to resurgence in pertussis outbreaks. Studies indicate that vaccine efficacy in adults drops to approximately 40–70% within 2–5 years post-vaccination. For this population, the bridge to efficacy involves timely Tdap boosters, ideally every 10 years or during pregnancy for women. Healthcare providers play a pivotal role in educating adults about the importance of these boosters, especially those in close contact with infants. Practical tips include integrating Tdap reminders into routine health check-ups and leveraging electronic health records to track vaccination status.
Comparing infant and adult responses highlights the need for tailored strategies. While infants rely on passive immunity from maternal antibodies and rapid primary series completion, adults require periodic boosters to maintain herd immunity. Interestingly, adolescents aged 11–18 years often receive Tdap as part of school requirements, achieving efficacy rates of 60–80% in the first year post-vaccination. This age group serves as a critical link in preventing transmission to younger siblings or infants. However, compliance remains a challenge, with only 89% of teens in the U.S. receiving Tdap by age 17, according to 2022 data.
A persuasive argument for universal adherence emerges when examining the societal impact of age-specific efficacy gaps. Unvaccinated or undervaccinated adults and adolescents act as reservoirs for pertussis, undermining efforts to protect infants. For instance, a 2019 California study found that 70% of infant pertussis cases were transmitted by household members, predominantly parents. Closing this gap requires not just individual action but systemic changes, such as workplace vaccination programs and public health campaigns targeting high-risk groups.
In conclusion, bridging the efficacy gap in pertussis vaccination demands age-specific approaches grounded in immunological science and behavioral insights. For infants, maternal vaccination and timely primary series are non-negotiable. Adults and adolescents must prioritize regular boosters, supported by healthcare infrastructure and community education. By addressing these disparities, we can fortify the protective barrier against pertussis across all populations.
Is M&T Bank FDIC Insured? Understanding Your Deposit Protection
You may want to see also
![]()
Waning Immunity Challenges: Decline in vaccine protection over time and booster recommendations
The effectiveness of the pertussis vaccine, while initially robust, diminishes over time, leaving individuals vulnerable to infection. This phenomenon, known as waning immunity, poses a significant challenge in maintaining herd immunity and preventing outbreaks. Studies have shown that protection against pertussis can decrease by 20-30% per year after the initial vaccination series, with adolescents and adults becoming particularly susceptible. For instance, a 2016 study published in *Pediatrics* found that the Tdap vaccine's efficacy dropped from 69% within the first year to 21% after 4 years in adolescents.
To address this decline, booster recommendations have been established to reinforce immunity. The Centers for Disease Control and Prevention (CDC) advises that adolescents receive a Tdap booster at age 11-12, while adults should get a Tdap booster once, followed by a Td or Tdap booster every 10 years thereafter. Pregnant women are also encouraged to receive a Tdap dose during each pregnancy, preferably between 27 and 36 weeks, to provide passive immunity to newborns, who are too young to be vaccinated and at highest risk of severe complications from pertussis.
However, adherence to booster recommendations remains suboptimal. Only about 30% of adults in the United States have received a Tdap booster, according to CDC data. Barriers such as lack of awareness, concerns about side effects, and limited access to healthcare contribute to this gap. To improve compliance, healthcare providers must emphasize the importance of boosters during routine visits and leverage reminder systems. Employers and schools can also play a role by offering on-site vaccination clinics and educational campaigns.
A comparative analysis of pertussis vaccination strategies reveals that countries with robust booster programs, such as Australia and the UK, have lower incidence rates than those with less stringent policies. For example, Australia’s introduction of a pertussis booster for adolescents in 2013 led to a 50% reduction in cases within two years. This underscores the critical role of timely boosters in sustaining immunity and controlling disease spread.
In conclusion, waning immunity to pertussis necessitates a proactive approach to booster vaccinations. By adhering to age-specific guidelines, raising awareness, and removing access barriers, individuals and communities can mitigate the risk of infection. Practical steps include scheduling booster shots during routine medical appointments, utilizing immunization registries to track vaccination status, and advocating for workplace or school-based vaccination initiatives. Addressing these challenges is essential to bridge the gap between initial vaccination and long-term protection, ensuring continued efficacy against pertussis.
Can Bank Transactions Be Hidden? Exploring Legality and Methods
You may want to see also
![]()
Global Vaccination Strategies: Efforts to reduce pertussis incidence through immunization programs
Pertussis, commonly known as whooping cough, remains a significant public health concern despite the availability of effective vaccines. Global vaccination strategies have evolved to address the persistent incidence of this highly contagious respiratory disease, leveraging innovative approaches like the "bridge to efficacy" concept. This strategy focuses on optimizing vaccine delivery and formulation to ensure robust and sustained immunity across diverse populations. By examining these efforts, we can identify key tactics that have proven effective in reducing pertussis cases worldwide.
One critical component of global vaccination strategies is the implementation of age-specific immunization schedules. For infants, the World Health Organization (WHO) recommends a primary series of three doses of diphtheria-tetanus-pertussis (DTP) vaccine, typically administered at 6, 10, and 14 weeks of age. This early vaccination is crucial, as infants are at highest risk of severe complications, including pneumonia and encephalopathy. Booster doses are then given during childhood and adolescence to maintain immunity. For example, the United States advises a DTaP (diphtheria, tetanus, and acellular pertussis) booster at 4–6 years, followed by a Tdap dose at 11–12 years. Such schedules create a "bridge" of protection, ensuring continuous immunity as the immune response wanes over time.
Another innovative strategy is the use of maternal immunization to protect newborns. Administering Tdap vaccine to pregnant women during the third trimester has been shown to transfer pertussis antibodies to the fetus, providing passive immunity during the first months of life. This approach has been widely adopted in countries like the United States, the United Kingdom, and Australia, significantly reducing pertussis-related hospitalizations in infants. For instance, studies indicate that maternal vaccination can prevent up to 91% of pertussis cases in newborns under 2 months old. This tactic not only bridges the immunity gap in early infancy but also complements the infant vaccination schedule.
However, challenges remain, particularly in low- and middle-income countries (LMICs) where vaccine access and infrastructure are limited. To address these disparities, global initiatives like Gavi, the Vaccine Alliance, have played a pivotal role in funding and distributing pertussis vaccines. Gavi’s support has enabled over 800 million children in LMICs to receive DTP vaccines since 2000. Additionally, efforts to strengthen cold chain systems and train healthcare workers have improved vaccine delivery in remote areas. These measures ensure that the "bridge to efficacy" is not just a theoretical concept but a practical reality for vulnerable populations.
A comparative analysis of high- and low-income countries reveals the impact of these strategies. Nations with robust immunization programs, such as the United States and Australia, have seen pertussis incidence decline by over 80% since the introduction of acellular pertussis vaccines in the 1990s. In contrast, LMICs with lower vaccination coverage continue to report higher disease burden. This underscores the importance of sustained investment in global vaccination efforts, including research into next-generation vaccines with longer-lasting immunity. By learning from successful models and adapting them to local contexts, the global health community can further reduce pertussis incidence and move closer to its eradication.
Mastering the Application: A Step-by-Step Guide to Landing a Bank Teller Job
You may want to see also
Frequently asked questions
The Bridge to Efficacy Pertussis Vaccine is a research approach used to assess the effectiveness of pertussis (whooping cough) vaccines by comparing immune responses in vaccinated individuals to those with natural immunity, rather than directly measuring disease prevention.
The Bridge to Efficacy concept is used for pertussis vaccines because conducting large-scale clinical trials to directly measure vaccine efficacy against disease is often impractical and unethical due to the high number of participants required and the need to expose them to the disease.
The Bridge to Efficacy approach determines pertussis vaccine effectiveness by correlating specific immune markers (e.g., antibody levels) in vaccinated individuals with those observed in people who have recovered from natural pertussis infection, assuming these markers are predictive of protection.